
Effectiveness of the Role of the Family-based as Observer Direct
Treatment for Tuberculosis Transmission Control
Bahtera B. D. Purba, Anggi Pramono Siregar, Bunga Rimta Barus, Cristica I. Surbakti
Faculty of Public Health and Faculty of Pharmacy, Institut Kesehatan DELI HUSAD
[Bahterabd, bungarimtabarus, christica, anggipramono95]@delihusada.ac.id
Keywords: Compliance with Medication, Tuberculosis, family-based DTO (Direct Treatment Observers), Health
Officers-based DTO (Direct Treatment Observers)
Abstract: In Tapanuli Tengah, Indonesia, 2142 positive TB cases were found. At 2886 cases of TB, 2384 cases
(82.6%) of new cases were found and 502 cases (17.4%) of cases of MDR (Multiple Drug Resistance) were
found. This study aims to examine the effectiveness of the family-based-based DTO (Direct Treatment
Observers) intervention’s model for drug adherence in TB patients. Participants in this study consisted of 92
families as direct treatment observers who were determined using a non random consecutive sampling
method. Data analysis was performed with one-way ANOVA at the level of significant α = 0.05. The results
of the analysis showed that there were differences in the effectiveness of the family-based-based DTO
(Direct Treatment Observers) and Health Officers-based DTO (Direct Treatment Observers) with a score of
3.5 (p = 0.001), the effectiveness of the environmental control of the family-based-based DTO (Direct
Treatment Observers) and the Health Officers-based DTO (Direct Treatment Observers) with score 7.5 (p
= 0.001), effectiveness of the family-based-based DTO (Direct Treatment Observers) droplet control with
the Health Officers-based DTO (Direct Treatment Observers) with a score of 3.8 (p = 0.001). It is
recommended that the Dinas Kesehatan Tapanuli Tengah to make training for families and health workers
as observer for taking medicine in the DOTS program.
1 INTRODUCTION
In Tapanuli Tengah, Indonesia at 2018 found 2384
new cases of TB (Purba, 2018). It is estimated that
the number of all new and old cases is 2,886 with
MDR (Multiple Drug Resistance) cases reaching
502 cases (Sis, 2017). The high MDR TB cases
show that the duration of TB treatment is increasing
with an average of 2 years (Daptes Tapteng, Dinkes,
2017). In Puskesmas Gonting Mahe, Tapanuli
Tengah, in the period of January-December 2018,
there were 142 positive cases of TB. At 142 TB
cases, 89 cases (62.6%) were new cases and 53 cases
(37.4%) were MDR-TB. From the records of TB
case at Puskesmas Gonting Mahe, it was found that
the success rate of TB increased from 2015 to 2018,
respectively from 76.4%, 78.8%, 83.7% and 89.6%
with an average increase of 4.4 % per year (Dinas
Kesehatan Sumatera Utara, 2018).
Tuberculosis is a disease caused by
micobacterium tuberculosis which can be
transmitted by removing nucleus droplets into the air
through coughing and sneezing (Mathema, 2017).
TB transmission can be controlled through
medication, environmental control, and control of
droplet nuclei (CDC, 2019).
TB transmission is caused by the low control of
the treatment of active TB cases, environmental
control, and controlling the behavior of removing
phlegm and sputum (droplet nuclei) by sufferers
(CDC, 2019; Mathema, 2017). Compliance with
medication, environmental control, and control of
droplet nuclei or called compliance with taking
medication can be defined as the level of obedience
of patients carrying out all instructions given in
treatment, provision of a sanitary environment, and
the behavior of closing the mouth when coughing
and sneezing and expelling sputum in a closed
container ( Mathema, 2017).
Controlling transmission requires special
attention from patients and family-based members.
Liang in her research found that family-based-based
DTO (Direct Treatment Observers) was more
effective than other DTO in taking medication
compliance (Liang, 2018). WHO stresses the
important role of DTOs in the DOTS (Directly
20
Purba, B., Siregar, A., Barus, B. and Surbakti, C.
Effectiveness of the Role of the Family-based as Observer Direct Treatment for Tuberculosis Transmission Control.
