
Implementation of Electronic Prescription the Outpatient Services of
the X Hospital: Evaluation of Readiness Factors
Ari Nurfikri, Amalia Rachmawaty and Elsa Roselina
Hospital Administration of Vocational Administration Program Universitas Indonesia,
Kampus Baru UI Depok 1624, Indonesia
Keywords: e-Prescription, Medical Errors, Evaluation, Readiness Factors, Hospital Revenue.
Abstract: The implementation of electronic prescriptions in hospitals has been evaluated to have an impact on patient
safety and hospital income. This method of prescription had been implemented in X hospital; however, a
previous study found that the frequencies of usage were low. From March to April 2019, this mixed-method
study conducted an explanatory sequential method design in X hospital to identify the proportion of physicians
used electronic prescription and its contributing factors Quantitative data was used to design questions for an
in-depth interview with informants of X hospital. The result showed that only 23% of X hospital physicians
used electronic prescriptions, while 58,3% of them used manual prescription and some electronic
prescriptions. Physicians who did not use electronic prescriptions at all were counted to be 18,7%. Physicians
who did not use electronic prescription would have the potential to cause medical errors and reduction of
hospital revenue. It has been found that the system and supporting factors might be not adequate to follow up
on the electronic prescription despite its sufficient human resource factors and work environment.
1 INTRODUCTION
In outpatient services, one of the factors that could
potentially lead to medical errors is an error reading
prescription. Error reading on manual prescription
cannot be read, the prescription information is not
complete, the use of abbreviations that are not
standard, dose errors, mistakes rules of use, as well as
errors of dose forms (Palappallil & Pinheiro, 2018).
The use of technology in the health sector used to
reduce medical errors and improve patient safety, one
of them with electronic prescribing (Kierkegaard,
2013). With electronic prescribing may reduce errors
reading the recipe as much as seven-fold. (Klepser,
Lanham, & Cochran, 2016). The use of electronic
prescriptions in various countries has a common goal,
namely to reduce medical errors. Use of electronic
prescription in many countries have similar
objectives, namely to reduce medical errors.
However, in doing so, physicians use prescription
compliance varies. In the United States, an increase
in the use of e-prescribing from 2008 to 2014
(Klepser et al., 2016). While European countries such
as England, Sweden, Denmark, and Estonia, the case
progress increased the use of e-prescribing from year
to year (Deetjen, 2016). The increasing use of
electronic prescriptions in the United States and
Europe due to the private sector's role in investment,
and the role of government as policymaker
(Samadbeik, Ahmadi, Sadoughi, & Garavand, 2017).
Whereas the development of electronic prescribing
other countries like in India since its launch in 2014,
the response of physicians as much as 60.7% are still
using manual prescription (Palappallil & Pinheiro,
2018). In Indonesia, the implementation of electronic
prescriptions has not been widely applied in hospitals
and other healthcare facilities. This is because it is
still constrained by the number of patients so much
that it takes a long time to enter, and the inability of
hospital management gives reward and punishment to
the physician in applying electronic prescription
(Asyary, Kusnanto, & Fuad, 2013).
The successful implementation of electronic
prescribing in Europe, influenced the seven factors
that influence the factor advances in information
technology in the health system, the system design is
good, the facilities are standardized, strong
leadership, readiness digital employees and patients,
have the planning and implementation of the
appropriate (Deetjen, 2016). Due to the conditions in
Indonesia are not the same as in Europe as a whole, is
rather difficult to apply the factors that affect the
Nurfikri, A., Rachmawaty, A. and Roselina, E.
Implementation of Electronic Prescription the Outpatient Services of the X Hospital: Evaluation of Readiness Factors.
DOI: 10.5220/0009567301030107
In Proceedings of the 1st International Conference on Health (ICOH 2019), pages 103-107
ISBN: 978-989-758-454-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
103
successful implementation of electronic
prescriptions. To evaluate the readiness of the
implementation of electronic prescriptions in
Indonesia, the used approach to four factors, namely
the readiness factor of the system, human resource
readiness factors, environmental factors work
readiness, and the readiness of the supporting factors
(Pratiwi, 2013). With this approach, you can know the
achievement of each factor to evaluate.
