
Increasing Health Care Provider Awareness on Cardiovascular
Disease by Malang Cardiovascular Networking System
Astrid Pramudya
1,2
, Mohammad Saifur Rohman
1,2
, Muhamad Rizki Fadlan
1,2
,
Liemena Harold Adrian
1,2
, Faris Wahyu Nugroho
1,2
, Monika Sitio
1,2
,
Diah Ivanasari
1,2
and Ardani Galih Prakosa
1,2
,
1
Department of Cardiology and Vascular Medicine, Faculty of Medicine,
Brawijaya University - Dr. Saiful Anwar General Hospital, Malang East Java, Indonesia
2
Brawijaya Cardiovascular Research Center, Brawijaya University, Malang East Java, Indonesia
Keywords: Malang Cardiovascular Networking System, Health Care Provider Awareness, Referral System.
Abstract: The state of being great value of interacting and linking health care unit for the management of acute
coronary syndrome (ACS) and other cardiovascular diseases (CVD) have been highlighted in the 2012
guidelines by the European Society of Cardiology (ESC) on ST-segment elevation myocardial infarction
(STEMI). Our past study in Malang showed that lack of health care provider awareness contributes to high
mortality due to cardiovascular disease. Malang Cardiovascular Networking System in Malang, established
since 2015 facilitates referral for further management on a daily basis. A retrospective cohort study was
conducted on analysing chat consultation and advocacy through Malang Cardiovascular Networking System
using Whatsapp Messaging Application in Malang Raya Region for the period 2015–2019. Also,
electrocardiogram machine suggested local public policy to strengthen the networking system. ECG report
was sent to enhance the consultation. The increasing number of consultation was the primary end-point.
The proportion of consultation in patients with cardiovascular disease (CVD) increased significantly after
Malang Cardiovascular Networking System began. Daily consultation accepted on Malang Cardiovascular
Networking System was 5-10 consultation, 150-200 monthly consultation, and more than 2000 (n= 2.114)
consultation annually, with a total of consultation 8.456 consultations. Within 4 years, 2283 (27%) patients
were referred to RSSA with CVD problem, 1040 (12.3%) patients were ACS, and the rest was non ACS
(14.7%, n = 1243). The number of consultation was increased annually since 2015 with increase rate about
2.3%, 3.4%, and 5.6%, respectively. The number of ACS patients undergoing reperfusion strategy was
found increase after 4-years of updating knowledge and advocacy with rate 12.1 % compared to the first
year (P=0.046). Malang Cardiovascular Networking System significantly increased health care provider
awareness on cardiovascular disease by increasing the number of consultations and provider’s knowledge.
1 BACKGROUND
The state of being great value of interacting and
linking health care units for the management of
acute coronary syndrome (ACS) and other
cardiovascular diseases (CVD) have been
highlighted in the 2012 guidelines by the European
Society of Cardiology (ESC) on ST-segment
elevation myocardial infarction (STEMI) (Steg,
2012). The networking is aimed at providing optimal
care by minimizing delays and, thereby, improving
clinical outcomes. In the management of patients
with STEMI, primary percutaneous coronary
intervention (PPCI) is a preferred reperfusion
strategy and a better choice than pre- hospital
fibrinolysis or in-hospital fibrinolysis (Wallentin,
2014).
Malang Raya is a region in East Java, Indonesia,
encompassing the municipality of Malang. Malang
has a mountainous area, also southern coast
bordering Indian ocean. Malang and its suburb,
Batu, had total of population 3.465.004 (2017
census) with total area of 3.882,44 km
2
(Pemerintah
Kota Malang, 2019). In Malang, Saiful Anwar
General Hospital (RSSA) is the main center and top
referral hospital and the biggest percutaneous
coronary intervention (PCI) and cardiovascular
center, established at 2015 with more than 50 other
48
Pramudya, A., Rohman, M., Fadlan, M., Adrian, L., Nugroho, F., Sitio, M., Ivanasari, D. and Prakosa, A.