DOI: 10.5220/0009461800200027
In Proceedings of the International Conference on Health Informatics and Medical Application Technology (ICHIMAT 2019), pages 20-27
ISBN: 978-989-758-460-2
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
Observed Treatment Short Course) program to
achieve zero TB in 2030 (WHO, 2017). The role of
DTO in handling TB cases becomes very important
due to the physical, economic, psychological, and
social DTO and TB patient's inability to face a long
treatment process (Sis, 2017). According to Martin
motivation is an important element for DTO in
carrying out their work (Martin, 2016). According to
Teroi Protection Motivation states that patient
compliance in consuming drugs is influenced by the
motivation of patients and their families. Pulmonary
TB treatment requires a long period of time between
6-9 months. This makes the patient has less
motivation or desire because they often experience
despair and risk not being compliant in taking
medication. To ensure regularity, the desire to take
medication requires a motivation both internal and
external and DTO has a role in supervising patients
every time they take medicine. Research conducted
by Prasetya and Nadin found a strong relationship
between family-based motivation and medication
adherence (Prasetya, 2017; Ratnaningsih, 2016).
Martin found the effect of age, sex, marital status,
and socioeconomic on patient compliance (Nawell,
2016). The CDC found a strong relationship
between patient noncompliance and low TB
knowledge and high TB transmission (WHO, 2016).
The handling of TB cases in Puskesmas is carried
out based on the DOTS strategy. The DOTS
program that is run at the Puskesmas is one of the
TB treatment control programs with the aim of
thoroughly treating TB patients (success rate 100%)
(WHO, 2017). Based on this the effectiveness of the
family-based-based DTO in treatment control, the
environment, and nuclear droplets needs to be
investigated.
2 METHOD
This research uses rexplanatory method with cross
sectional approach. Effectiveness of treatment
control, environment, and droplet nuclei of family-
based-based DTO with health officers-based
determined by the value of product moment (r)
correlations. This research was carried out at
Puskesmas Gonting Mahe Sorkam, Tapanuli Tengah
in 2019 with a period of 6 months from January-
June 2019.
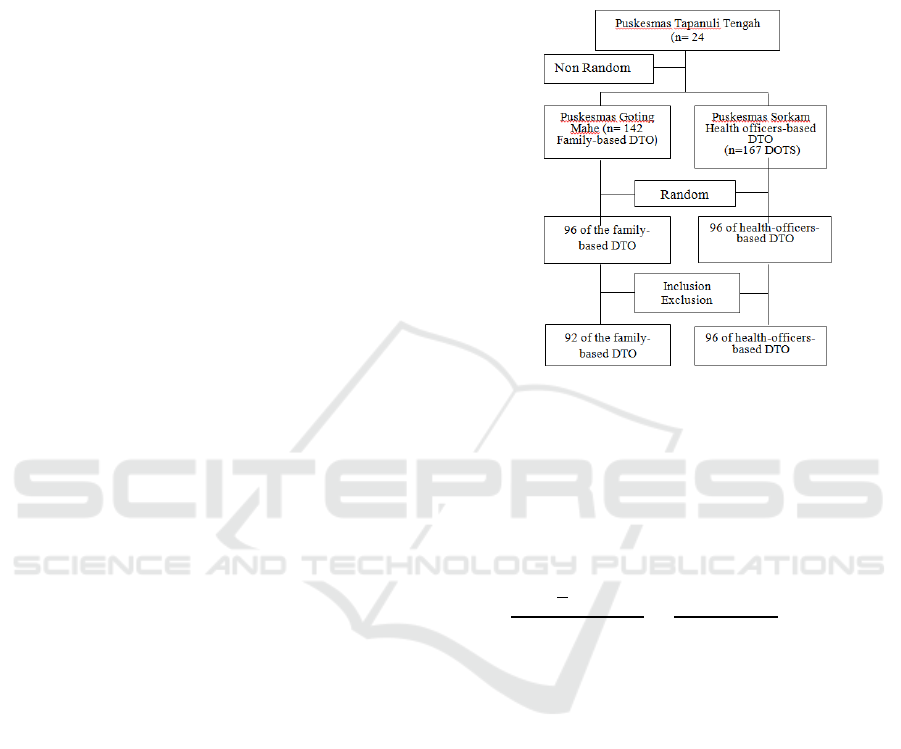
Participants in this study were 92 DTO families
of tuberculosis patients who were undergoing DOTS
treatment program in Puskesmas Gonting Mahet
2019. The comparison group consisted of 96 DTO
health workers from Puskesmas Sorkam with almost
the same characteristics as puskesmas Mahe gonting.
