
Mental Health Understanding from Culture Perspective: A Study of
Lay People Mental Health Literacy
Lina Cuwandayani and Anita
Novianty
Faculty of Psychology, Universitas Kristen Krida Wacana (UKRIDA),
Jl. Tanjung Duren Raya No.4, Jakarta Barat, Indonesia
Keywords: Chinese, Culture, Depression, Lay People, Mental Health Literacy, Schizophrenia.
Abstract: The gap between the prevalence and the access to professional treatment of mental disorder was one of the
biggest problems that acknowledged by health professionals. Low in mental health literacy was one of the
factors that contributed to prohibiting lay people to seek help. Culture has to get more attention in mental
health discussion because it is probably related to mental health literacy aspects such as mental disorder
recognition, belief about the cause of the mental disorder, stigma, even the help-seeking. In this study, we
want to explore the mental health understanding from the sample of Chinese people's perspectives in
Jakarta, Indonesia. The participants in this study were 130 people consisted of 85 women, 45 men (ranged
14-65 years old). The instruments to collect data in this study were two vignettes (depression and
schizophrenia). The method to measure data was descriptive analysis. The result showed the mental health
literacy of Chinese lay people was low, where Chinese culture mainly contributed to constructing beliefs
about the cause of the mental disorder and the decision to seek help. This study implied the study of mental
health should consider the culture to arrange a better mental health literacy program and help-seeking
system.
1 INTRODUCTION
Jorm (2000) introduced mental health literacy as
public knowledge and beliefs about mental disorder,
which consisted of recognition or labeling mental
disorder; (b) The knowledge and belief about the
cause of mental disorder; (c) The knowledge and
belief about self-help and professional help’s belief;
(d) and stigma towards mental disorder.
Some studies showed a trend that mental health
literacy in developing countries relatively low
compared to developed countries (Loo & Furnham,
2012; Kim et al., 2006; Wong et al., 2017). The
culture was one factor that related to symptoms
recognition, belief about the cause and the way to
seek help related to mental disorder. The concept of
mental health from the Western perspective
probably unacceptable in some non-western
countries because of the cultural tradition that would
be a proximal cause for the lack of ability to
recognize the symptoms (Novianty & Hadjam,
2017).
Race, ethnicity, and religion have a strong impact
on individual health and well-being. The cultural
background is important to be considered because
the concept of mental health was intertwined by
context, individual and the cause of the problem.
Mental disorders, such as depression, anxiety,
dissociative symptoms have a broader explanation
from a cultural perspective that was not seen as
health problems, instead of the challenge of
individual, morality issue, or disharmony between
family or community (Kirmayer & Swartz, 2014).
The severe mental disorder was considered a
problem in every culture, but it was addressed as
different perspectives that usually related to religion,
spirituality, and morality issue (Kirmayer &
Bhugra, 2009). Therefore, global mental health
should address the common mental disorder not
separated from diverse psychosocial context. Most
recognition or labeling of mental disorders could be
found in any kind of label, culture and diverse ways
of seeking help (Jacob & Patel, 2014).
Chinese culture in Indonesia has experienced
acculturation. Amanah, Bahari, and Fatmawati
(2014) studied the acculturation between Chinese
and Malay in Pontianak in terms of languages is
syncretistic, because of the Chinese Language in
304
Cuwandayani, L. and Novianty, A.
Mental Health Understanding from Culture Perspective: A Study of Lay People Mental Health Literacy.
DOI: 10.5220/0009594703040309
In Proceedings of the 1st International Conference on Health (ICOH 2019), pages 304-309
ISBN: 978-989-758-454-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
Indonesia was not only Mandarin but also had the
other four languages, such as Hokkien, Hakka, Teo-
Chiu, Kanton. Therefore, Chinese in Indonesia has a
significant difference between one another because
they have their own language that probably was not
understood by others. Currently, Chinese in
Indonesia was divided into two categories namely
Tionghoa Totok and Tionghoa Peranakan (Tan,
2008).