Increasing Health Care Provider Awareness on Cardiovascular Disease by Malang Cardiovascular Networking System.
DOI: 10.5220/0009388500480052
In Proceedings of the 4th Annual International Conference and Exhibition on Indonesian Medical Education and Research Institute (The 4th ICE on IMERI 2019), pages 48-52
ISBN: 978-989-758-433-6
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

hospitals and primary health care referring their
cardiovascular patients for PCI or further
management to RSSA.
Our past study in Malang showed that lack of
health care provider awareness contributes to high
mortality due to cardiovascular disease. Malang
Cardiovascular Networking System in Malang,
established since 2015 facilitates referral for further
management on a daily basis.
1.1 Aim
To obtain the relationship between health care
provider awareness on cardiovascular disease by
Malang Cardiovascular Networking System.
2 METHOD
A retrospective cohort study was conducted on
analyzing chat consultation and advocacy through
Malang Cardiovascular Networking System using
Whatsapp Messaging Application in Malang Raya
Region for the period 2015–2019. Whatsapp
messaging group consisted of three groups, Malang
regency, Batu City and Malang City. The group
member is general practitioners in primary health
care, clinics, Type D, C and B Hospital.
Besides, the Malang government policy and
task to complete all the public health care with one
electrocardiogram machine and routinely ECG
training to support and strengthen Malang ACS
networking existence (Dinas Kesehatan Kota
Malang, 2016). Whatsapp group received the data
transmitted from a previous health care center that
would refer the patient to RSSA. A pre-hospital data
included name, age, type of insurance, patient’s
general examination line subjective, objective (vital
sign, physical examination), supporting observation,
especially 12-lead ECG; chest X-Ray and laboratory
examination results. All the data is directly
transmitted from the group consultation centered in
RSSA cardiology unit, and skilled operators with
direct access to RSSA received and analyzing the
consultation. This method possibly decreasing the
delay between referral time and increasing response
and fast patient management tracks to bypass the
ER, or Catheterization laboratory (cath lab), or
Intensive Cardiovascular Care Unit (iCVCU).
Each consultation attached with
electrocardiogram patient’s result, and/or CXR of
the patient. was sent to the group. The increasing
number of consultation was the primary end-point.
This networking system also had annual training to
the GP all around Malang greater area. The big data
also conducted using hospital medical records. All
patients referred to RSSA included ACS and non
ACS patients who were admitted to RSSA from any
public health care, primary clinic, and hospital
operating under the area of Malang Cardiovascular
Networking System between the 3 May 2015 to 30
September 2019. We record and observe the
consultation data including age, genders, type of
cardiovascular disease (acute coronary syndrome
versus non acute coronary syndrome), date of
consultation, date of admission in RSSA, date of
discharge, managements and intervention types,
status of discharge.
We observed two primary indicators describing
the performance of the main targeted network, one
for care processes and one for outcomes, using as
dependent variables: The clinical characteristics and
proportion of patients with ACS and non ACS
admitted to RSSA, ACS treated with reperfusion
strategy, the recommended and standard treatment
choice of STEMI according to the guideline;
increasing number of consultation and referral cases.
To evaluate the relationships between the
performance indicators and awareness of health care
providers and to take the systematical structure of
the data into account, we performed multilevel
logistic regression with random intercepts for
hospitals, controlling for potential intra-hospital
correlations. Next, to investigate the gap in
outcomes and
the introduction of the network. We
performed data analyses using SPSS 22. All p-
values reported are two sided with significance
threshold of p < 0.05.
3 RESULTS
From the final analysis we found 8.456 consultations
within 4 years we accepted on Malang
Cardiovascular Networking System, with the
number of daily consultation was 5-10 consultation,
150-200 monthly consultation, and average annual
consultation was 2.114. At first year of its existence
there are 2017 consultation (2015-2016), 2060
(2016-2017), 2129 (2017-2018) and 2250
consultations in 2018-2019 (Figure 1). We noted it
increased significantly over time for 4 years, with
increase rate about 2.3%, 3.4%, and 5.6%,
respectively.