Family-based-based DTO inclusion criteria: aged
15-60 years, core family-based members of TB
patients, have a health BPJS payment system and
exclusion criteria: HIV / AIDS TB patients, diabetes
mellitus TB, unable to, and refuse to participate.
Figure1: DTO participant listing.
The sample size was determined based on a
minimum sampling formula from Lameshow with a
probability value of the occurrence of tuberculosis
unknown (p = 0.5). Based on the value of p = 0.5
The number of samples in this study was determined
based on the following formula:
Source: Senedecor GW, Cochran WG (1997);
Lameshow (1997)
This formula provides an illustration of n is the
number of samples needed, Z1-α / 2 is the value of Z
in the degree of significance (95% = 1.96), p is the
proportion of a particular case to the population (p =
0.5) and d is the degree deviations from the desired
population: 10% (0.10).
The research instrument used the Self
Dertermination Questionnaire (SDT) from Deci and
Ryan with dimensions of competence, autonomy,
and relations. The questionnaire used first tested the
validity (corrected item total correlation) CITC> 0.5
and Cronbach's Alpha reliability> 0.6. Data analysis
was performed by one way ANOVA statistical test
at the significance level α = 0.05.
Effectiveness of the Role of the Family-based as Observer Direct Treatment for Tuberculosis Transmission Control
21

3 RESULTS
The characteristics of the family-based-based DTO
and health officers-based DTO are important
elements in this study. This is because in addition to
internal factors, individual motivation is also
inseparable from the characteristics and other
external factors of the individual concerned. The
characteristics of DTO in this study are focused on
people, education, relationships with TB patients,
treatment control, environmental control, and droplet
nuclei control.
The mean age of family-based-based DTOs in
this study was lower (38.9 ± 9.7 years) compared to
health officers-based DTO (39.4 ± 10.4) years.
School years of family-based DTO were also found
to be lower (7.2 ± 4.3) years compared to health
officers-based DTO (14.5 ± 2.3) years. The control
of family-based DTO treatment was higher (13.1 ±
1.5) compared to health officers-based DTO (9.6 ±
2.0), environmental control of family-based DTO
was higher (14.7 ± 2.1) compared to DTO health
officers-based (7.2 ± 2.2), and control droplet nuclei
were higher in family-based DTO (12.1 ± 2.2)
compared to health workers DTO (8.3 ± 2.5).
Family-based DTO motivation was also higher
found in family-based DTO (85.1 ± 10.0) compared
to the motivation of health officers-based DTO (78.5
± 5.0).
Table 1: DTO characteristics in puskesmas goting mahe
in 2019.
Characteristic
s
Family-based
DTO (n=92)
Health workers
DTO (n=96)
Mean
SD
Mean
SD
Age
38.9
9.7
39.4
10.4
School year
7.2
4.3
14.5
2.3
Kontrol
Pengobatan
13.1
1.5
9.6
2.0
Kontrol
Lingkungan
14.7
2.1
7.2
2.2
Kontrol
Droplet
Nuclei
12.1
2.2
8.3
2.5
Motivasi
85.1
10.0
78.5
5.0
DTO: Direct Treatment Observers; n: Number of
Samples; SD :Standard Deviation
Differences in the motivation of treatment
control, environmental and family-based DTO
nucleus droplets and health officers-basedDTOs
with the one way ANOVA test also showed
significant differences.
From the table above it can be seen that there
are differences in the control of family-based DTO
treatment with health officers-based DTO (p =
0.001; p <0.05). In the case of environmental control
also found a significant difference in the DTO of the
family-based and the DTO of the health officers-
based (p = 0.001; p <0.05). In the control category
droplet nuclei also found significant differences in
DTO of family-based with health officers-based
DTO (p = 0.001; p <0.05). Likewise, the motivation
of the family-based DTO was found to be different
from the of the health officers-based DTO (p = 0.03;
p <0.05).
Table 2: Differences in the Effectiveness of Family-Based
DTO and Health Officers-Based DTO.
