
Scheduled Bulk SMS Program as Hypertension Education Media and
Medication Reminder in Puskesmas 2 East Denpasar
Hari Purnomo
1
, Fariz Afristya Putra
2
and Anindya Agripina Hadyanawati
1
1
Industrial Engineering, Universitas Islam Indonesia, Sleman, Yogyakarta, Indonesia
2
Field Epidemiology, Universitas Udayana, Denpasar, Bali, Indonesia
Keywords: Automated, Text Messaging, Medication, Adherence, Health Education, Hypertension
Abstract: This research is an operational research aimed to evaluate ongoing scheduled bulk SMS program in
Puskesmas 2, East Denpasar. The evaluation comprised of health education media and medication reminder.
Research was held prospectively with multiple posttest method. Within one-year evaluation of program
implementation, 90 people satisfy the research criteria and managed to follow the procedure to the end of
research. Questionnaire result from four examination (pretest and three times posttest) statistically analyzed
using ANOVA with repeated values. Research result showed that scheduled bulk SMS Program statistically
significant to improve perception about their medication regiment (as a health education media) (F (1.928;
171.594) = 171.509, p<0.005), and statistically significant to increase medication adherence (as a medication
reminder) (F (2.495; 222.092) = 149.293; p<0.005).
1 INTRODUCTION
Cardiovascular disease mainly caused or made
worse by uncontrolled high blood pressure, even
some research boldly stated that blood pressure is
directly correlated with cardiovascular mortality risk
(Lewington et al., 2002). Importance of controlling
blood pressure emphasized when it was found that
cardiovascular disease chance is decreased when
patient manage to control their blood pressure
(Staessen, Wang and Thijs, 2001; Staessen et al.,
2005) independently whether the patient manage to
control their obesity and diabetes or not (Anand and
Yusuf, 2011).
Management of high blood pressure is not as
simple as taking medicine to treat the disease. Two
important management need to be done daily to
maintain low blood pressure, which are daily
adherence to suggested blood pressure medication
(Neal et al., 2000), and life style changes to eliminate
risk factors, such as alcohol and smoking (Whitworth
and World Health Organization, 2003; Staessen et al.,
2005). Those two-management synergy needs to be
maintained in long term to decrease cardiovascular
disease morbidity and mortality.
A lot of intervention already been used to improve
adherence, both for treatment and life style change
with mixed and varying result (Haynes et al., 2008).
Lately medical treatment trend also undergoes
digitalization. With worldwide access of mobile
phone, lately it’s more difficult to find patient with no
access to mobile phone. Mobile phone already used
before as medication support, lifestyle education
delivery, discussion media with health care providers,
or independent individual searches of health issues in
Internet (Heron and Smyth, 2010).
According to Indonesia’s Ministry of
Communication and Informatics by the end of 2017,
371.4 million people have already had access to
mobile phone, this is very big, considering total
population of Indonesia at the time were 262 million
(Kementerian Komunikasi dan Informatika Republik
Indonesia, 2019). That means 142% of Indonesian
population have access to personal communication
device by the end of 2017 or on average 1.4 phones
per person. This is possible as more and more people
have multiple phone for different purposes. Further
reading showed that only around 43% of that
population have access to internet and social media,
that means only half of Indonesia population have
smartphones (Statista, 2019). As access of
smartphones are limited, basic mobile phone services
(phone calls, or short message services) are probably
have better penetration compared with internet-based
services.
Purnomo, H., Putra, F. and Hadyanawati, A.
Scheduled Bulk SMS Program as Hypertension Education Media and Medication Reminder in Puskesmas 2 East Denpasar.
DOI: 10.5220/0009352900250032
In Proceedings of the International Conferences on Information System and Technology (CONRIST 2019), pages 25-32
ISBN: 978-989-758-453-4
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
25

Researches based on Short Message Service
(SMS) to improve adherence have varying result
worldwide, but so far writer haven’t found proper
similar research in Indonesia. To name a few,
significant research result are from Russia (Kiselev et
al., 2012), China (Lin et al., 2014), and South Korea
(Park and Kim, 2012). Not significant results are from
Pakistan (Mohammed, Glennerster and Khan, 2016),
Spain (Márquez Contreras et al., 2004; Carrasco et
al., 2008), and Philippines (Philipines Department of
Health, 2017). As previous researches were not
yielding coherence and similar result, writer speculate
there are region specific causes that causes different
results. Parallel with writer’s speculation, similar
effort to improve adherence using SMS is performed
by one of primary health care (puskesmas) in
Denpasar, Bali. Writer then collaborate with said
primary health care to evaluate program’s result.