In Europe, the adoption of electronic prescribing
is also used to increase hospital revenue. This is due
to patient adherence to physician's recommendation
to pay for healthcare in the hospital, so the hospital
will increase revenue from pharmaceutical units
(Deetjen, 2016). X hospital in Depok has a revenue
decrease in Pharmacy. This is because many
outpatient prescriptions do not take the medicine at
the pharmacy installation. The escape of these
prescriptions influenced the use of a prescription
manual. Therefore, X hospital in Depok establishes
the use of electronic prescriptions, the use of
electronic prescribing targets by 100% in outpatient
services. But in its implementation, there are still
many physicians or specialists who prescribe
manually, so that the target is not reached the use of
electronic prescribing. Impact, revenue X Hospital in
Depok has not increased according to the targets set.
The researchers wanted to evaluate the use of
electronic prescribing readiness factors in X Hospital,
seen from the factor of the system, human resource
factors, environmental work factors, and the
readiness of the supporting factors.
2 METHOD
This research is a mixed-method, with the sequential
explanatory approach. This approach uses two
phases, collecting quantitative data, analyzing the
results, and then use the results to the qualitative
research phase. Qualitative data helps strengthen and
clarify information in the initial quantitative
(Creswell, 2016). This study was conducted at X
Hospital Depok, beginning in March until April 2019.
In quantitative research, researchers will take the
proportion of data that is matched the use of
electronic prescriptions between data in the clinic
with the data in Pharmacy. Proportions obtained were
then grouped into three categories, the first category
is the use of electronic prescribing 0%, category 2
uses an electronic prescription and prescription
manual, and category 3, the use of electronic
prescribing 100%. To deepen the evaluation of the
use of electronic prescriptions, used in-depth
interviews. The subjects were medical assistants were
3 people who represent each category. Triangulation
is done by observation of electronic prescription data
in Pharmacy taken in April 2019. The results of in-
depth interviews compiled in transcripts and matrix
are grouped into the readiness factor of the system,
the human factor, the work environment factors, and
supporting factors (Pratiwi, 2013).
3 RESULT AND DISCUSSION
Hospital X in Depok, target the use of electronic
prescribing in outpatient service is 100%. In March
2019, the resulting data on the use of electronic
prescriptions as follows:
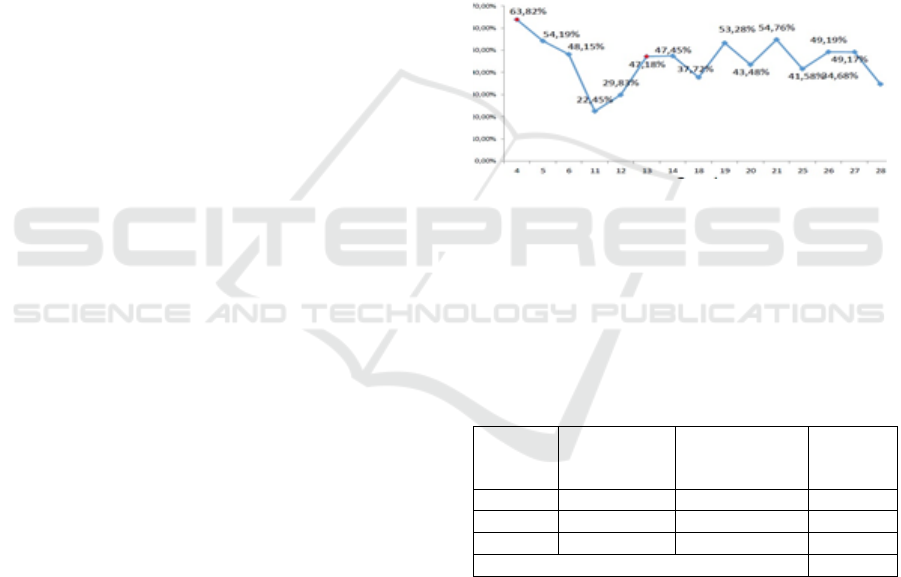
Figure 1: Percentage Use of Electronic Prescriptions
Outpatient Services Hospital X in March 2019.
