
Turmeric Extract Administration Increases the Expression of Brain
Derived Neurotropic Factor Following Repetitive Traumatic
Brain Injuries
Andre Marolop Pangihutan Siahaan
1*
, Iskandar Japardi
1
, Wismaji Sadewo
2
1
Department of Neurosurgery, Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia
2
Department of Neurosurgery, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia
Keywords: Repetitive Traumatic Brain Injuries; Turmeric Extract; BDNF.
Abstract: Objective: To demonstrate the role of turmeric extract administration in increasing Brain-Derived
Neurotrophic Factor (BDNF). Method: A model of repetitive traumatic brain injury was used on Sprague
Dawley mouse, using a 40-gr weight dropped onto the vertex from 1-m height with total frequency of
twelve times, divided into four days; three traumas every day. A 500 mg/kg turmeric extract was
administered per oral daily. BDNF expression was assessed using immunohistochemistry examination. As a
comparison, there were also negative sham control group and trauma only group. Result: There was no
significant difference in BDNF expression between the negative sham control group and trauma only group.
Instead, there was a significant increase in BDNF expression in the group with turmeric extract
administration. Conclusion: Turmeric extract administration increased BDNF expression following
repetitive traumatic brain injury.
1 INTRODUCTION
Even though the first long-term effect following
repetitive traumatic brain injury (RTBI) was
reported almost a century ago, it starts to be a
prominent issue in the last decade, especially after
Omalu reported this finding in American Football
(Omalu et al., 2005). This condition, termed Chronic
Traumatic Encephalopathy (CTE), is related to
disturbance of behavior, mood, cognitive, and motor
function (Montenigro et al., 2015). Following RTBI,
the brain will undergo progressive changes
consistent with degeneration process, with tau
protein as the main pathology (McKee et al., 2016).
CTE itself is still a disease of elusive, with varying
diagnostic criteria and no proved effective treatment
(Hay et al., 2016).
This problem becomes significant if we
consider that some people, such as contact sport
athletes (i.e., American football, soccer, and martial
arts) and military personals are prone to encounter
RTBI (McKee et al., 2009). In professional soccer
players, for instance, head impacts during playing
are various, dependent on the season, from four
times up to 125 times in two weeks. A post-mortem
examination in American football players confirmed
this hypothesis. A report showed that NFT was
found in most, if not all retired professional
American football players (Perrine et al., 2017).
RTBI itself will disturb ionic stability in the
neural cell. Following an impact, the released
glutamate will initiate hyperactivation of N-methyl-
D-aspartate (NMDA)-type receptors, burden the cell
with calcium, and induct neuroinflammation
(Guerriero et al., 2015). All of these processes will
lead to neuronal cell death. To overcome it,
neurotrophic factors, especially the brain-derived
neurotrophic factor (BDNF), will be released. BDNF
serves as a crucial mediator of neuronal plasticity
that will lead to neuronal remodeling, the formation
of new synapses, or new neurogenesis (Failla et al.,
2015). However, this response is lessened following
RTBI. Inflammatory cytokines that released
following RTBI seem to play a key role by reducing
the expression of BDNF (Kaplan et al., 2010). This
inhibition is not limited only to BDNF, but also to
other trophic factors, such as nerve growth factor
(NGF) and neurotrophin-3 (NT-3).
Siahaan, A., Japardi, I. and Sadewo, W.
Turmeric Extract Administration Increases the Expression of Brain Derived Neurotropic Factor Following Repetitive Traumatic Brain Injuries.
DOI: 10.5220/0009841200150018
In Proceedings of the 2nd International Conference on Tropical Medicine and Infectious Disease (ICTROMI 2019), pages 15-18
ISBN: 978-989-758-469-5
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
15
Turmeric (Curcuma longa) plants commonly
found in South and Southeast Asia. For centuries,
the rhizome of this plant has been used as a spice in
daily food and medicinal properties. Curcumin, its
active component, has been isolated for decades and
proved to have strong anti-inflammation activity
(Aggarwal et al., 2013). The aim of this study was to
demonstrate the effect of turmeric extract
administration on BDNF expression following
RTBI.
2 METHOD
2.1 Animal Model and Experimental
Groups
Thirty Sprague-Dawley young adult rats were
divided randomly into three groups, i.e., the negative
sham control group, trauma-only group, and
turmeric group. Total traumas were twelve times,
divided into four days, i.e. on day 1, 2, 4, and 7, with
a no-trauma period on day 3, 5, and 6. This timing
was carried out to resemble the real condition in
sports. Trauma was applied using a weight model
drop, by dropping a 40-gr mass from 1-meter height
onto the vertex. A metal helmet was put on the
vertex to prevent skull fracture (Xu et al., 2016).
This protocol was approved by the Medical
Research Committee, Medical Faculty Universitas
Sumatera Utara, Medan, Indonesia.
2.2 Turmeric Extract Supplementation
A commercially available turmeric extract (Sido
Muncul, curcumin 18.02%) was given orally with
500 mg/kg dose daily to rats in the turmeric group.