Categor
y
Family-
based
DTO
(n=92)
Health
officers-
based
DTO
(n=96)
Differ
ence
p
Treatme
nt
13.1±1.5
9.6±2.0
3.5
0.001
Environ
ment
14.7±2.1
7.2±2.2
7.5
0.001
Droplet
nuclei
12.1±2.2
8.3±2.5
3.8
0.001
Motivati
on
85.1±10
78.5±5.0
6.6
0.03
p = Probability of significance at α = 0.05
4 DISCUSSION
From the results of statistical analysis found a
significant difference in the motivation of family-
based DTO and health officers-based DTO
motivation’s to control the tuberculosis transmission
in the work area of Gonting Mahe,, Tapanuli
Tengah. Transmission control compared with DTO
motivation of health officers-based.
The results of this study are consistent with a
variety of previous research. Liang in his study
found family-based DTO was more effective than
other DTOs in controlling tuberculosis treatment
(Liang, 2018). WHO emphasizes the important role
of DTOs in the DOTS program to achieve zero TB
by 2030 (WHO, 2016; WHO, 2017). The role of
DTO in handling TB cases is very important due to
the physical, economic, psychological, and social
disability of DTOs and TB patients in dealing with a
long treatment process (Sis, 2017; Cameron, 2018).
WHO’s DOTS strategy has helped improve
outcomes in TB in many ways: new resources have
been channelled towards TB control programmes,
drug supplies and information systems have been
ICHIMAT 2019 - International Conference on Health Informatics and Medical Application Technology
22

strengthened and targets have been set. The strategy
has helped ensure that national governments take
notice of TB control efforts in their countries and
also that advances have been made in the coverage
and quality of TB control globally. WHO has
refined the global programme in the Stop TB
Strategy.1 To ensure that patients benefit from these
efforts, it is clear that good health services are
necessary but not sufficient. Patients still need to
choose to take the drugs (Purba, 2018).
Many studies centred on the influence of
patients' understanding of treatment, including its
duration and the consequences of defaulting, on
adherence to treatment. The long treatment period
was poorly understood by patients and adherence
appeared to be facilitated where patients understood
the importance of completing treatment. One study
on adherence to prophylaxis reported that
nonadherent patients had little information on TB as
a disease, but were very aware of the potential
adverse effects caused by treatment (Mathema,
2017).
Patients beliefs about the efficacy of treatment,
both positive and negative, may impact on
adherence. Patients may question the efficacy of the
pills or think that only injections are medicine, or
even question the validity of diagnostic tests that are
not considered sophisticated enough for such a
dangerous disease. Belief in treatment efficacy
appeared to be related to patient confidence in the
medical system; in some cases community-based
treatment programmes increased confidence among
community members that TB could be cured.
Another study noted that patients preferred to
consult traditional healers (Purba, 2018).
People occupying this polarity believe that
poor adherence is a problem for the public health
system caused by recalcitrant patients; these patients
don’t know, don’t care and don’t understand why
they need to complete the full course of treatment.
The natural response to this set of beliefs is to devise
a menu of policies to educate, to motivate, to watch
and to punish patients if they do not do as instructed
(Purba, 2019).
At the other extreme, policy-makers and
providers consider it their job to deliver an
intervention that is generally highly effective against
a life-threatening and debilitating disease. For this
approach to succeed, health-care practitioners must
work within an effective health system that delivers
care appropriate to people’s needs. If a large
proportion of people do not complete treatment, then
it is the health-care system that has failed, by not
delivering what it is supposed to. This viewpoint
emphasises that a health-care system should operate
in a way that is appropriate to people’s needs, rather
than emphasising the development of means for
providers to control patients’ behavior (Purba,
2018).
Fear and denial of diagnosis were common
themes across the included studies. Some patients
had difficulty accepting their diagnosis, often
wanting to hide their disease. In other studies,
patients' desire to be cured was cited as a motivator
for adherence in people presenting with TB
symptoms, and patients' fear of the negative
consequences of irregular treatment was associated
with treatment adherence. Patients could be
nonadherent if they were taking other western or
traditional medicines and perceived there to be
negative consequences if these were taken
concurrently with TB medication. Two studies
mentioned a relationship between pregnancy and
nonadherence, one of which noted that female
patients believed that pregnancy would increase
intolerance to drugs and make TB drugs ineffective
(Mathema, 2017).