Chinese’s traditional concept about mental
health was encouraging Chinese people to
emphasize self- development to control the emotion,
to avoid interpersonal conflict and to maintain
harmony with other people. The great philosophers,
such as Confucius, were strongly influenced by
Chinese ideology and culture. Confucius taught
eight dharma virtues ”八德” (pinyin: Bā dé), such as
“孝”(pinyin: Xiào), means filial piety, “悌” (pinyin:
Tì) means humble, “忠” (pinyin: Zhōng) means
loyalty, “信” (pinyin: Xìn) means trustworthy, “禮”
(pinyin: Lǐ) means manner, “義” (pinyin: Yì) loyal
friends, “廉” (pinyin: Lián) means sincere heart, “恥
” (pinyin: Chǐ) means introspective. Chinese people
believed that people with a mental disorder was a
shame for family or having bad Fēngshuǐ. Family is
very essential in Chinese culture, not only as basic
social organization but also as a support to solve the
problem. Family is an important aspect related to
individual mental health (Tseng, Lin, & Yeh, 1995).
Traditional Chinese medicine based on the
concept of Yin and Yang, which formulated an
internal mechanism that works in the human body.
The understanding of health from traditional Chinese
medicine based on harmony between Yin and Yang
(Yip, 2003). Some Chinese people more prefer to
seek help from a traditional healer, drink herbal
medicine and tonic to cure the sickness rather than
finding psychosocial intervention and professional
help (Yip, 2003).
Most of the research about mental health literacy
currently constructed by Western perspectives,
especially according to the psychiatry field (Jorm,
2000; Kutcher, Wei, & Coniglio, 2016). Similar to
them, research about mental health literacy in
Indonesia also emphasized psychiatry definition to
measure the knowledge and belief about the
label, the cause of mental disorder and help-seeking.
The aim of this study was to measure mental health
literacy according to the mental health literacy
concept by Jorm (2000), as well as explore more the
intertwined Chinese culture perspective in each
aspect of the mental health literacy concept.
2 METHOD
The quantitative approach was applied in this study
with descriptive analysis. Two vignettes
(depression & Schizophrenia) were used as
instruments in which adapted from Jorm (2000), to
explore the recognition, belief about the cause of the
mental disorder, the way to help people with mental
disorders and stigma. Data were collected by an
online questionnaire using google form which
consisted of informed consent, personal information,
depression and schizophrenia vignettes following
eight questions of mental health literacy aspects.
2.1 Participants
Participants were Chinese adolescents (aged 14-22
years old, n=76) and Chinese adults (aged 23-65
years old, n=54) that were recruited by snowball
sampling technique. Participants who were filled
online questionnaires (n=130; 45 females; 85 males)
which consisted of Hakka/Khe (n=41), Kanton
(n=2), Hokkian (n=40), Tiochiu (n=9), dan
Peranakan (n=52).
2.2 Research Instrument
The vignettes that were used in this study was an
adapted story about the mental disorder (depression
and schizophrenia) that have been translated into the
context of Chinese people in Jakarta, Indonesia. The
questions that were following the vignettes consisted
of the aspect of mental health literacy by Jorm
(2000). The vignettes were validated with four
experts to confirm if all symptoms already fulfilled
the diagnostic criteria in DSM-V, then Aiken’s
V was applied to check the validity of all vignettes
that were used in this study.
Table 1: Aiken’s V Value for All Vignettes.
Type of Vignettes Aiken-V Conclusion
Depression Vignette for
Adolescent
0,625 Valid
Schizophrenia Vignette for
Adolescent
0,875 Valid
Depression Vignette for
Adult
0,625 Valid
Schizophrenia Vignette for
Adolescent
0,750 Valid
Mental Health Understanding from Culture Perspective: A Study of Lay People Mental Health Literacy
305
2.3 Data Analysis
Data were coded into some categories according to
previous literature, then descriptive statistics in
percentage was applied in every theme.
3 RESULT
In this study, 130 data were collected in which
divided into adolescent groups and adult groups.
Data consisted of participant’s responses in each
aspect of mental health literacy.
3.1 Recognition of Mental Disorder
In the adolescent group, participants who are able to
recognize and give the psychiatric label correctly for
depression vignette (56.6%) were higher than for
schizophrenia vignette (27.6%). In the adult group,
most participants are able to recognize of psychiatric
label correctly for depression vignette (38.8%)
but are not able to recognize the schizophrenia
vignette with a psychiatric label correctly (59.2%).