From Figure 1, it appears that the use of electronic
prescribing is still below the target, the highest
percentage only 63.82%. The use of electronic
prescriptions per category can see the table below:
Table 1: Proportion of Electronic Prescription Usage Each
Category.
Category
Average
Number of
Prescriptions
Percentage of Use
Electronic
Prescriptions
Quantity
1
83,11
0%
9
2
53,76
1-99,9%
28
3
6,81
100%
11
Total
48
From table 1 above, it can be seen that the
physicians who use electronic prescribing on target
(100%), only 11 out of 48 physicians (23%), and there
are nine physicians or specialists from 48 (18.7%)
who did not use electronic prescriptions and there are
28 physicians or specialists from 48 (58.3%) still
using manual prescriptions and electronic
prescriptions. More and more prescriptions are
written, the more disobedient use of electronic
prescriptions. The fewer the number of prescriptions,
the more committed the use of electronic
ICOH 2019 - 1st International Conference on Health
104
prescriptions. To determine the outpatient service
specialists anywhere who does not use electronic
prescriptions can be seen in the following table:
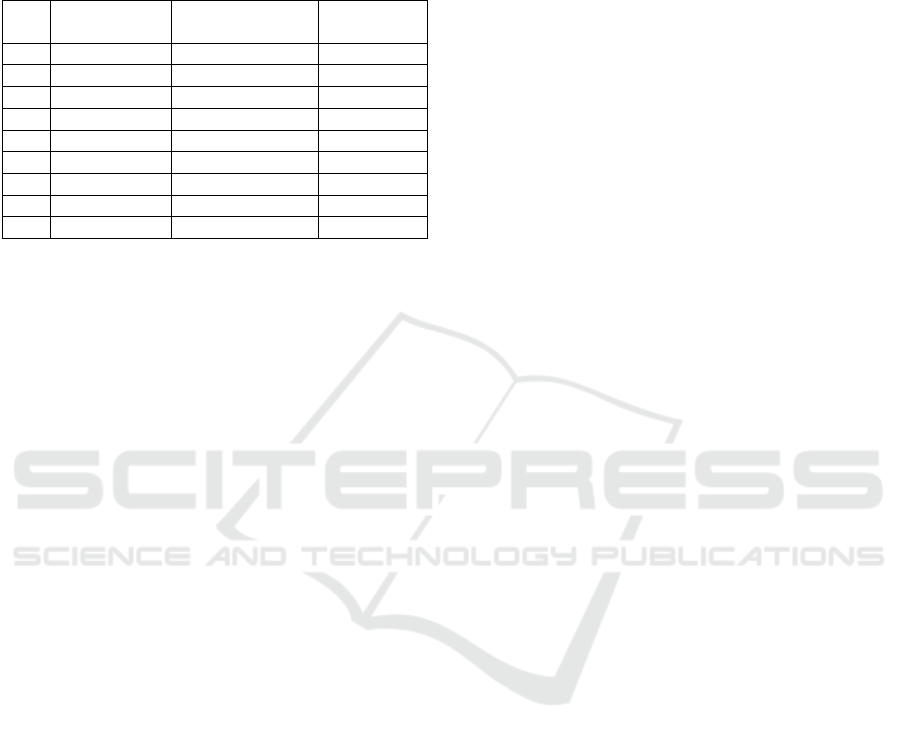
Table 2: Proportion of Use Prescription Electronics
Category 0%.
No.
Name of
Specialist
Outpatient Clinic
Total
Prescription
1
dr. F
Dermatologist
179
2
dr. Cc
Dermatologist
22
3
dr. H
Neurologist
169
4
dr. Cb
Neurologist
15
5
dr. Bt
Ortho
14
6
dr. Ag
Pulmonology
30
7
dr. D
Internist
99
8
dr. S
Internist
199
9
dr. G
Psychiatric
21
From Table 2 above, it can be seen that the majority
of specialists who do not use the electronic
prescription, the prescription number exceeds the
average number of prescriptions category 0% which is
equal to 83.11. So that the number of prescriptions,
inversely related to the use of electronic prescribing by
physicians. More and more specialist are using
prescription manually, also affect hospital revenue.