2 MATERIALS AND METHODS
2.1 Participants, Questionnaire, and
SMS Program
Research subjects are all patients treated in
Puskesmas 2, East Denpasar who meet the research
criteria. Inclusion criteria were as follows: (1) over 18
years old (2) diagnosed as hypertension patient (3)
receiving drugs and medication from Puskesmas 2,
East Denpasar (4) literate, able to read (5) possess cell
phone / smartphone. Exclusion criteria are also added
to prevent result alteration: (1) palliative patient with
life expectancy under one-year (2) patient also
diagnosed with other chronic illnesses (diabetes,
cancer, COPD) (3) dementia or with severe mental
disorder. Control group was not formed, as this
research is an evaluation of Puskesmas’ new program
to promote health, so all patients are included in the
program. This attempt to increase treatment
adherence were one of Puskesmas’ innovation in
yearly Outstanding Puskesmas contest.
There were two questionnaires used in this
research, one for evaluating subject’s attitude about
their medication regiment, and one for evaluating
subjective medical adherence of each patient.
Assessing attitude and knowledge of research
subjects done using Indonesian adaptation of 30
questions Drug Attitude Inventory (DAI30) (Hogan,
Awad and Eastwood, 1983). Adherence to
medication was scored using Morisky’s 8 Items
Medication Adherence Scale (MMAS-8) (Morisky et
al., 2008). These two-questionnaire tested for validity
and reliability after translation, resulted in no needs
for further editing aside from translation into
Indonesian language.
Scheduled bulk SMS program were not built by
writer, the program used was paid Android phone
(Google, 2019) based program named Pulse (Klinker,
2019). Pulse was selected because of their useful
feature within scope of this research. Features used in
this research are: (1) scheduled SMS (2) bulk SMS
option and grouping (3) repeat SMS option (4)
automatic response by sender and by keyword (5)
scheduling can be performed with other devices
without changing phone number.
2.2 Research Procedure
This is an operational research using prospective
analytic research with multiple posttest method
without control group, held within February 2018
until February 2019 time span. All hypertension
patients who came to check their health and procuring
routine medicine in February 2018 (28 days) are
invited into this research, before continuing, they are
screened through inclusion criteria, exclusion criteria,
and signing informed consent. Patients unwilling to
join with any reason are convinced that they’re going
to have the same treatment as usual with patients who
joins this research. This was to ensure that no patient
feels forced to join, while medical adherence is also
affected by patient’s willingness to follow up through
their treatment regimen.
Patients who join this research then interviewed
for their demographic data (including age, sex,
marriage status, education status, occupation, health
insurance, medication used, medical complication,
phone number, type of phone used, and phone signal
around home), and baseline data as a pretest score
using adapted DAI30 (patient’s attitude toward their
medication) and MMAS-8 (patient’s adherence
toward their medication) into Indonesian language.
After one-month process of screening and
acquiring baseline pretest data in February 2018,
scheduled bulk SMS program were performed.
Patients are grouped by what kind of medications are
they on, and date of follow up to puskesmas for their
illness, then they will get targeted SMS based on their
group to help improve their treatment adherence. For
education purpose, patients are not grouped and
receiving the same SMS. There are several types of
SMS patients receive throughout this research those
are:
Reminder for medication time (specific for
each patient’s medication regiment)
Reminder for illness follow up to puskesmas
date and procuring more medicine (SMS sent
CONRIST 2019 - International Conferences on Information System and Technology
26
five days, three days, and one day before
following up date for each patient)
Short education about illness they suffer,
medication taken, and healthy lifestyle (3-4
times per week)
Evaluation to check whether SMS sent manage to
affect perception towards treatment regimen and
medication adherence (posttest) was done three times,
on June 2018, September 2018 and February 2019.
Software used to analyze pretest and posttest data are
Ms. Excel (Microsoft, 2019) and SPSS (IBM, 2019).
Statistical analysis was done using ANOVA with
repeated measures to know whether any data changes
between test are statistically significant or not.
Demographic descriptive analysis data will be
presented as is, or as percentage.
3 RESULT AND DISCUSSION
3.1 Research Participants
Within one month of collecting baseline data, 98
patients are registered to join this research, but only
90 patients (91%) are able to finish through all
posttest. From those eight people who didn’t manage
to finish this program, one died, one admitted to
hospital because of stroke, and six lost to follow up.
Table 1 shows demographic and baseline data of
research participants who managed to join the
program for one full year and finished three follow
ups.
Table 1. Baseline Characteristics, n=90
Age
Mean
Std Deviation
Range
(Y.O)
53.3
14.2
30-79
Years
Diagnosed
Mean
Std Deviation
Range
(year)
3.5
2.2
1-9
Sex
Male
Female
35.6%
64.4%
Complication
Yes
No
34.4%
65.6%
Marriage
Not Married
Married
Widowed
6.7%
58.9%
34.4%
Ever Change
Medication
Yes
No
23.3%
76.7%
Education
None
Elementary
Junior High
Senior High
Bachelor
Post Grad.