2.3 Brain Extraction
Decapitation was done using sharp scissors. Ether
was used as an anesthetic agent. Craniotomy was
performed started posteriorly from the foramen
magnum to the anterior, without preservation of the
olfactory bulb. A 10% formalin buffer solution was
used as a fixation agent.
2.4 Immunohistochemistry
Examination and Cell Count
A 4-micron paraffin block was stained using BDNF
antibody (Abcam). Brown-stained nuclear was
counted as positive. The observation was carried out
using cell count in twenty visual fields at the cortex
of the vertex with magnification 400 times.
2.5 Statistical Analysis
Values were expressed as means SEM. The results
were computed statistically using the independent t-
test. A difference was considered significant at the p
<0.05 level.
3 RESULTS
3.1 Mortality and Body Weight Change
There was no mortality found in this protocol, either
in the negative sham control group, trauma only
group, and turmeric group. There was also no
significant difference regarding body weight before
and after protocols in all three groups (table 1).
Table 1: Change of body weight before and after the
protocol
Group
Before protocol
After protocol p
Negative
sham
377.22 29.72
378.44 29.66
0,910
Trauma 351.78 29.89 349.33 38.90 0,482
TE 367.89 36.70 357.89 39.89 0,950
*paired t-test. Significant if p<0.05.
3.2 BDNF Expression
Compared to the negative sham control group, there
was no significant change in BDNF expression
following RTBI (p=0.999). BDNF expression in the
turmeric group was significantly higher compared to
negative sham (p=0.021) and trauma only group
(p=0.007; figure 1)
ICTROMI 2019 - The 2nd International Conference on Tropical Medicine and Infectious Disease
16
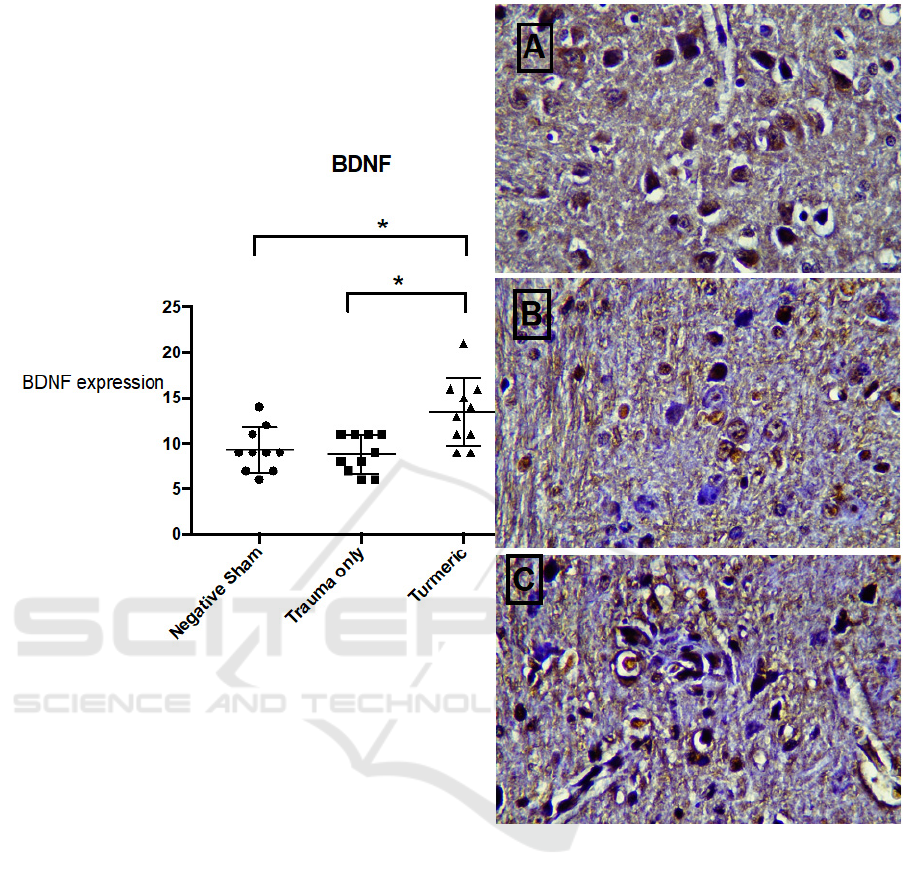
Figure 1: BDNF expression in the negative sham control group (A), trauma only group (B), and turmeric group (C). The
significant difference was found between the turmeric group and trauma only group as well as between the turmeric group
and negative sham control group. BDNF: Brain Derived Neurotropic Factor. *significant.