The difference in motivation between the
family-based PMO and the health officers-based
PMO is because the family PMO in the work area of
the Puskesmas Goting Mahe Community is a close
family member who has emotional connections with
tuberculosis patients. In this context, the family-
based PMO can be the TB patient's wife, parents,
and siblings or sister of the patient. In controlling the
treatment of TB patients, the family has a dual role
as the observers of taking the medicine and also as a
close family member of the patient (Cameron,
2018).
The difference in motivation effectiveness of
family-based DTOs compared to health officers-
based DTOs is due to cultural factors. In the work
area of Puskesmas Gonting Mahe Community, all
tuberculosis patients come from the Batak tribe.
Batak tribes have been known to have a very strong
kinship relationship in the family-based. The nature
of helping in the family-based, especially in difficult
situations, is one of the characteristics of the Batak
people.
During the research process it was also found
that family-based members in the Batak tribe such as
tulang, namboru, bapa tua, brothers often gave
assistance to the family-based DTO. This assistance
can be in the form of transportation assistance to
take medicine to the Puskesmas and help with
money to buy milk and nutritious food (Samuel,
Effectiveness of the Role of the Family-based as Observer Direct Treatment for Tuberculosis Transmission Control
23

2016). In certain custom events DTO families also
often get motivation from other relatives to be able
to deal with tuberculosis problems that are faced by
family-based members.
Likewise, TB patients often get certain advice
from relatives in certain traditional events. These
advice can certainly be a motivation for DTO
families and TB patients to be more confident and
motivated to improve medication adherence
behavior. According to protection motivation theory
, if the family-based DTO is motivated to treat and
supervise TB patients taking medication and TB
patients also feel motivated to take medication
regularly then this motivation will manifest into
controlled actions (Sirur, 2016).
From observations made during the research
process in the work area of Gonting Mahe Health
Center, North Tapanuli Regency, that family
members such as bones, namboru, elderly fathers,
brothers often provide assistance to DTO families,
for example in taking drugs to the puskesmas
delivered by relatives who have vehicles. Financial
assistance is also often given to buy milk and
nutritious food in tuberculosis patients. In certain
custom events DTO families also often get
motivation from other relatives to be able to deal
with tuberculosis problems being faced by family
DTO family members. Likewise, TB patients often
get certain advice from relatives in certain traditional
events. These advice can certainly be a motivation
for family DTOs and TB patients to be more
confident and motivated to improve their
compliance with medication. According to the
protection motivation theory, if the family DTO is
motivated to treat and supervise TB patients taking
medication and TB patients also feel motivated to
take medication regularly then this motivation will
manifest in controlled actions.
Family DTO has a dual role in controlling
tuberculosis treatment which is different from other
DTOs which only have a single role. The role of the
family DTO is to carry out the supervision process
in accordance with instructions given by health
workers and care for tuberculosis patients. Caring
for patients who are family members themselves is
also a moral responsibility held by the family DTO.
And in the tradition of the Batak tribe, it is the
responsibility to treat patients until they recover
despite spending their possessions in the process of
treatment (Purba, 2018).
The emotional, psychological, values, and
cultural relationships that are adopted are
distinguishing factors that influence the motivation
of the family DTO with the motivation of the DTO
health workers, DTO teachers, and DTO community
leaders in the work area of Sorkam, Central Tapanuli
Regency. Motivation is the driving force of an
individual to act on something both influenced by
intrinsic factors and extrinsic factors. The emotional,
psychological, values and cultural relationships are
elements of a relationship based on the formation of
motivation in accordance with the opinion of Deci
and Ryan (2012) in the theory of self-determination.
If these intrinsic elements are still maintained and
developed, and training in family PMOs is
consistently carried out, then control of tuberculosis
treatment can be effectively carried out. This is also
consistent with Deci and Ryan's theory which states
that high motivation in individuals to take an action
if the individual is given the right relationship,
freedom, and competence to do the action (Purba,
2019).
Family-based DTO has a dual role in
controlling tuberculosis transmission which is
different from health officers-based DTO who only
have a single role. The role of the family-based DTO
is to carry out the supervision process in accordance
with instructions given by health workers and care
for tuberculosis patients. Caring for patients who are
family-based members themselves is also a moral
responsibility held by the family-based DTO. In the
tradition of the Batak tribe, it is the responsibility to
treat patients until they recover despite spending
their possessions in the process of treatment.