15.6%
31.1%
25.6%
15.6%
10.0%
2.2%
Phone Type
Handphone
Smartphone
61.1%
38.9%
Occupation
Informal
Private Sect.
Civil Sector
Professional
Entrepreneur
Unemployed
34.4%
22.2%
5.6%
8.9%
11.1%
17.8%
Bad Phone
Signal
Yes
Sometimes
No
20.0%
70.0%
10.0%
Medication
Amlodipine
Captopril
20%
80%
Keep Phone
Near
Yes
No
53.3%
46.7%
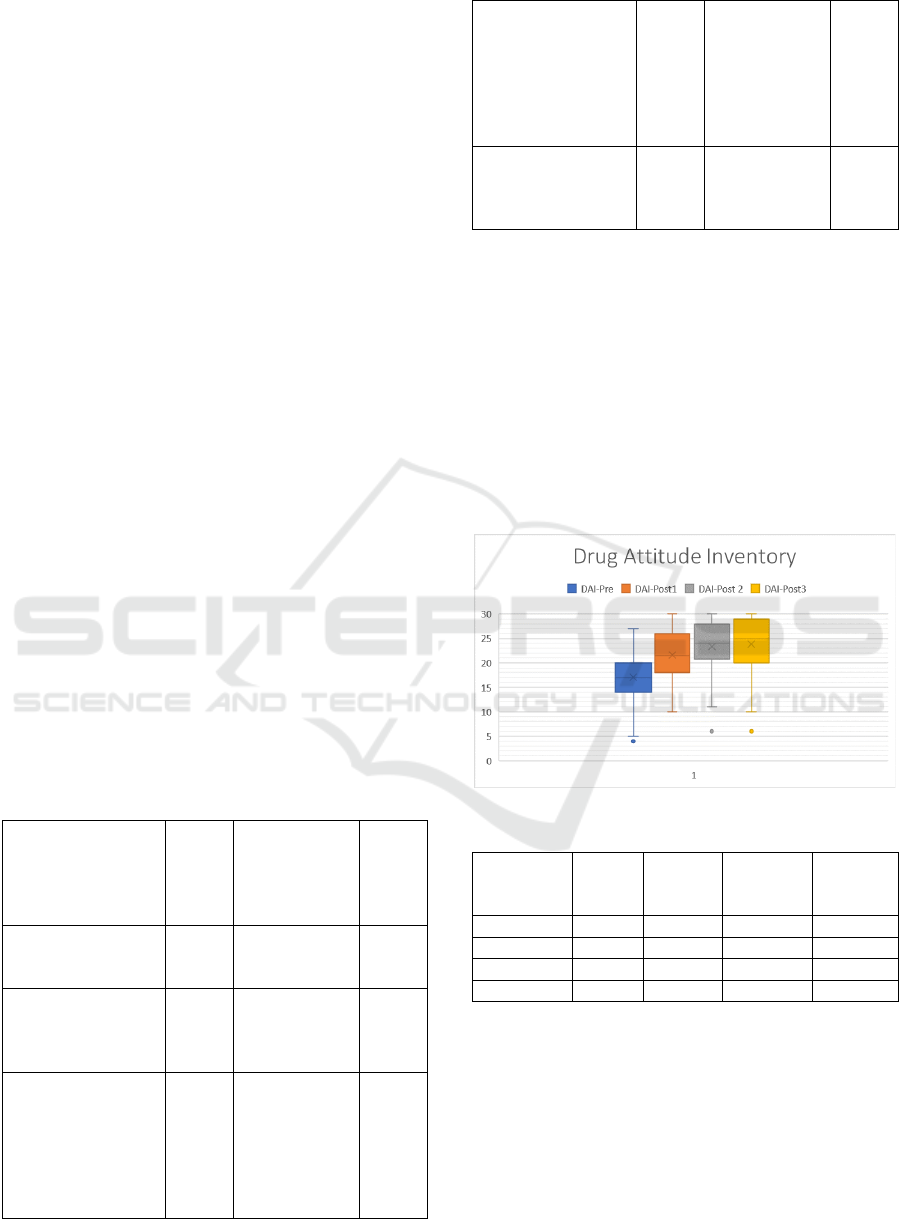
3.2 Drug Attitude Inventory
Drug Attitude Inventory is an adapted
questionnaire used to define patient’s perception and
their level of trust to medication. Higher score
associated with higher level of trust, and vice versa,
lower score associated with lower level of trust to
their medication. Figure 1 and Table 2 are boxplot
and mean table for four data result (pretest, posttest 1,
posttest 2, posttest 3) using this questionnaire.
