
Analysis of Factors Relating to the Event of Dyslipidemia in Oil and
Gas Workers
Putri Handayani and Fierdania Yusvita
Department of Public Health, Universitas Esa Unggul, Jl. Arjuna Utara No 9, Jakarta, Indonesia
Keywords: Dyslipidemia, Occupational Health, HDL, Cholesterol, Work Promotion.
Abstract: Dyslipidemia is a health disorder that is often found in workers in the oil and gas mining industry. Workers
have a huge potential to experience the risk of cardiovascular disease because several factors in the work
environment can affect health. The purpose of this study was to determine the factors associated with the
incidence of dyslipidemia in workers at PT X. This research method uses a cross-sectional study. The
population of this study is the workers who served on Ship A, amounting to 45 people. The statistical test
used is the Chi-Square test. Based on the results of the study found that, there is no relationship of LDL (p-
value = 1,000), triglycerides (p-value = 0.135), BMI (p-value = 1,000), smoking status (p-value = 0.704),
hypertension status (p-value = 0.699) with the incidence of dyslipidemia and there is a relationship between
HDL (p-value = 0.006), obese (p-value = 0,025) and cholesterol (p-value = 0.001) with the incidence of
dyslipidemia. Researchers suggest that companies are expected to be able to revitalize work promotion
programs in the workplace.
1 INTRODUCTION
Dyslipidemia is a disorder of lipoprotein metabolism
in the form of overproduction or lipoprotein
deficiency. This disorder can be manifested by an
increase in total serum cholesterol (TC), low-density
lipoprotein cholesterol (LDL-C), and triglyceride
concentrations, and a decrease in lipoprotein protein
(HDL-C) high-density concentration. This is a major
risk factor for coronary heart disease (CHD), the
leading cause of death worldwide (American Heart
Association, 2004).
The Increasing prevalence of dyslipidemia has
become a worldwide public health problem (Qi et
al., 2015). Dyslipidemia occurs due to several
factors one of which is lifestyle changes.
Dyslipidemia can be experienced by anyone without
knowing a social or educational status. Dyslipidemia
can cause several effects on workers such as type 2
diabetes (Jayarama and Lakshmaiah, 2012; Zhou et
al., 2014), atherosclerosis (Snehalatha et al., 201),
stroke (Djelilovic-Vranic et al., 2013) and
cardiovascular diseases (Stamler et al., 2000;
Vergani and Lucchi, 2012). Factors that trigger
dyslipidemia include age (WHO, 2007), smoking
(WHO, 2007), body mass index (WHO, 2007;
Basheikh, 2016), hypertension (Lopez, 2006), HDL,
LDL, triglycerides, and total cholesterol (Basheikh),
2016).
PT. X is a company engaged in the oil and gas
sector. The results of research conducted at this
company in 2017 showed that the proportion of
workers with dyslipidemia status was 82.2% with
the total workers at risk of cardiovascular disease of
51.1%. Until 2008 it was reported that cases of death
due to Coronary Heart Diseases (CHD) increased by
30% in this company. Furthermore, in 2009 it was
reported that the proportion of active workers who
died due to CHD at PT X was as much as 40%.
Based on the results of periodic health checks
conducted at the company, in 2004-2016 there was
an increase in risk factors for dyslipidemia such as
BMI, cholesterol, and glucose above the normal
limit in workers. The proportion of workers with
high total cholesterol (>200 mg/dL) was 64.1%,
workers with a BMI >25 kg/m2 were 42.3%, and
workers with impaired glucose were 13.8%. Also, as
many as 7.3% of workers have a history of
hypertension (blood pressure >140/90 mmHg) and
43.2% of workers are active smokers (Health Dept.
PT X, 2016). Therefore, this study aimed to
determine the factors associated with the incidence
of dyslipidemia in workers at PT X.
Handayani, P. and Yusvita, F.
Analysis of Factors Relating to the Event of Dyslipidemia in Oil and Gas Workers.
DOI: 10.5220/0009594903170319
In Proceedings of the 1st International Conference on Health (ICOH 2019), pages 317-319
ISBN: 978-989-758-454-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
317
2 METHOD
This quantitative research uses a non-experimental
design. The sample of this research is 45 workers
who are all workers who work on Ship A. Data
collection is done cross-sectionally using secondary
data. Data analysis is performed using computer
software, univariate analysis is performed to see the
frequency distribution of each variable. research to
determine the variation of each variable, and
bivariate analysis to see the relationship between
independent and dependent variables. The statistical
test used was chi-square with a significance level of
0.05.
3 RESULT
Table 1: Distribution of respondent characteristics and risk
factors for dyslipidemia.
Variable Categories n %
Dyslipidemia Yes 37 82,2
No 8 17,8
Ages >48 Years old 22 48,9
<48 Years old 23 51,1
Obese Obese 25 55,6
Normal 20 44,4
Smoking Yes 26 57,8
No 19 42,2
Hypertension Yes 30 66,7
No 15 33,3
LDL Low 22 48,9
High 23 51,1
HDL Low 22 48,9
High 23 51,1
Triglyceride Normal 22 48,9
High 23 51,1
Total
Cholesterol
Low 22 48,9
High 23 51,1
In this study, the proportion of workers with
dyslipidemia was 82.2%. Based on workers aged
<48 years 51.1%, abnormal BMI 55.6%, smoking
57.8%, hypertension 66.7%, high LDL 51.1%, high
HDL 51.1%, high triglycerides 51, 1%, and high
cholesterol 51.1% (see table 1).