The emotional, psychological, values, and
cultural relationships that are adopted are
distinguishing factors that affect the motivation of a
family-based DTO with the motivation of a health
officers-based DTO. Motivation is the driving force
of an individual to act on something both influenced
by intrinsic factors and extrinsic factors.
Emotional, psychological, value and cultural
relationships are elements of relationships based on
the formation of motivation in accordance with the
opinions of Deci and Ryan (2012) in the theory of
self-determination (Maclean, 2016; Martin 2016,
Sis, 2017). If these intrinsic elements are still
maintained and developed, as well as training on
DTO families consistently carried out so controlling
tuberculosis transmission can be effectively carried
out (maclean, 2016). This is also consistent with
Deci and Ryan's theory which states that high
motivation in individuals to take action if individuals
These relations are given the right, the freedom, and
the competence to carry out these actions (Mathema,
2017).
Health Officers are the first and foremost
jargon in overcoming all health problems faced by
ICHIMAT 2019 - International Conference on Health Informatics and Medical Application Technology
24

each individual, group, and community. From the
results of the analysis in this study found a
significant difference in the control of family-based
DTO treatment with health officers-based DTO.
This means that family-based DTO in controlling
tuberculosis transmission have more effective
motivation than health officers-based DTO (Martin,
2016; Mathema, 2017).
The difference in motivation of family-based
DTO and health officers-based DTO in the work
area of Puskesmas Gonting Mahe Community,
Tapanuli Tengah is due to the perception of the local
community on health officers. At first the DTO
established by the DOTS program in the supervision
of eating medicine was a health officers. As time
goes by, Health officers-based DTO cannot serve all
TB patients in one work area, so DTO can be
recruited from teachers, family-based members and
community leaders who are first given training. In
carrying out their duties the DTO is given an
honorarium in accordance with the work stipulated
in the DOTS program (WHO, 2016; WHO, 2017).
The results of the analysis in this study indicate
that there are differences in the effectiveness of
environmental control and nucleus droplets of
families-based DTO with health-officers based DTO
in tuberculosis transmission control. This result of
this study are consistent with previous studies which
also found that there are differences in
environmental control and control of nuclei droplets
of family-based DTO with health officers-based
DTO in tuberculosis transmission control (Prasetya,
2017; Sis, 2017).
Health literacy has become very important in
improving the control of treatment of TB patients,
especially in rural areas where access to information
is still very low. Increased individual health literacy
will depend on individual interests, intentions,
interests, and beliefs (Martin, 2015). This lack of
interest, intention, and belief makes PMO teachers
and PMO community leaders not as motivated as
effectively as the motivations of family PMOs and
health workers (Purba, 2019).
The results of the analysis in this study indicate
that there is no difference in the motivation of PMO
teachers and PMO community figures for
tuberculosis treatment control. This shows that the
placement of PMO teachers and PMO community
leaders are not effective in controlling the treatment
of tuberculosis patients. The results of this study are
consistent with previous research which also found
that there was no difference in the influence of PMO
teachers and PMO community leaders on
tuberculosis treatment control (Prasetya, 2009; Sis,
2004).
PMO teachers and PMO community leaders
are two types of PMO that are not related to familial
relations with tuberculosis patients. The PMO was
initially appointed by local health workers to replace
the PMO of health workers in places where health
workers are very poor especially in rural areas. The
teacher's PMO and community leaders' PMO in
carrying out their duties are only based on the
incentives received, but emotionally very different
from the family's PMO.
PMO teachers and PMO health workers also do
not have special expertise in the field of health
despite receiving certain training. Community
perceptions of teachers and community leaders will
be very different from perceptions of health workers.
Observations during this research process showed
that TB patients felt that PMO teachers and PMO
community leaders did not work effectively and
were also unable to answer TB patients' questions
completely.
5 CONCLUSION
Motivation of family-based DTO was 6.6 score,
control treatment was 3.5 score, environmental
control was 7.5 score and control of nucleus droplet
was 3.8 score compared to health officers-based
DTO in controlling tuberculosis transmission.