Fig. 1. DAI 30 Mean Result
Table 2. DAI 30 Descriptive Statistics
Mean
Std.
Dev.
N of
Max
Score
Δ with
prior
exam.
Pretest
17.066
4.7612
0
Posttest 1
21.588
5.1970
8
4.5222
Posttest 2
23.355
5.4511
17
1.7667
Posttest 3
23.844
5.8883
18
0.4888
Boxplot diagram shows that there was
considerable elevation of score from pretest to
posttest 1. However, the increment of score result
tends to decrease in posttest 2 and become negligible
in posttest 3. With continuous increment of mean
score within this research, ANOVA with repeated
measure was performed to ensure whether those
increment are statistically significant or not. Table 3-
5 shows the result of said statistical analysis:
Scheduled Bulk SMS Program as Hypertension Education Media and Medication Reminder in Puskesmas 2 East Denpasar
27
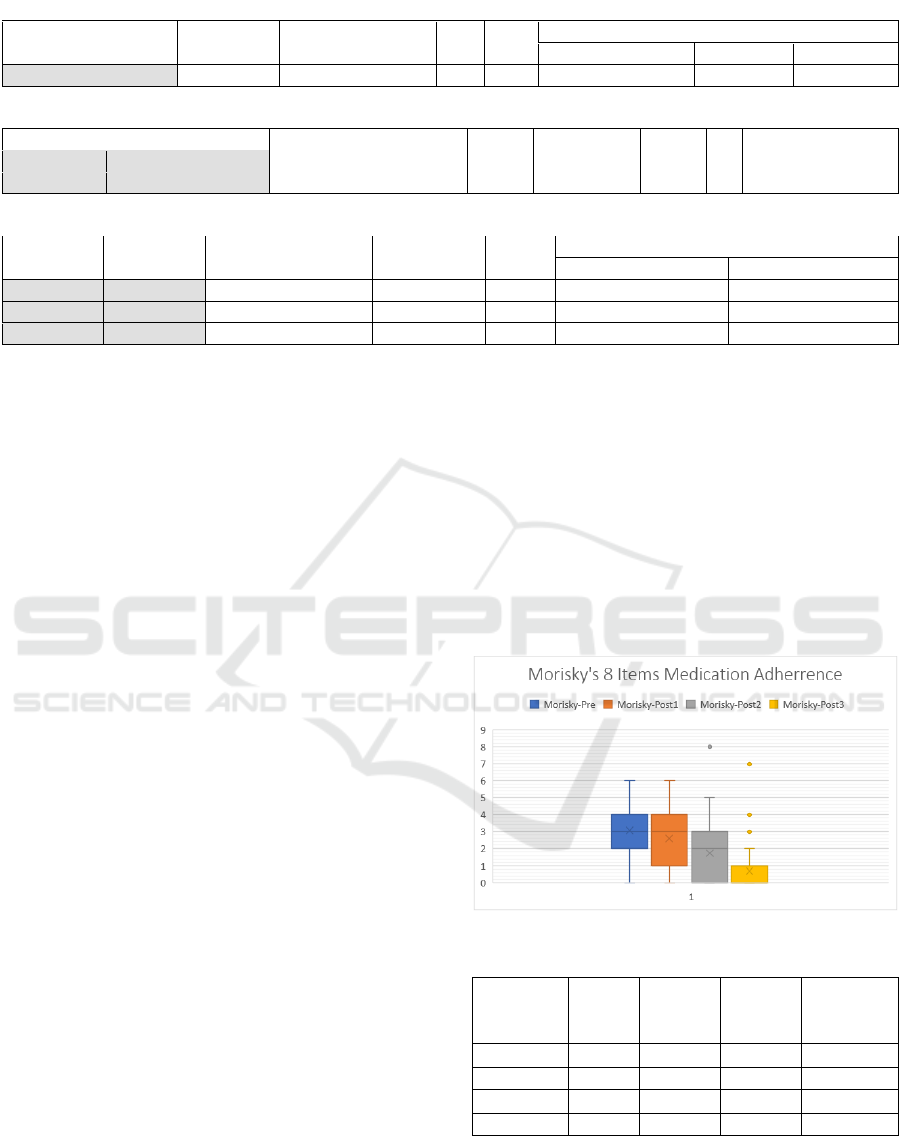
Table 3. DAI 30 Mauchly's Test of Sphericity
Within Subjects Effect Mauchly's W
Approx. Chi-Square
df Sig.
Epsilon
Greenhouse-Geisser
Huynh-Feldt
Lower-bound
Time
0.415
77.148
5
0.000
0.643
0.657
0.333
Table 4. DAI 30 Anova with Repeated Measures
Source
Type III Sum of Squares
df
Mean Square
F
Sig.