Prescriptions that go into pharmacy installation X
Hospital will be reduced because the patient does not
redeem the manual prescription medication in the
hospital. In contrast to the use of electronic
prescriptions entirely go first to the pharmacy
installation. When they see table 2 above, internists,
neurologists, and dermatologists have the highest
number of prescriptions. Drugs of the third specialists
also include classes of drugs that are expensive, to
influence the decline in X Hospital income. In Europe,
the adoption of electronic prescribing is also used to
increase hospital revenue. This is due to patient
adherence to physician's recommendation to pay for
healthcare in the hospital, so the hospital will increase
revenue from pharmaceutical units (Deetjen, 2016).
Electronic prescription comes as a solution to
reduce medication errors. However, when the use of
electronic prescribing is not applied correctly, as they
combined with a manual prescription, then it would
only cause new problems (Ghasemi et al., 2019).
Innovation in an organization including hospitals
must meet the interests of the two elements, the first
should involve top management to buy, adopt, or to
innovate. While both have to involve users of these
innovations (Faber, van Geenhuizen, & de Reuver,
2017). From Table 2 above, specialists who have
many prescriptions tend not to use electronic
prescribing. In this case, the policymakers do not
involve the user, in this case, the physicians in the
design concept of electronic prescriptions. Although
the development of electronic prescriptions tailored
to the user can encourage the physician to use and
reduce their dissatisfaction (Ghasemi et al., 2019).
To further deepen in answering the question of
how and why the use of electronic prescribing is still
low, we stepped into a stage of qualitative, in-depth
interviews with using the instrument. Evaluation of
the use of electronic prescribing is done by four
factors readiness approach (systems, human
resources, work environment, and support).
Factors readiness of the system can be seen from
the quality system. In-depth interviews show that the
electronic prescription system is still much
constrained in its use and is expected also in line with
the electronic medical record. Because if already
electronic prescriptions, but medical records are still
manual, the work is not effective. Build a system that
has a high quality is not easy, so it should continue to
do a lot of system improvements, to produce the
expected system users and outputs to be achieved as
mentioned by the informant A, B, and C below:
“…. My suggestion for electronic prescribing
more drugs to the list needs to be updated, to avoid
no-name prescription drugs want, no need to ask to
the pharmacy again …” (Informant A).
“…. If you can add features in the patient
diagnosis electronic prescription system to be more
efficient so it does not work the same twice so
consistent - the same electronics allow for quicker
….” (Informant B).
“ ….. The system needs to be improved, in order
not to die alone like an error or application …”
(Informant C).
In a major change, in this case from manual to
electronic prescribing prescription must have the
support of top management (Ghasemi et al., 2019).
With the commitment of the top management, generate
an electronic prescription system is not easily
generated error, electronic prescribing medic
integrated with electronic records and would require
substantial investment value. Integration of electronic
prescriptions with electronic prescribing, besides, to
further streamline the service time also reduces
medication errors in patients geriatric weak, and have
a history of complex diseases (Moro Agud et al., 2016).
Human resource readiness factors can be seen
from the perceived impact and adaptation of user-
friendly electronic prescriptions. The system to be
especially helpful in reducing errors in the
administration of drugs to patients. Obstacles that
happens is difficult to use electronic prescriptions if
Implementation of Electronic Prescription the Outpatient Services of the X Hospital: Evaluation of Readiness Factors
105

patients a lot because the doctor must explain the
diagnosis directly to the patient in conjunction with
the input data into the electronic prescription system.
The following statements from informants A, B, and
C on it.
…….” Help, if the patient is not crowded. If more
crowded over the manual prescription. Because
complicated, doctors diagnosing patients still
manually, keep an electronic prescription. Happens
to work twice that. So yes, all wrote the manual
prescription let me quickly…” (Informant A).