Family-based DTO has motivation, treatment
control, environmental control, and droplet nuclei
control which is more effective on controlling
tuberculosis transmission compared to health
officers-based DTO.
6 SUGGESTION
It is recommended to the Dinas Kesehatan Tapanuli
Tengah to develop TB control programs through
family-based-wide DTO until tuberculosis
transmission can be effectively controlled.
ACKNOWLEDMENT
This research was supported by Institut Kesehatan
Delihusada Delitua, Institut Kesehatan Medistra
Lubuk Pakam, Sembiring Hospitel Foundation, and
Grand Med Hospital Foundation, Indonesia.
Effectiveness of the Role of the Family-based as Observer Direct Treatment for Tuberculosis Transmission Control
25

REFERENCES
Cameron, J.; Pierce,W. D. 2018. Reinforcement, Reward,
and Intrinsic Motivation: A Meta-Analysis, Review of
Educational Research
CDC, 2017; Managing Tuberculosis Patients and
Improving Adherence. U.S. DEPARTMENT OF
HEALTH AND HUMAN SERVICES ,Centers for
Disease Control and Prevention, National Center for
HIV/AIDS, Viral Hepatitis, STD, and TB Prevention,
Division of Tuberculosis Elimination, Atlanta,
Georgia
CDC, 2019.Patient Adherence To Tuberculosis Treatment;
U.S. Department Of Health And Human
ServicesPublic Health Service, Atlanta, Georgia
Cut, Z. 2008; Pengembangan Motivasi Individu dalam
Dunia Kerja, Rineka Cipta. Jakarta
Dave PV, Shah AN,Nimavat PB, Modi BB,Pujara KR,
Patel P, at al,. Direct Observation of Treatment
Provided by a Family-based Memberas Compared to
Non Family-based Member among Children with New
Tuberculosis:A Pragmatic,Non-Inferiority, Cluster-
Randomized Trialin Gujarat, India. PLOS 2016;
11:e0148488
Haas JD, Booysen V, Kaseke L, 2018;Tuberculosis
infection prevention and control. Battercare.
Kementerian Kesehatan Republik Indonesia, 2016.Jakarta
Pengendalian Penyakit dan Penyehatan Lingkungan.
Pedoman Nasional Penanggulangan Tuberculosis
Kumar V, Abbas, A.K., Fausto N, Mitchell RN
(2017). Robbins basic pathology . Saunders Elsevier.
page. 516–522.
Lemos, A,. Matos, E,.2016; Multidrug-Resistant
Tuberculosis. Brazilian Journal Infectious Diseases.
Liang L, Gao L, Hao Y, Liu C, 2018; Factors Contributing
to the High Prevalence of Multidrug-Resistant
Tuberculosis: A Study from China. PUB MED
Maclean, RT, 2016. Tutor-PHC Research Trainees;
Conceptualizing Primary Health Care University of
British Columbia, Vancouver, BC.
Martin, L,. Williams, S,. Haskard, K,. DiMatteo, R,. 2016;
The Challenge of Patient Adherence, Department of
Psychology, La Sierra University, CA, USA;
2Department of Psychology, University of California,
Riverside, CA, USA.
Mathema B,Jason R. Andrews, Cohen T, Martien
W. Borgdorff, at al. Drivers of Tuberculosis
Transmission. The Journal of Infectious Diseases
2017; 216: 644–53
Mathema, B,. Andrew, JR,. Cohen, T,. Brogdorff, MW,.
Behr, M,. Glynn, JR,. At al. Drivers of Tuberculosis
Transmission. The Journal of Infectious Diseases.
2017; 2016: 5644-53
Mitchell, T. R. 2017. Research in Organizational
Behavior. Greenwich, CT: JAI Press
Newell, JN,. Baral, SC,. Pande, SB,. Bam, DS,. Malla,
PL,. Family-based-member DOTS and community
DOTS for tuberculosis control. Proquest. 2016; 367:
903
Newell, JN,. Baral, SC,. Pande, SB,. Bam, DS,. Malla,
PL,. Family-based-member DOTS and community
DOTS for tuberculosis control. Proquest. 2006; 367:
903
Nissa MK, 2018; Kenapa Penderita TBC Harus Punya
Pengawas Minum Obat (DTO), Halo Sehat Tim.
Pagaoa, MA,. Royce, RA,. Cheng, MP,. Golup, JE,.