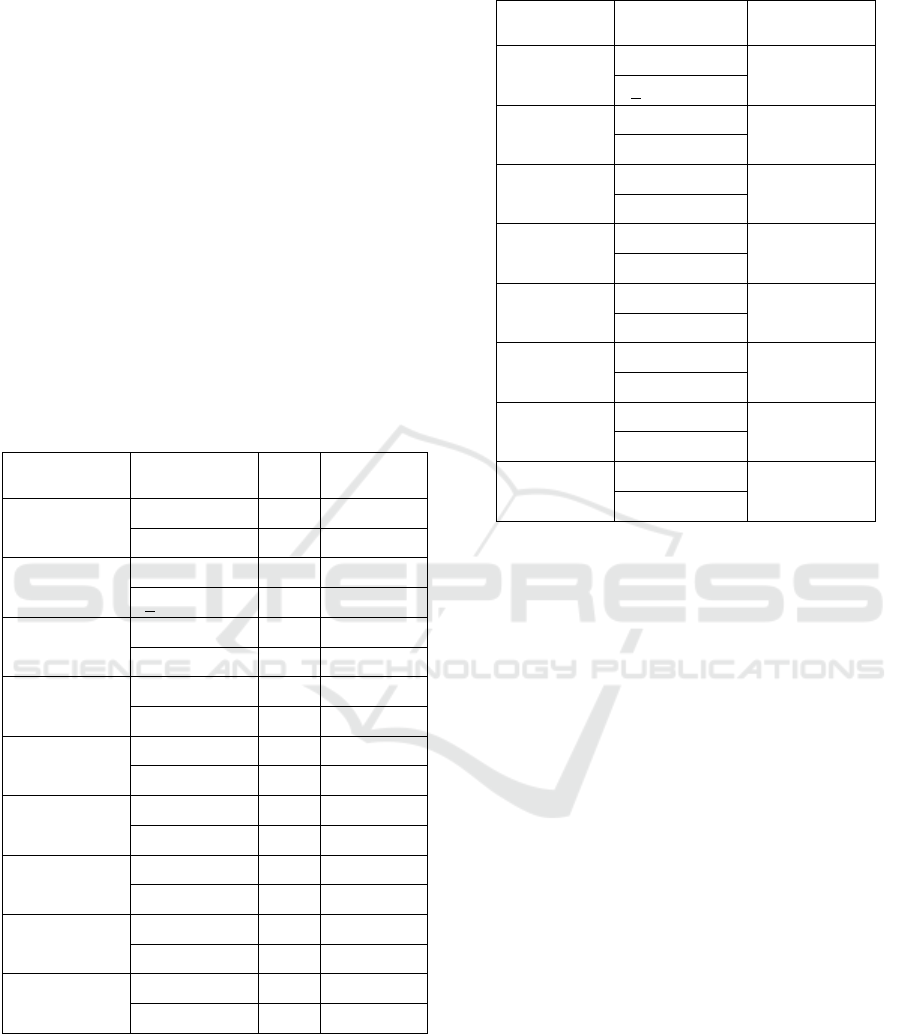
Table 2: Factors related to dyslipidaemia.
Variable Categories p-value
Ages >48 Years old 0,879
<48 Years old
Obese Obese 0,025
Normal
Smoking Yes 0,704
No
Hypertension Yes 0,699
No
LDL Low 1,000
High
HDL Low 0,006
High
Triglyserida Normal 0, 136
High
Total
Cholesterol
Low 0,001
High
Bivariate analysis results show that there is no
relationship of LDL (p-value = 1,000), triglycerides
(p-value = 0.136), smoking status (p-value = 0.704),
hypertension status (p-value = 0.699) with the
incidence of dyslipidemia and there is a relationship
between HDL (p-value = 0.006), obese (p-value =
0,025) and cholesterol (p-value = 0.001) with the
incidence of dyslipidemia (see table 2).
4 DISCUSSION
The prevalence of dyslipidemia continues to
increase in some developing countries (Fuentes et
al., 2003). In this study, the prevalence of
dyslipidemia in oil and gas company workers
reached 82.2%. The high prevalence of dyslipidemia
can be caused by changes in worker lifestyle,
especially such as lack of physical activity (Hirai, et
al., 2019), smoking habits and unhealthy food intake
(Basheikh, 2016).
The results of the bivariate analysis show there is
a relationship between obesity status and
dyslipidemia status with the risk of cardiovascular
disease. This is in line with the theory revealed by
WHO (2007) that obesity is a health problem that
develops in both developed and developing
countries. Prospective epidemiological studies have
shown an association between being overweight or
ICOH 2019 - 1st International Conference on Health
318

obese and cardiovascular morbidity, CVD mortality
and total mortality. Obesity is strongly associated
with cardiovascular risk factors, such as raised blood
pressure, glucose intolerance, type 2 diabetes, and
dyslipidemia. A meta-analysis of RCTs has shown
that reducing weight-diet, combined with exercise,
results in significant body weight, reducing total
cholesterol and LDL cholesterol, increasing HDL-
cholesterol, and improving blood pressure control
and diabetes.