Partial Eta Squared
Time
Greenhouse-Geisser
2573.697
1.928
1334.891
171.509
.000
.658
Error (Time)
Greenhouse-Geisser
1335.553
171.594
7.783
Table 5. DAI 30 Bonferroni Post Hoc
(I) Time
(J) Time
Mean Difference
(I-J)
Std. Error
Sig.
95% Confidence Interval for Difference
Lower Bound
Upper Bound
1
2
-4.522
*
.307
.000
-5.351
-3.693
2
3
-1.767
*
.242
.000
-2.419
-1.114
3
4
-.489
.227
.206
-1.103
.125
Mauchly's Test of Sphericity (Table 3)
indicated that the assumption of sphericity had been
violated (X
2
=0.415, p<0.005). Because sphericity had
been violated, Anova with repeated measure result
should be corrected. Greenhouse-Geisser correction
was chosen because it resulted in epsilon of 0.643.
Greenhouse-Geisser adjustment on ANOVA
with repeated measure result shows, in general mean
value of DAI30 statistically differs between each
examination time (F (1.928; 171.594) = 171.509,
p<0.005) (Table 4). Mean score increment of DAI30
are observeable from pretest until all three posttest as
can be seen on Table 2, respectively, 17.1±4.8;
21.6±5.2; 23.4±5.5 ; 23.8±5.9.
However, even though increment may always
be observed, not all of them are statistically
significant (Table 5). Significant score increase can
be seen on pretest to posttest 1 with mean difference
of -4.522±0.307 (p<0.005), and posttest 1 to posttest
2 -1.767±0.243 (P<0.005), unfortunately score
difference between posttest 2 and posttest 3 is not
significantly differs -0.489±0.227 (p=0.206).
As statistical analysis result showed,
scheduled bulk SMS program has better efficacy on
the beginning of program, and slowly recede towards
the end of 1-year period. However, this probably
happened because max score of DAI30 questionnaire
already reached by most subjects by the end of
research, this leads to stagnation of mean score as no
additional score may be achieved by subjects.
Perhaps further research should be performed to
establish whether after program ended, patient still be
able to maintain their high attitude toward
medication, or perhaps this program should be
continued to maintain program result.
3.2 Morisky’s Eight Items Medical
Adherence
Morisky’s Eight Item Medical Adherence
measures patient’s medication adherence. Different
with DAI30, M8MA score interpreted as better if
lower score is achieved. This because M8MA asks
about factors that promote medication
inconsistencies, more factors helped inconsistencies
means worse medication adherence rate. Below is
boxplot diagram and mean result of M8MA
questionnaire from pretest to the third posttest.
Fig. 2. M8MA mean result
Table 6. M8MA Descriptive Statistics
Mean
Std.
Dev.
N of
Max
Score
Δ with
prior
exam.
Pretest
3.0078
1.21070
1
Posttest 1
2.6000
1.50505
6
0.4078
Posttest 2
1.7444
1.53287
25
0.8556
Posttest 3
0.6778
1.22546
58
1.0666
As can be seen from previous Figure 2 and
Table 6, score reduction always happened between
time period, and the difference keeps getting larger
after each posttest. Even from pretest, there was
already one sample with max adherence, and the
CONRIST 2019 - International Conferences on Information System and Technology
28

number of patients with max adherence keeps
gradually increasing towards the end of research.
Mean scores are pretest 3.0078±1.21070, posttest 1
2.6000±1.50505, posttest 2 1,7444±1.53287, and
posttest 3 0.6778±1.22546.
Mauchly’s test of sphericity in Table 7
indicates that the assumption of sphericity had been
violated, with result of X
2
=0.635; p<0.005. Huynh-
Feldt correction is chosen to adjust result of ANOVA
with repeated measures as it produced epsilon of
0.832.
ANOVA with repeated measures with Huynh-
Feldt correction (Table 8) shows that mean score of
M8MA statistically differs between each examination
time (F (2.495; 222.092) = 149.293; p<0.005).
Significant score reduction of M8MA (increasing
adherence) are observed via Post Hoc test using
Bonferroni correction on all four tests performed
(Table 9). The score difference are 0.478±0.111
(p<0.005) between pretest and posttest 1,
0.856±0.093 (p<0.005) between posttest 1 and
posttest 2, lastly 1.067±0.107 (p,0.005) between
poosttest 2 and posttest 3.
This program tends to have better effect on
M8MA score approaching the end of research, with
more than 50% of patient managed to get full
adherence by the end of research. This result differs
with DAI30 that have better score increment in the
beginning of research.