Table 2: Recognition of Mental Disorder.
Themes
Adolescent Adult Group
Group
D S D S
(%) (%) (%) (%)
Correct Psychiatric Label 56.6 27.6 38.8 1.8
Incorrect Psychiatric 13.2 42.1 35.1 59.2
Label
Incorrect Label 30.2 29.0 26.1 39.0
Not know 0 1.3 0 0
Notes: D: Depression; S: Schizophrenia
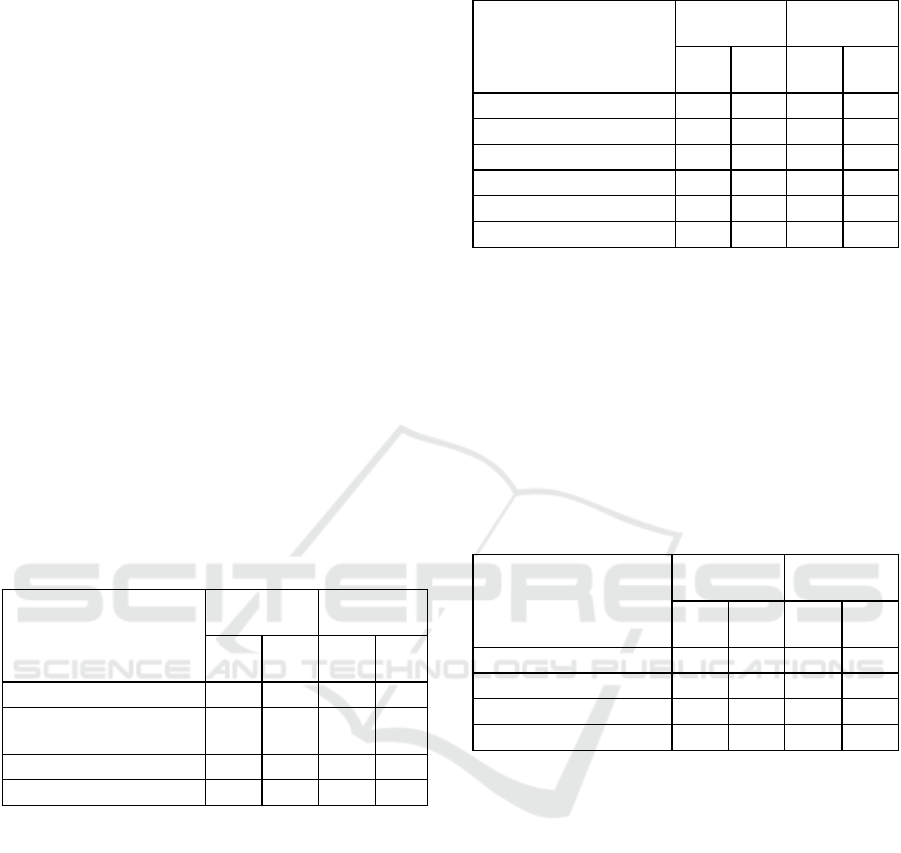
3.2 The Belief about the Cause of
Mental Disorder
In explaining the cause of the mental disorder, most
participants in the adolescent group focus on
personal factors as the cause of depression (60.6%)
and schizophrenia (65.7%). It is really similar to the
adult group that most participants tend to focus on
personal factors in explaining the cause of
depression (68.5%) and schizophrenia (63%) as
well. The personal factor such as lack of doing a
ritual, lack of pray, lack of wise seems related to the
culture of participants and the paradigm of well-
being in Chinese culture, which is social support,
especially family as the main value in Chinese
culture.
Table 3: The Cause of Mental Disorder.
Themes
Adolescent
Group
Adult Group
D
(%)
S
(%)
D
(%)
S
(%)
Social 35.5 19.7 24 24.1
Personal 60.6 65.7 68.5 63
Biological 1.3 1.3 2 0
Mystical 1.3 9.2 0 9.2
Not know 1.3 0 0 0
Unidentified 0 4.1 5.5 3.7
Notes: D: Depression; S: Schizophrenia
3.3 Help-seeking
Most participants in the adolescent group try to seek
help informally for depression vignette (80.3%), and
it was higher than the schizophrenia vignette
(42.1%). Interestingly, it also similar to the adult
group in which most participants try to seek help
informally for depression vignette (88.8%) and
schizophrenia vignette (55.6%) as well.