Increasing Health Care Provider Awareness on Cardiovascular Disease by Malang Cardiovascular Networking System
49
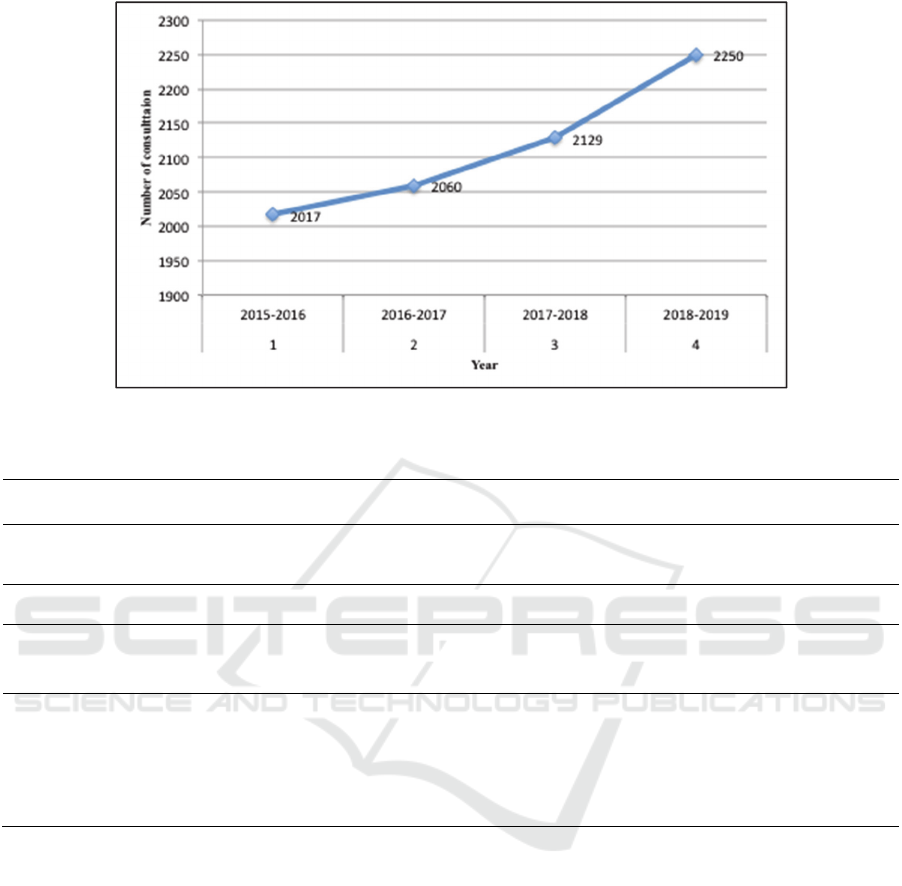
Figure 1: Number of consultation.
Table 1: Clinical Characteristics and Cases.
Variable 2015-2016
proportion (%)
2016-2017
proportion (%)
2017-2018
proportion (%)
2018-2019
proportion (%)
Total proportion
(%)
Number of
consultations
2.017 2.060 2.129 2.250 8.456
Referred to RSSA 474 (20.7) 515 (22.5) 635 (27.8) 659 (28.8) 2.283 (27)
Patient’s diagnosis
ACS
196 (41.3)
228 (44.3)
275 (43.3)
341 (51.8)
1040 (45.5)
Non ACS 278 (48.7) 287 (45.7) 360 (46.7) 318 (48.2) 1243 (54.5)
Management strategy
of ACS
Reperfusion
91 (46.2)
121 (53)
152 (55.2)
199 (58.3)
563 (44.1)
Non reperfusion 105 (43.8) 107 (47) 123 (54.8) 142 (41.7) 477 (45.9)
3.1 Clinical Characteristics
The total number of consultations has been increased
significantly, as we saw in Table 1. At its year of
launched, 2015-1016 there 2017 consultation, and in
the end of 4-years existence there were 2250
consultation (increased 11.5 %) at average the
number of patient referred to RSSA for further
treatment was 27% (2.283 cases) among 4 years.