3.2 Discussions
Scheduled bulk SMS program have positive
effect to patient’s perception of their medication
(DAI8) as well as the level of medication adherence
(M8MA). However, said positive effect seems have
different pattern in long term and long term. DAI8’s
score increment tends to decrease along the time
points (Δ pretest-posttest 1 = 4.5222; Δ posttest 1-
posttest 2 = 1.7667; Δ posttest 2-posttest 3 = 0.4888).
Meanwhile, SMS manage to increase patient’s
adherence better in long run (Δ pretest-posttest 1 =
0.4078; Δ posttest 1-posttest 2 = 0.8556; Δ posttest 2-
posttest 3 = 1.0666).
This difference of effect by time period may
have happened because there are different
fundamental goals of SMS program between
educating and reminding patients. Education
functions as new information giver thus may lead to
saturated information, in which no new information
are received by patients. Reminder on the other hand,
is aimed to help patient remember when to take their
medication, so repeated exposure may help increase
adherence better.
Similar approach of study based around SMS
to improve adherence tends to have various result.
Further reading suggested that SMS program have
better effect on medication adherence in a large
countries such as Russia (Kiselev et al., 2012) and
China (Lin et al., 2014). Smaller countries inclined to
have less positive effect from SMS intervention, such
as research in Spain (Carrasco et al., 2008) (Márquez
Contreras et al., 2004), Pakistan (Mohammed,
Glennerster and Khan, 2016), and Philippines
(Philipines Department of Health, 2017). Other factor
that may influence research is length of study, better
result can be observed in research with more than six
months intervention (Kiselev et al., 2012; Lin et al.,
2014; Márquez Contreras et al., 2019) compared with
less than six months intervention (Márquez Contreras
et al., 2004; Philipines Department of Health, 2017).
Table 7. Mauchly's Test of Sphericity
Within Subjects
Effect
Mauchly's W Approx. Chi-Square
df Sig.
Epsilon
Greenhouse-Geisser
Huynh-Feldt
Lower-bound
Time
.635
39.882
5
.000
.808
.832
.333
Table 8. M8MA Anova with Repeated Measures
Source
Type III Sum of Squares
df
Mean Square
F
Sig.
Partial Eta Squared
Time
Huynh-Feldt
299.942
2.495
120.197
149.293
0.000
0.627
Error (Time)
Huynh-Feldt
178.808
222.092
0.805
Table 9. M8MA Post Hoc Bonferonni
(I) Time (J) Time Mean Difference (I-J) Std. Error Sig.
b
95% Confidence Interval for Difference
Lower Bound
Upper Bound
1
2
0.478
0.111
0.000
0.179
0.777
2
3
0.856
0.093
0.000
-.605
1.106
3
4
1.067
0.107
0.000
0.778
1.355
Scheduled Bulk SMS Program as Hypertension Education Media and Medication Reminder in Puskesmas 2 East Denpasar
29

Previous researches support our research
result, Indonesia is a large country with thousands of
islands (Nurul Fitri Ramadhani, 2017), this leads to
better SMS reach area compared with countries with
smaller area. As previously mentioned in
introduction, SMS was chosen as media because of its
accessibility and cost. This research also reinforces
previous research result that longer intervention by
SMS performed evidently helped patients to maintain
their medication adherence.
There are several research limitations that
needs to be considered. First one is presence of outlier
data in this research. With the ongoing increment
score of DAI30 there were always outliers with very
low score along the research, similar with DAI30,
M8MA also have several outliers within the group but
writer notices different pattern of outlier. DAI30 have
outliers on all time points from pretest to the third
posttest, but in M8MA outliers only happened on
second and third posttest. By analyzing bottom 5
score acquirer, there are at least two people that
constantly getting low score. Furthermore, their
scores are not constantly increasing as other
participants do.
There are several possible reasons why this
happened, language barrier, weak comprehension to
the questions and laziness and/or ignorance to follow
order of research. Language barrier happened because
even though the questionnaire already translated into
Indonesian language, and Indonesian language is the
national language in the country, there are minority of
the population (especially geriatrics) who only
understand local languages (Cohn and Ravindranath,
2014). Geriatrics also have other problems aside from
language disparity that affects questionnaire result,
such as vision degeneration (Saw et al., 2003),
cognitive impairment (Mardiyanto, Jahja and
Limyati, 2017), or both (Ong et al., 2012). Other
factor author managed to grasp was laziness of the
respondents. With total of 38 questions to answer -if
each question is to be read in at least 15 until 30
seconds- respondents needs at least 10 minutes to
finish, but there are several respondents that submit
the paper within 2-3 minutes. This may be because of
laziness or ignorance to the questionnaire result.
Further research should address the same problem if
happened by eliminating those samples or performing
in depth interview to understand factors affecting
program efficacy.