Table 4: Help-seeking of Mental Disorder.
Themes
Adolescent
Group
Adult Group
D
(%)
S
(%)
D
(%)
S
(%)
Formal 17.1 39.5 10.1 31.5
Semi-formal 1.3 15.8 1.1 11.1
Informal 80.3 42.1 88.8 55.6
Unidentified 1.3 2.6 0 1.8
Notes: D: Depression; S: Schizophrenia
3.4 The Attitude towards People with
Mental Disorder
In this aspect, we want to explore the attitude of
laypeople towards people with depression and
schizophrenia. It was found out that most
participants are willing to be friends with people in
depression vignette (97.4%) in the adolescent group
and (100%) in the adult group with familial bonding
as the main reason. Whereas, around 42.5% of
participants in the adult group are willing to be close
with people in schizophrenia vignette. The
stigma for schizophrenic people such as dangerous,
uncontrollable, able to attack, stink, unorganized
look are the main reason for participants are not
willing to be close with them.
ICOH 2019 - 1st International Conference on Health
306

3.5 Public Opinion about People with
Mental Disorder
In this aspect, we want to explore how participants
perceive what other people think and feel about the
individual with depression and schizophrenia. In the
adolescent group, most participants perceive people
will give labels toward people in depression vignette
as a common label such as stress (15.7%). They
think the other people will consider depressive
symptoms as an introvert, weird, and weak. Whereas
people with schizophrenia will be considered as
crazy (37%), mental illness (16.6%), annoying
(12.9%), weird (11.1%), possessed by the spirit
(1.8%), and feeling fear (15.1%).
3.6 Chinese’s Perspective in Mental
Health Literacy
In the recognition of the mental disorder, there is a
participant using Mandarin Language to respond to
depression vignette, such as 神情病 (pinyin:
Shénjīngbìng, which means neurotic. In the belief
about the cause of the mental disorder aspect, the
absence of social support, such as family and close
friend support was perceived as the cause of the
mental disorder. It was related to Chinese value that
prioritizes family support as one of the factors of
individual well-being. Other causes were related to
eight dharma virtues that were taught by Confucius
such as lack of worship, lack of discipline, and
untrustworthy. In a help-seeking aspect, for
depression vignette, participants tend to seek help
from a traditional healer (such as tabib, sinshe, thiau
tang, monks), drinking hu water, go to biokong,
drink herbal, praying in Vihara, or fengshui. In
Schizophrenia vignette, participants also tend to
seek informal help-seeking, such as doing kwamia,
lokthung worship, go to Biku or monks.
4 DISCUSSION
Mental health literacy of Chinese people in this
study was low in both groups (adolescent and adult).
It was indicated by the lack of recognition of the
mental disorder, the belief about the cause of mental
disorder that mostly explained by the personal
factor, informal help-seeking that was mostly
accessed, as well as the stigma that was perceived by
participants toward people with a mental disorder.
Even though participants in the adolescent group
tend to recognize depression vignette with
psychiatric labels correctly, rather than the adult
groups which tend to lack recognition of psychiatric
labels for depression and schizophrenia vignette.
Chinese in Indonesia has been assimilated with
other cultures that affect their perception and
behavior in daily life. The recognition of depression
and schizophrenia from the Chinese perspective
mostly used common labels. There are some labels
in the Chinese Language to describe people with
mental disorder such as 神經病 (pinyin:
Shénjīngbìng; translation: neurotic) which has a
negative connotation in daily life.
According to DSM-V, there are multiple causes
for depression such as genetics, childhood trauma,
medical condition, brain structure and function,
psychosocial, drugs and alcohol consumption.
However, participants in both groups of this study
tend to explain the cause of the mental disorder
(depression and schizophrenia vignette) by personal
factors. It seems related to the Confucius as a source
of guidance for Chinese people about the way of
living in daily life. Family support was the main
factor for Chinese people that indirectly having an
important role in Chinese people’s mental health
model (Tseng, Lin, & Yeh, 1995).