From this group there were 1040 cases (45.4%), and
the rest was non ACS (54.5%) ACS.
The group of patients with non ACS cases was
mostly patient with heart failure, atrial fibrillation,
other arrhythmia disturbances, acute limb ischemia,
and any others cardiovascular disease. The patient
referred was 54.5 % (n=1243).
3.2 Management Strategy
The majority of ACS patients were diagnosed with
STEMI. Among those with STEMI, reperfusion was
not done in most patients. On most STEMI patients
referred for reperfusion strategy such as primary
percutaneous coronary intervention (PPCI), over
half of them were given fibrinolysis. The number of
reperfusion strategy was 44.1 % (563 cases) from
1.040 cases of ACS referred to RSSA, and the
remaining were not. It could be
Caused by the patient had been undergone a
PPCI or fibrinolytics from the previous hospital,
patients with autolysis STEMI, patients with onset
more than 3 days, or patients with conservative
treatment.
The 4th ICE on IMERI 2019 - The annual International Conference and Exhibition on Indonesian Medical Education and Research Institute
50

The number of ACS patients undergoing
reperfusion strategy was found to increase after 4-
years of updating knowledge and advocacy, with
rate 5.6% compared to the first year (P=0.046). The
awareness of health care providers was achieved on
their top level since their knowledge increased too.
Technology based management is significantly
support the successful of cardiovascular networking.
General practitioners and/or other specialists had
been more aware of cardiovascular disease
especially ACS cases.
According to the guideline, we fulfilled the
recommendation for the cardiovascular network,
especially reperfusion network to achieve speed
target time, delivery for cardiovascular disease
therapy. We were tailored network for the
community, and network itself respond to local
conditions and surroundings, easy to access, gain
support and acceptance from all stakeholders, and
adaptability to new knowledge.
Somehow, most parts of the world existed
cardiovascular networks are VIENNA STEMI
network and SAMU system in Europe, The Vital
Heart Network in Canada, and any other STEMI and
cardiovascular alert team in United States, India,
China, Russia, Australia, Latin America, and South
Africa.
Huber et al declared the essential ST-elevation
myocardial infarction system of care consist of
single telephone emergency number, ambulances
(vehicles, helicopters, planes), equipped with 12 lead
ECGs and defibrillators, and staffed with physicians
or well-trained paramedics, capable of basic and
advanced cardiac life support, occasionally
automatic ECG interpretation or ECG telemetry,
direct telephone access to catheterization laboratory,
protocols for standardized care, cardiologist or
intensive care specialist as a network leader,
involvement of healthcare authorities, public
information campaigns, regular meeting of involved
parties, and prospective registry (Abdul, 2019).
As cardiovascular networking system provided
those list above too, we already completed the
essential cardiovascular networking system and care
except the ambulances facility. Thus we relied social
messaging in order to make easier access to bigger
cardiovascular centers and shortening the delay.
More than that, beside its role on behalf to
management pre hospital of cardiovascular disease,
another possible function of cardiovascular network
was monitoring post discharge patients in primary
health care and home. The possible monitoring
checklist we can performed are cardiac symptoms,
physical and cardiac examination, drugs, and simple
cardiac rehabilitation at home. A study reported by
Chiantera et al. in Italy contemplate the use of ACS
networking and usual care, 63% of patients
discharged after ACS was found to exhibit cardiac
symptoms 1-month post discharge. ACS networking
was found to be able to slightly reduce hospital
readmissions (ACS networking 44% versus usual
care 56%) while at the same time better identifying
true from false angina among the patients (ACS
networking 85% true positive for cardiac cause
versus usual care 55%) (Chiantera, 2016).