………” If longer use little help patients, if more
crowded even be inhibiting the use of electronic
prescription.” (Informant B).
……” Very helpful, to avoid incorrect attachment
of barcode or wrong in reading the recipe …”
(Informant C).
Resistance to change from the user side may
happen when they do not see the added value of such
changes, but if they voluntarily follow the changes
but no carrying capacity of hospital management,
they will combine the use of manual and electronic
prescribing (Gagnon, Nsangou, Payne-Gagnon,
Grenier, & Sicotte, 2014). Depth interviews above, it
appears that open resistance from physicians to
change from manual to electronic prescribing
prescription, but at the time many patients, they will
go back to using a manual recipe, because the medical
record still manually to avoid double work. Carrying
capacity required hospital management to
accommodate the desire of physicians in medical
records and electronic prescriptions are integrated.
Readiness factors of the work environment can be
seen when using the attitude on the implementation
of electronic prescriptions. The same problems can be
responded to differently. When there was a slight
problem with the application of electronic
prescriptions, there are re-using the recipe manually,
but there are still repeating the use of electronic
prescriptions to succeed. This can be seen in the
following informant's narrative:
……” Ever are difficult to use it, but sometimes
the data of patients seeking treatment rather not
appropriate, should that today the patient A, even the
outpatient B was yesterday already went, so we use
the manual prescription….” (Informant A).
….” In the application there is already a patient's
name, so all that remains is to prescribe the medicine.
Sometimes a prescription for one patient can be sent
twice. For example, the first prescription has been
sent, apparently, there are additional prescription
drugs. So, the recipe for additional drugs is made
again, or sometimes the recipe sent is illegible in the
pharmacy, so we make it again, maybe that's what
makes double the use of electronic prescription…”
(Informant B).
….” This is difficult to use it, but yes for any error,
so I use the recipe manually anymore …” (Informant
C).
In Kuwait, a physician as the user responds
positively, but almost half of these studies provide
input to electronic prescriptions that should have a
better function, which will make them not back to
using a manual recipe (Almutairi, Potts, & Al-Azmi,
2018). Function problems in the application of
electronic prescriptions will determine the readiness
of the working environment responds positively to the
use of electronic prescribing. In-depth interviews
mentioned above is seen in the work environment in
the X hospital has responded positively to the use of
electronic prescriptions, but with the malfunction of
the application, some specialists still use electronic
prescribing for the patient is not a lot, and re-use
prescription manuals for many patients that services
are not hampered.
Factors supporting viewable readiness of
equipment and networks. The successful use of a
system should also be supported by the network
equipment and standardized so it does not hamper the
current will be used. It is like a narrative following
informant:
“…. Ever, it is difficult for access, sometimes like
an error when you want to log into the electronic
system …” (Informant A).
“…. Sometimes a sudden want to login directly
application error ….” (Informant B).
“ ….. directly error Sometimes the time will log in
suddenly an error immediately, or the computer
suddenly restarts immediately do not know why …”
(Informant C).
In various countries have made significant efforts
to promote the use of electronic prescriptions with
several substantial investments to develop a good
system, but a little forgotten maintenance of
equipment and the network as a contributing factor
(Gagnon et al., 2014). Kuwait also noted that to
conduct electronic prescription there must be
adequate technical support for the implementation of
electronic prescribing application maintenance
(Almutairi et al., 2018). From in-depth interviews
above, it appears that the maintenance of the
equipment and network absolutely must be met for
the smooth use of electronic prescribing in hospitals
X. routine and unscheduled maintenance of the
ICOH 2019 - 1st International Conference on Health
106

equipment and the network, the user can reduce
electronic prescriptions complain of hard login or
sign in to the app.
4 CONCLUSIONS
The use of electronic prescriptions in X Hospital
Depok does not comply with the specified target
(100%). 23% use of the electronic prescription as a
whole is still far from the target set. While the use of
the still use of electronic prescriptions and
prescriptions manual amounted to 58.3%, and that
does not use at all prescription electronics by 18.7%.