The lack of mental disorder recognition as a
psychiatric issue and the belief about the cause of
mental disorder by the personal factor directed
participants to seek informal help rather than
professional help. This finding is comparable with
findings of similar studies conducted by Novianty
(2017), which also found out that public stigma was
higher in schizophrenia vignette rather than
depression vignette in both groups. There was a
discrepancy between the participant’s attitude and
participant’s perceived attitude of others toward
people with a mental disorder. Participant’s attitudes
toward people with mental disorders tend to
maintain a close relationship with them, on the other
hand, the participants' perceived others have a
negative attitude toward people with a mental
disorder.
Wong et al (2017) stated that culture has
important role in shaping the belief of the cause of
mental disorder and help-seeking. This study also
found out similar findings in which culture has an
important role in the explanation of the cause of the
mental disorder, such as family issues, social
pressure, not having close friends or mystical factors
such as possessed by ancestor’s spirit, the imbalance
between yin and yang. All those responses were
related to the Chinese’s value of social and family
support as part of the individual well-being. Even
Mental Health Understanding from Culture Perspective: A Study of Lay People Mental Health Literacy
307

there is one participant which identified the cause of
the mental disorder was being a minority.
The help-seeking from the Chinese’s perspective
that was found out in this study using ritual or
traditional healing. Some participants believed
amulet paper (hu) could heal a mental disorder.
Another belief was kuamia or suanming (算命;
pinyin: Suànmìng), which able to detect our health
and well-being by analyzing the date and time of
birth using shio (Qian, 2015). This method to be
believed could predict our health condition and
prevent from scarce diseases. Another belief was by
rituals such as lokthung. Informal help-seeking that
was mostly accessed by Chinese participants in this
study probably happened because Chinese is one of
the minorities ethnic in Indonesia. according to
Gopalkrishnan and Babacan (2015), the minority
ethnic tend to seek help for mental disorder issues to
informal help-seeking rather than the majority in a
country.
The role of culture in mental health (how
laypeople recognize, understand, belief about the
cause, type of help-seeking for mental disorder
issues) was a consequence of their cultural history,
racism, and even stigma towards culture
(Gopalkrishnan & Babacan, 2015). The way of lay
people in understanding the mental health model in
different ethnicities showed similarly result that
most indigenous participant in various ethnicities
hardly recognize, identify, analyze the cause and
seek to professional help because they will tend to
try to access their cultural narrative concept in
explaining the issue and seeking traditional healer
(El-Islam, 2008; Kpanake, 2018; Rochford, 2004;
Yip, 2003).
According to Kirmayer and Swartz (2014),
culture affects how people perceive, express, explain
the symptoms and interpret the cause of the
symptoms, the pattern of help-seeking, even
social stigma. There is a construct gap between how
laypeople understand the mental disorder issue and
the psychiatry field constructing the issue. It does
not necessarily mean one against another, yet we
have to understand both constructs to find a better
solution.
We also found out the gap between adolescent
and adult groups was significantly different in their
ability to recognize the vignette using the
psychiatric label. The adolescent group is able
recognizing the vignette using a psychiatric label
correctly than the adult group. Another point we
have to focus on the term “your family/close friend”
in vignette seems to affect the participant’s attitude
toward a person in depression and schizophrenia
vignette. Most participants are willing to maintain a
close relationship with him, because of familial
bonding.
This study implies that culture affects how lay
people, specifically in this study was Chinese
participants, addressing, interpreting the cause,
the way to seek help and stigma towards symptoms
expressed by people with a mental disorder.
Therefore, culture should be considered in
promoting the awareness of mental health issues,
even in diagnosing the mental disorder.
5 CONCLUSIONS
There is a discrepancy of knowledge and belief
about representative symptoms of depression and
schizophrenia between the psychiatric field and lay
people’s understanding of the mental health issue.
The way Chinese lay people construct the label, the
interpretation of cause, the way to seek help and the
attitude towards people with a mental disorder were
affected by their culture. Specifically, culture mainly
affects the beliefs about the cause of the mental
disorder and the way people try to seek help.
REFERENCES
Amanah, N., Bahari, Y., Fatmawati 2014, ‘Akulturasi
Budaya Tionghoa dengan Budaya Melayu pada
mahasiswa Pendidikan Bahasa Mandarin Fkip Untan
Pontianak’, Jurnal Pendidikan dan Pembelajaran,
vol.3, no.6, pp. 1-14.