Davidow, AL,. Moyerman, YH,. at al. Risk factors for
transmission of tuberculosis among United States-born
African Americans and Whites. PMC. 2017: 19: 1485-
1492
Pasipondya, JG; Gumbo T (2018). A Meta analysis of
self administrative Directly Observed Therapy
affect.. Clin Infect Dis. PMC 3669525. PMID
23487389.
Prasetya J, 2017. Hubungan Motivasi Pasien TB Paru
dengan Kepatuhan Dalam Mengikuti Program
Pengobatan Sistem DOTS di Wilayah Puskesmas
Genuk Semarang, Jurnalvisikes. Volume 8 no 1,
halaman 46-53.
Purba BD, 2018; Pengaruh determinan sistem informasi
terhadap kualitas data dots program di puskesmas
kabupaten deli serdang. Researcgate,
https://www.researchgate.net/publication/331198113_
pengaruh_determinan_sistem_informasi_terhadap_kua
litas_data_dots_program_di_puskesmas_kabupaten_d
eli_serdang
Purba BD, 2019; pengaruh sosiaodemografi dan budaya
terhadap pencarian pengobatan pasien tuberculosis,
Researchgate,
https://www.researchgate.net/publication/334989132_
pengaruh_sosiaodemografi_dan_budaya_terhadap_pen
carian_pengobatan_pasien_tuberculosis
Ratnaningsih, T. Ati, ASN, 2016; Hubungan Motivasi Ibu
Dengan Kunjungan Posyandu Balita di Posyandu
Dusun Kumitir Kecamatan Jatirejo Kabupaten
Mojokerto, Jurnal penelitian kesehatan
Robbins, Stephen P.; Judge, Timothy A. 2018. Perilaku
Organisasi Buku 1, Jakarta: Salemba Empat
Salla G, Roggi, A,. Matteelli A,. 2016; Tuberculosis:
Epidemiology and Control. PMCID
Samuel, B,. Volkmann, T,. Cornelius, S,. Mukhopadhay,
S,.2016; Relationship between Nutritional Support and
Tuberculosis Treatment Outcomes in West Bengal,
India. HHS Public Access
Sirur, R, Richardson, J,. Wishart, L,. Hanna, S, 2016; The
Role of Theory in Increasing Adherence to Prescribed
Practice. Proquest
Sis, YH,. Jannati, A,. Jafarabadi, MA,. Kalan, ME,.
Taheri, A,. Koosha, A,.The Effectiveness of Family-
based-Based DOTS versus ProfessionalFamily-based
Mix DOTS in Treating Smears Positive
Tuberculosis.Health Promotion Perspectives. 2017; 4:
98-106
Sis, YH,. Jannati, A,. Jafarabadi, MA,. Kalan, ME,.
Taheri, A,. Koosha, A,. The Effectiveness of Family-
based-Based DOTS versus ProfessionalFamily-based
Mix DOTS in Treating Smears Positive Tuberculosis.
Health Promotion Perspectives. 2004; 4: 98-106
ICHIMAT 2019 - International Conference on Health Informatics and Medical Application Technology
26

Sreeramareddy,. Candrashekhar, T,. Harsha, KHN,.
Arokiasamy, JT,. Prevalence of self-reported
tuberculosis, knowledge about tuberculosis
transmission and its determinants among adults in
India: results from a nation-wide cross-sectional
household survey. BMC Infection Diseases. 2013; 10:
1186.
TB Indonesia, 2018; Epidemiology TB di Indonesia..
Volmink, J; Garner P (2018). Directly Observed Therapy
for Treating Tuberculosis. Cochrane Database of
Systematic Reviews: PMC 4460720. PMID.
Walley, JD,. Jhon, D,. Khan, MA,. Newell, JN,. Khan,
MH,. Effectiveness of the direct observation
component of DOTS. Proquest. 2001; 357: 664
WHO, 2016; Building on and enhancing DOTS to meet
the TB-related Millennium Development Goals WHO,
JANEVA
WHO, 2017; Global Actions and Investments Fall Far
Short of those Needed to End the Global TB
Epidemic. Global TB Report, WHO, Janeva
Effectiveness of the Role of the Family-based as Observer Direct Treatment for Tuberculosis Transmission Control
27