Based on the Chi-Square test, smoking status
does not have a significant relationship with the risk
of cardiovascular disease in workers at PT X. This is
because smoking can cause changes in the structure
and function of blood circulation in the body.
According to WHO (2007), Smoking is a major risk
factor for heart disease, including heart attacks and
strokes, and also has a strong relationship with CHD
so stopping smoking will reduce the risk of a heart
attack. Cigarette smoking increases the risk of heart
attack 2 to 3 times. About 24% of deaths due to
CHD in men and 11% in women due to smoking.
Despite a progressive decline in the proportion of
the population who smoked since the 1970s, in 1996
29% of men and 28% of women still smoked. One
thing of concern is the increased prevalence of
smoking in adolescents, especially in adolescent
girls. People who do not smoke and live with
smokers (passive smokers) have an increased risk of
20-30% compared to people who live with
nonsmokers. The risk of developing CHD due to
smoking is related to a dose where people who
smoke 20 or more cigarettes a day have a risk of two
to three times higher than the general population to
experience CHD events (WHO, 2007).
The results of the bivariate analysis showed that
age was not related to the risk of cardiovascular
disease. This is contrary to what was expressed by
Djohan (2004) that the risk of cardiovascular disease
will increase with age. In this study, the age factor
becomes unrelated, possibly due to other factors that
have a stronger influence compared to the age factor.
5 CONCLUSIONS
Based on the results of the analysis, related factors
are factors that can be prevented by adopting a
healthy lifestyle at work. Companies are advised to
re-activate health promotion programs, especially in
work areas such as Ship A. This needs to be done so
that the triggering factors for cardiovascular disease
can be controlled properly. Further research is
needed to find out the most dominant factor
influencing the risk of cardiovascular disease in
workers in similar industries.
REFERENCES
Basheikh, K., et al., 2016. Prevalence of dyslipidemia and
its associated factors among employees of primary
health care centers, Jeddah, Saudi Arabia.
International Journal of Medical Science and Public
Health 2016; 5(05): 946–951.
Djelilovic-Vranic, J.; Alajbegovic, A.; Zelija-Asimi, V.;
Niksic, M.; Tiric-Campara, M.; Salcic, S.; Celo, A.
Predilection role diabetes mellitus and dyslipidemia in
the onset of ischemic stroke. Med. Arch. 2013, 67,
120–123.
Djohan, T. Bahri Anwar, 2004., “Penyakit Jantung
Koroner dan Hypertensi”, Fakultas Kedokteran
Universitas Sumatera Utara, Sumatera Utara.
Fuentes R, Uusitalo T, Puska P, Tuomilehto J, Nissinen A.
Blood cholesterol level and prevalence of
hypercholesterolaemia in developing countries: a
review of population-based studies carried out from
1979 to 2002. Eur J Cardiovasc Prev Rehabil
2003;10(6):411–9.
Jayarama, N.; Lakshmaiah, M.R. 2015. Prevalence and
pattern of dyslipidemia in type 2 diabetes mellitus
patients in a rural tertiary care centre, southern India.
Glob. J. Med. Public Health 2012, 1, 24–27.
Lopez AD et al., 2006. Global and regional burden of
disease and risk factors, 2001: systematic analysis of
population health data. Lancet 2006, 367
(9524):1747–57.
Qi, Li., et al., 2015. Prevalence and Risk Factors
associated with Dyslipidemia in Chongqing, China.
International Journal of Environmental Research and
Public Health 2015; 12: 13455–13465.
Snehalatha, C.; Nanditha, A.; Shetty, A.S.; Ramachandran,
A. 2011. Hypertriglyceridaemia either in isolation or
in combination with abdominal obesity is strongly
associated with atherogenic dyslipidaemia in Asian
Indians. Diabetes Res. Clin. Pract. 2011, 94, 140–145.
Stamler, J.; Daviglus, M.L.; Garside, D.B.; Dyer, A.R.;
Greenland, P.; Neaton, J.D. 2000. Relationship of
baseline serum cholesterol levels in 3 large cohorts of
younger men to long-term coronary, cardiovascular,
and all-cause mortality and to longevity. JAMA 2000,
284, 311–318.
Vergani, C.; Lucchi, T. 2012. Plasma HDL cholesterol
and risk of myocardial infarction. Lancet 2012, 380,
1989–1990.
World Health Organization, 2007. Prevention of
cardiovascular disease: guidelines for assessment and
management of total. Genewa.
Zhou, X.; Zhang, W.; Liu, X.; Li, Y. 2014. Interrelationship
between diabetes and periodontitis: Role of
hyperlipidemia. Arch. Oral. Biol. 2014, 60, 667–674.
Analysis of Factors Relating to the Event of Dyslipidemia in Oil and Gas Workers
319