El-Islam, F.M 2008, ‘Arab culture and mental health care,
Transcultural Psychiatry, vol.45, no.4, pp. 671-682.
Gopalkrishnan, N., & Babacan, H 2015, ‘Cultural
diversity and mental health’, Australian Psychiatry,
vol. 23, pp. 6–8.
Jacob K.S, & Patel V 2014, ‘Classification of mental
disorders: A global mental health perspective’, Lancet,
vol. 383, pp.1433-1435.
Jorm, A.F. 2000, ‘Mental health literacy: Public
knowledge and beliefs about mental disorders, British
Journal of Psychiatry, vol. 177, pp. 396-401.
Kim, K., Ryu, E., Chon M.-K., Yeun E.-J., Choi S.-Y.,
Seo J.-S. & Nam B.-W 2006, ‘Internet addiction in
Korean adolescents and its relation to depression and
suicidal ideation: A questionnaire survey’,
International Journal of Nursing Studies, vol, 43, pp.
185-192.
Kirmayer, L. J., Bhugra D., 2009. Culture and mental
illness: Social context and explanatory models. In I.
M. Salloum, J. E. Mezzich, editors. Psychiatric
diagnosis; Patterns and prospects. New York: John
Wiley & Sons.
ICOH 2019 - 1st International Conference on Health
308

Kirmayer, L. J., & Swartz, L., 2014. Culture and global
mental health. In V. Patel, H. Minas, A. Cohen, &
M. J. Prince, Global and Mental Health; Principle and
Practice. New York: Oxford University Press.
Kpanake, L 2018, ‘Cultural concepts of the person and
mental health in Africa, Transcultural Psychiatry,
vol.55, no. 2, pp. 198-218.
Kutcher, S., Wei, Y., & Coniglio, C 2016, ‘Mental health
literacy: Past, present, and future’, The Canadian
Journal of Psychiatry, vol. 61, no. 3, pp. 154-158.
Loo, P.-W. & Furnham, A 2012, ‘Public knowledge and
beliefs about depression among urban and rural
Chinese in Malaysia’, Asian Journal of Psychiatry,
vol. 5, pp. 236–245.
Novianty, A 2017, ‘Literasi kesehatan mental:
Pengetahuan dan persepsi publik mengenai gangguan
mental, Analitika, Vol. 9, no. 2, pp. 68 – 75.
Novianty, A., & Hadjam, M.N.R 2017, ‘Literasi kesehatan
mental dan sikap komunitas sebagai prediktor
pencarian pertolongan formal’, Jurnal Psikologi, vol.
44, no. 1, pp. 50-65.
Qian, J 2015, ‘Chinese Fortune Telling: A crash course in
the ancient pseudoscience of determining your future’,
Retrieved from
http://www.smartshanghai.com/articles/smsh/cheat-
sheet-chinese-fortune-telling. Rochford, T 2004,
‘Whare Tapa Wha: A Maori model of a unified theory
of health’, The Journal of Primary Prevention, vol. 25,
no.1, pp. 41-57.
Tan, M.G., 2008. Etnis Tionghoa di Indonesia: Kumpulan
tulisan, Yayasan Obor Indonesia, Jakarta.
Tseng, W.S., Lin, T.Y. & Yeh, E.K., 1995. Chinese
societies and mental health. In T. Y. Lin, W. S. Tseng
& E. K. Yeh (Eds) Chinese societies and mental
health, Oxford University Press, Hong Kong.
Wong, D.F.K., Cheng, C. W., Zhuang, X. Y., Ng, T. K.,
Pan, S.M., He, X., Poon, A 2017, ‘Comparing the
mental health literacy of Chinese people in Australia,
China, Hong Kong and Taiwan: Implications for
mental health promotion’, Psychiatry Research, vol.
256, pp. 258-266.
Yip, K.S., 2003. Traditional Chinese concepts of mental
health: The implications for multicultural professional
counseling practice. In W.O. Phoon, & I. Macindoe,
Untangling the threads: Perspectives on mental health
in Chinese communities, Transcultural Mental Health
Care, New South Wales.
Mental Health Understanding from Culture Perspective: A Study of Lay People Mental Health Literacy
309