Second research limitation is there were no
control group in this research because the nature of
this research as an operational research to evaluate
ongoing program performed on all patient in the
primary health care. Third research limitation is this
research only performed in one health center. Second
and third research limitation may be diminished by
larger research on multiple health center using
randomized controlled trial.
4 CONCLUSION
To conclude this research, scheduled bulk
SMS program is statistically significant to increase
DAI30 score (increase medication perception) and
decrease M8MA score (increase medication
adherence) (F (1,928; 171,594) = 171,509, p<0,005
and F (2,495; 222,092) = 149,293; p<0,005
respectively). This program is advised to be adapted
in larger scale and longer term, seeing SMS program
inclined to perform better in larger area and
continuously. Since this method have high
effectiveness despite the low cost, primary health care
may be able to deliver better result compared with
secondary and tertiery health center or hospital, as
most long-term treatment of chronic illnesses patients
are treated within the scope of primary health care.
COMPETING INTEREST
Authors hereby declare that they have no
competing interests.
ACKNOWLEDGEMENTS
We are grateful to all patients who
participated, all health care workers in Puskesmas II
East Denpasar, especially to the doctors: dr. I Made
Buda Wisnawa, M.Kes.; dr. Anik Rosida ; dr. Ni
Wayan Kandita Arumdani. Also we are grateful to
Pulse Software developer Luke Klinker for giving us
permission to use the software.
REFERENCES
Anand, S. S. and Yusuf, S. (2011) ‘Stemming the
global tsunami of cardiovascular disease’, The Lancet,
377(9765), pp. 529–532. doi: 10.1016/S0140-
6736(10)62346-X.
Carrasco, M. P. et al. (2008) ‘Impact of Patient–
General Practitioner Short-Messages-Based Interaction on
the Control of Hypertension in a Follow-up Service for
Low-to-Medium Risk Hypertensive Patients: A
CONRIST 2019 - International Conferences on Information System and Technology
30

Randomized Controlled Trial’, IEEE Transactions on
Information Technology in Biomedicine, 12(6), pp. 780–
791. doi: 10.1109/TITB.2008.926429.
Cohn, A. C. and Ravindranath, M. (2014) ‘Local
languges in Indonesia: Language maintenance or language
shift?’, Linguistik Indonesia, 32(2), pp. 131–148. Available
at: http://www.mlindonesia.org/images/files/Agustus
2014.pdf#page=33.
Google (2019) Mobile Operating System - Android.
Available at: https://www.android.com/ (Accessed: 28 June
2019).
Haynes, R. B. et al. (2008) ‘Interventions for enhancing
medication adherence’, Cochrane Database of Systematic
Reviews, (2), p. CD000011. doi:
10.1002/14651858.CD000011.pub3.
Heron, K. E. and Smyth, J. M. (2010) ‘Ecological
momentary interventions: Incorporating mobile technology
into psychosocial and health behaviour treatments’, British
Journal of Health Psychology, 15(1), pp. 1–39. doi:
10.1348/135910709X466063.
Hogan, T. P., Awad, A. G. and Eastwood, R. (1983) ‘A
self-report scale predictive of drug compliance in
schizophrenics: reliability and discriminative validity.’,
Psychological medicine, 13(1), pp. 177–83. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/6133297 (Accessed:
27 June 2019).
IBM (2019) SPSS Software - IBM. Available at:
https://www.ibm.com/analytics/spss-statistics-software
(Accessed: 29 June 2019).
Kementerian Komunikasi dan Informatika Republik
Indonesia (2019) Laporan Tahunan Ditjen
Penyelenggaraan Pos dan Informatika (PPI) Tahun
Anggaran 2017, KemKomInfo. Available at:
https://www.kominfo.go.id/content/all/laporan_tahunan
(Accessed: 18 July 2019).
Kiselev, A. R. et al. (2012) ‘Active ambulatory care
management supported by short message services and
mobile phone technology in patients with arterial
hypertension’, Journal of the American Society of
Hypertension, 6(5), pp. 346–355. doi:
10.1016/j.jash.2012.08.001.
Klinker, L. (2019) Pulse SMS Application. Available
at: https://messenger.klinkerapps.com/overview/
(Accessed: 28 June 2019).
Lewington, S. et al. (2002) ‘Age-specific relevance of
usual blood pressure to vascular mortality: a meta-analysis
of individual data for one million adults in 61 prospective
studies.’, Lancet (London, England), 360(9349), pp. 1903–
13. doi: 10.1016/s0140-6736(02)11911-8.
Lin, P.-H. et al. (2014) ‘A text messaging-assisted
randomized lifestyle weight loss clinical trial among
overweight adults in Beijing’, Obesity, 22(5), pp. E29–E37.
doi: 10.1002/oby.20686.