4 DISCUSSION
To the date, there was no generally accepted
protocol that can reproduce the situation in RTB in
contact sport athletes. The protocol used in this
research itself was considered as "mild" TBI, even
there are no diagnosis criteria of concussion in the
rat (Xu et al., 2016). Even though, we had shown no
change in BDNF expression following RTBI. BDNF
acts in secondary injury caused by a combination of
inflammation, ischemia, cytotoxic process, and
apoptosis. Several experimental studies on rat had
shown an increase in hippocampal BDNF mRNA
days after moderate-severe TBI. Another study
showed
that BDNF level would decrease in 24 hours
following TBI, but not significant again after 36
hours (Yang et al., 2009).
We also found an increase in BDNF
expression following turmeric administration.
Curcumin is shown to be a potent anti-inflammatory
agent in an animal model of TBI. BDNF expression
is affected by inflammation (Failla et al., 2015). The
mRNA levels of BDNF on hippocampal were
reduced following administration of interleukin.
Even so, the inflammatory response itself is very
Turmeric Extract Administration Increases the Expression of Brain Derived Neurotropic Factor Following Repetitive Traumatic Brain
Injuries
17

crucial in neural remodeling process and recovery. It
makes neuroinflammation is not the only pathway
that should be restricted in treating TBI (Lyman et
al., 2014).
To the best of our knowledge, this is the first
research that demonstrates the effect of turmeric on
BDNF expression following RTBI. The main
limitation of this research was no evaluation of the
status of neuroinflammation itself, even regarding
proinflammatory cytokines or either astrogliosis or
microglia activation. This aspect can be evaluated in
further research.
5 CONCLUSION
Turmeric extract administration increased BDNF
expression following repetitive traumatic brain
injury.
ACKNOWLEDGMENT
This study was funded by Universitas Sumatera
Utara in TALENTA Grant. Authors also thanked
Widi Riawan from Department of Biochemistry,
Faculty of Medicine, Universitas Brawijaya,
Malang, Indonesia, for the help in conducting this
study.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
REFERENCES
Aggarwal BB, Gupta SC, Sung B. Curcumin: an orally
bioavailable blocker of TNF and other pro-
inflammatory biomarkers. 2013. British Journal of
Pharmacology, 169(8),1672–92.
Failla MD, Conley YP, Wagner AK. Brain-Derived
Neurotrophic Factor (BDNF) in Traumatic Brain
Injury-Related Mortality.2015. Neurorehabil Neural
Repair, 30(1), 83–93.
Guerriero RM, Giza CC, Rotenberg A. Glutamate and
GABA Imbalance Following Traumatic Brain Injury.
2015. Curr Neurol Neurosci Rep, 15(5), 27–11.
Hay J, Johnson VE, Smith DH, Stewart W. 2016. Chronic
Traumatic Encephalopathy: The Neuropathological
Legacy of Traumatic Brain Injury. Ann Rev Pathol,
11(1), 21–45.
Kaplan GB, Vasterling JJ, Vedak PC. Brain-derived
neurotrophic factor in traumatic brain injury, post-
traumatic stress disorder, and their comorbid
conditions: role in pathogenesis and treatment. 2010.
Behavioral Pharmacology, 21(5-6), 427–37.
Lyman M, Lloyd DG, Ji X, Vizcaychipi MP, Ma D.
Neuroinflammation: The role and consequences. 2014.
Neuroscience Research, 79, 1–12.
McKee AC, Alosco ML, Huber BR. Repetitive Head
Impacts and Chronic Traumatic Encephalopathy.
2016. Neurosurg Clin N Am, 27(4), 529–35.
McKee AC, Cantu RC, Nowinski CJ, Hedley-Whyte ET,
Gavett BE, Budson AE, et al. Chronic Traumatic
Encephalopathy in Athletes: Progressive Tauopathy
After Repetitive Head Injury. 2009. Journal of
Neuropathology & Experimental Neurology, 68(7),
709–35.
Montenigro PH, Bernick C, Cantu RC. 2015. Clinical
Features of Repetitive Traumatic Brain Injury and
Chronic Traumatic Encephalopathy. Brain Pathol,
25(3), 304–17.
Omalu BI, DeKosky ST, Minster RL, Kamboh MI,
Hamilton RL, Wecht CH. 2005. Chronic Traumatic
Encephalopathy in a National Football League Player.
Neurosurgery, 57(1),128–34.
Perrine K, Helcer J, Tsiouris AJ, Pisapia DJ, Stieg P. The
Current Status of Research on Chronic Traumatic
Encephalopathy. 2017. World Neurosurg 102, 533–44.
Xu L, Nguyen JV, Lehar M, Menon A, Rha E, Arena J, et
al. Repetitive mild traumatic brain injury with impact
acceleration in the mouse: Multifocal axonopathy,
neuroinflammation, and neurodegeneration in the
visual system. 2016. Experimental Neurology,
275(Part 3), 436–49.
Yang J, Siao C-J, Nagappan G, Marinic T, Jing D,
McGrath K, et al. 2009. Neuronal release of
proBDNF. Nat Neurosci, 12(2),113–5.
ICTROMI 2019 - The 2nd International Conference on Tropical Medicine and Infectious Disease
18