4 CONCLUSION
Malang Cardiovascular Networking System
significantly increased health care provider
awareness on cardiovascular disease by increasing
number of consultation and provider’s knowledge.
Networking system like Malang Cardiovascular
network including electrocardiogram machine
facilities, and whatsapp group and bigger medical
center with catheterization laboratories facility along
24/7, and within a distance that can achieve
recommended transport are able to raise guideline
adherence and patient outcomes by streamlining the
critical pre- and intra-hospital processes as well as
improving timely access to invasive procedures,
recommended management and best outcome from
the patient.
ACKNOWLEDGEMENT
We would like to thank the Department of
cardiology and vascular medicine, faculty of
medicine Brawijaya University, dr. Saiful Anwar
general hospital Malang and the Malang
cardiovascular networking system for supporting in
the development of this manuscript.
REFERENCES
Abdul, M. K. (2019). Strengthening acute coronary
syndrome referral network: Insights from initiatives of
Penang General Hospital cardiology centre. The
Medical journal of Malaysia 74(4), pages 355–358.
Chiantera, A., Scalvini, S., Pulignano, G., Pugliese, M.,
De Lio, L., Mazza, A., et al. (2005). Role of
telecardiology in the assessment of angina in patients
Increasing Health Care Provider Awareness on Cardiovascular Disease by Malang Cardiovascular Networking System
51

with recent acute coronary syndrome. J Telemed
Telecare 11(Suppl 1).
Dinas Kesehatan Kota Malang. (2016). Pelatihan EKG
bagi tenaga paramedic di puskesmas. [Online]
Available from: https://dinkes.malangkota.go.id/2016/
08/29/pelatihan-ekg-untuk-tenaga-paramedis-di-puske
smas/ [Accessed 4th October 2019].
Huber, K., Gersh, B. J., Goldstein, P., Granger, C. B., &
Armstrong, P. W. (2014). The organization, function,
and outcomes of ST-elevation myocardial infarction
networks worldwide: current state, unmet needs and
future directions. European Heart Journal, 35(23),
pages 1526–1532.
O’Neill, D. E., Southern, D. A., Norris, C. M., O’Neill, B.
J., Curran, H. J., & Graham, M. M. (2014). Acute
coronary syndrome patients admitted to a cardiology
vs non-cardiology service: variations in treatment &
outcome. BMC health services research 17(1), pages
354.
Pemerintah Kota Malang. (2020) Sekilas Malang:
Geografi [Online]. Available from: https://
malangkota.go.id/sekilas-malang/geografis/ [Accessed
4th October 2019].
Saia, Mario, et al. (2018). Impact of the Regional Network
for AMI in the Management of STEMI on Care
Processes, Outcomes and Health Inequities in the
Veneto Region, Italy. International Journal of
Environmental Research and Public Health, 15.9: 1980.
Steg, P. G., James, S. K., Atar, D., Badano, L. P.,
Blömstrom-Lundqvist, C., et al. (2012). Task Force on
the management of ST-segment elevation acute
myocardial infarction of the European Society of
Cardiology (ESC), ESC guidelines for the
management of acute myocardial infarction in patients
presenting with ST-segment elevation. Eur Heart J,
33(20): 2569-619.
Sunjaya, A. P., Sunjaya, A. F., & Priyana, A. (2019).
Insights and challenges of indonesia’s acute coronary
syndrome telecardiology network: three year
experience from a single center and in west Jakarta,
Indonesia. IOP Conference Series: Materials Science
and Engineering Vol. 508, No. 1, pages 012142.
Wallentin, L., Kristensen, S. D., Anderson, J. L., Tubaro,
M., Sendon, J. L., Granger, C. B., et al. (2014). How
can we optimize the processes of care for acute
coronary syndromes to improve outcomes? Am Heart
J, 168(5): 622-31.
The 4th ICE on IMERI 2019 - The annual International Conference and Exhibition on Indonesian Medical Education and Research Institute
52