Specialists who do not use electronic prescriptions,
potentially cause medical errors and reduce hospital
income. It has been found that the system and
supporting factors might be not adequate to follow up
on the electronic prescription despite its sufficient
human resource factors and work environment.
ACKNOWLEDGMENTS
We thank those who have helped, so the
implementation of this research.
REFERENCES
Almutairi, B. A., Potts, H. W. W., & Al-Azmi, S. F. (2018).
Physicians' perceptions of electronic prescribing with
electronic medical records in Kuwaiti primary healthcare
centers. Sultan Qaboos University Medical Journal.
https://doi.org/10.18295/squmj.2018.18.04.008
Asyary, A., Kusnanto, H., & Fuad, A. (2013). Sistem
Peresapan Elektronik pada Keselamatan Pengobatan
Pasien. Kesmas: National Public Health Journal.
https://doi.org/10.21109/kesmas.v8i3.355
Creswell J, 2016, Research Design, Qualitative,
Quantitative, and Mixed Methode Approaches, Fourth
Edition (Fawaid, A & Pancasari R, penerjemah),
Pustaka Pelajar, Yogyakarta (Buku asli diterbitkan
2014).
Deetjen, U. (2016). European E-Prescriptions: Benefits and
Success Factors. Cyber Studies Programme.
Faber, S., van Geenhuizen, M., & de Reuver, M. (2017).
eHealth adoption factors in medical hospitals: A focus
on the Netherlands. International Journal of Medical
Informatics. https://doi.org/10.1016/j.ijmedinf.2017.
01.009
Gagnon, M. P., Nsangou, É. R., Payne-Gagnon, J., Grenier,
S., & Sicotte, C. (2014). Barriers and facilitators to
implementing electronic prescription: A systematic
review of user groups’ perceptions. Journal of the
American Medical Informatics Association.
https://doi.org/10.1136/amiajnl-2013-002203
Ghasemi, S. H., Etminani, K., Dehghan, H., Eslami, S.,
Hasibian, M. R., Vakili Arki, H., … Namayandeh, S.
M. (2019). Design and evaluation of a smart medication
recommendation system for the electronic prescription.
Studies in Health Technology and Informatics.
https://doi.org/10.3233/978-1-61499-971-3-128
Kierkegaard, P. (2013). E-Prescription across Europe.
Health and Technology. https://doi.org/10.1007/
s12553-012-0037-0
Klepser, D., Lanham, A., & Cochran, G. (2016). Electronic
prescriptions: opportunities and challenges for the
patient and pharmacist. Advanced Health Care
Technologies. https://doi.org/10.2147/ahct.s64477
Moro Agud, M., Menéndez Colino, R., Mauleón Ladrero,
M. del C., Ruano Encinar, M., Díez Sebastián, J.,
Villamañán Bueno, E., … González Montalvo, J. I.
(2016). Analysis of electronic medication
reconciliation and information at discharge programme
for frail elderly patients. International Journal of
Clinical Pharmacy. https://doi.org/10.1007/s11096-
016-0331-4
Palappallil, D. S., & Pinheiro, C. (2018). Perceptions of
prescribers towards electronic prescription: A pre-
implementation evaluation. Journal of Young
Pharmacists. https://doi.org/10.5530/jyp.2018.10.69
Pratiwi, P. M. D. 2013. "Analisa Kesiapan Pelayanan
Farmasi Rawat jalan Dalam Penerapan Sistem E-Resep
di Rumah Sakit Karya Bakti Tahun 2013 Thesis
Universitas Indonesia.
Samadbeik, M., Ahmadi, M., Sadoughi, F., & Garavand, A.
(2017). A comparative review of electronic prescription
systems: Lessons learned from developed countries.
Journal of Research in Pharmacy Practice.
https://doi.org/10.4103/2279-042x.200993
Implementation of Electronic Prescription the Outpatient Services of the X Hospital: Evaluation of Readiness Factors
107