Mardiyanto, F. Y., Jahja, D. S. and Limyati, Y. (2017)
‘Factors Related to Cognitive Function in Elderly People’,
Journal Of Medicine & Health, 1(6). doi:
10.28932/jmh.v1i6.547.
Márquez Contreras, E. et al. (2004) ‘[Effectiveness of
an intervention to provide information to patients with
hypertension as short text messages and reminders sent to
their mobile phone (HTA-Alert)].’, Atencion primaria,
34(8), pp. 399–405. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/15546536
(Accessed: 16 July 2019).
Márquez Contreras, E. et al. (2019) ‘Specific
hypertension smartphone application to improve
medication adherence in hypertension: a cluster-
randomized trial’, Current Medical Research and Opinion.
Taylor & Francis, 35(1), pp. 167–173. doi:
10.1080/03007995.2018.1549026.
Microsoft (2019) Spreadsheet Software - Microsoft
Excel. Available at: https://products.office.com/en/excel
(Accessed: 29 June 2019).
Mohammed, S., Glennerster, R. and Khan, A. J. (2016)
‘Impact of a Daily SMS Medication Reminder System on
Tuberculosis Treatment Outcomes: A Randomized
Controlled Trial’, PLOS ONE. Edited by L. Gao. Public
Library of Science, 11(11), p. e0162944. doi:
10.1371/journal.pone.0162944.
Morisky, D. E. et al. (2008) ‘Predictive validity of a
medication adherence measure in an outpatient setting.’,
Journal of clinical hypertension (Greenwich, Conn.). NIH
Public Access, 10(5), pp. 348–54. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/18453793
(Accessed: 28 June 2019).
Neal, B. et al. (2000) ‘Effects of ACE inhibitors,
calcium antagonists, and other blood-pressure-lowering
drugs: results of prospectively designed overviews of
randomised trials. Blood Pressure Lowering Treatment
Trialists’ Collaboration.’, Lancet (London, England),
356(9246), pp. 1955–64. doi: 10.1016/s0140-
6736(00)03307-9.
Nurul Fitri Ramadhani (2017) 16,000 Indonesian
islands registered at UN, The Jakarta Post. Available at:
https://www.thejakartapost.com/news/2017/08/21/16000-
indonesian-islands-registered-at-un.html (Accessed: 16
July 2019).
Ong, S. Y. et al. (2012) ‘Visual Impairment, Age-
Related Eye Diseases, and Cognitive Function’, Archives of
Ophthalmology. American Medical Association, 130(7),
pp. 895–900. doi: 10.1001/archophthalmol.2012.152.
Park, M.-J. and Kim, H.-S. (2012) ‘Evaluation of
mobile phone and Internet intervention on waist
circumference and blood pressure in post-menopausal
Scheduled Bulk SMS Program as Hypertension Education Media and Medication Reminder in Puskesmas 2 East Denpasar
31

women with abdominal obesity’, International Journal of
Medical Informatics, 81(6), pp. 388–394. doi:
10.1016/j.ijmedinf.2011.12.011.
Philipines Department of Health (2017) ‘Effectiveness
of SMS Text Reminders to Improve Blood Pressure Among
Patient...: All Library Resources at PGIMER’, Clinical
Trial. Available at:
https://clinicaltrials.gov/ct2/show/study/NCT01255436
(Accessed: 16 July 2019).
Saw, S.-M. et al. (2003) ‘Causes of low vision and
blindness in rural Indonesia’, British Journal of
Ophthalmology. BMJ Publishing Group Ltd, 87(9), pp.
1075–1078. doi: 10.1136/BJO.87.9.1075.
Staessen, J. A. et al. (2005) ‘Blood Pressure Reduction
and Cardiovascular Prevention: An Update Including the
2003-2004 Secondary Prevention Trials’, Hypertension
Research, 28(5), pp. 385–407. doi: 10.1291/hypres.28.385.
Staessen, J. A., Wang, J.-G. and Thijs, L. (2001)
‘Cardiovascular protection and blood pressure reduction: a
meta-analysis’, The Lancet, 358(9290), pp. 1305–1315.
doi: 10.1016/S0140-6736(01)06411-X.
Statista (2019) Smartphone user penetration in
Indonesia 2014-2019, 2019. Available at:
https://www.statista.com/statistics/257046/smartphone-
user-penetration-in-indonesia/ (Accessed: 18 July 2019).
Whitworth, J. A. and World Health Organization, I. S.
of H. W. G. (2003) ‘2003 World Health Organization
(WHO)/International Society of Hypertension (ISH)
statement on management of hypertension.’, Journal of
hypertension, 21(11), pp. 1983–92. doi:
10.1097/01.hjh.0000084751.37215.d2.
CONRIST 2019 - International Conferences on Information System and Technology
32
