
Effects of Visual Imagery Techniques on Improving Motor Function
of Upper Limb in Chronic Ischemic Stroke Patients:
A Serial Case Report
Edwin Goutama
1
, Steven Setiono
1
1
Department of Physical Medicine and Rehabilitation, Dr. Cipto Mangunkusumo Hospital,
University of Indonesia, Jakarta, Indonesia
Keywords: Chronic Ischemic Stroke, Motor Function, Upper Limb, Visual Imagery.
Abstract: The aim of this study is to report our success in improving the motor function of the paresis hand of chronic
stroke patients using visual imagery techniques. Three patients with chronic ischemic stroke were given
visual imagery therapy carried out twice over three weeks, without stopped the occupational therapy. At the
end of the treatment, an increase in hand function was found in all three cases, using the DASH
questionnaire. In the first case, there was a significant increase in hand function in the activities of holding a
motorcycle and car steering wheel, holding a shopping bag, and cleaning hair. In the second case, there was
an increase in the function of opening and closing the jar, opening the lock, opening the door handle,
attaching the object to the rack, cleaning the back, and holding the motor steering wheel. In the third case,
improved hand function was found in carrying heavy objects, shopping bags, and wearing clothes. There
was no decrease in hand function reported in all three cases after the administration of visual imagery
therapy. This shows that visual imagery therapy as an adjunctive rehabilitation treatment to motor function
in patients with chronic ischemic stroke gives good results.
1 INTRODUCTION
Stroke is the second highest cause of death, and the
third highest cause of disability in the world
(Johnson, et al, 2016). The impact of disability will
hamper daily activities and patient’s readiness to
return to their social environment. One of the
disabilities due to stroke is impaired motor function
of the upper limb. Rehabilitation of upper limb
motor function becomes important because it
supports the activities of daily living (ADL), such as
eating and drinking, wearing clothes, bathing,
combing hair, and so on (Venketasubramanian et al.,
2017). Occupational therapy has been an option as a
task-oriented training in rehabilitation of upper limb
motor functions (Hatem et al., 2016). However, to
achieve a fast recovery process requires continuous
exercise every day, and this is often hampered by
patient compliance. Then another alternative therapy
is needed that can help speed up the recovery
process of motor function of the upper limb. In
recent years, many studies of visual imagery
techniques in improving motor function after stroke.
This technique is done by giving suggestions to the
patient in a state of relaxation (Jones, 2014), and
imagining the paresis limb to perform certain
functional movements (Park et al., 2015). This
technique is the most likely to be done routinely
because without being affected by the motor strength
of stroke patients. Aaron J. Manganiello in 2011
conducted a case study of visual imagery technique
of a 57-year-old man with right hemiplegia. The
result, within 5 weeks, there was an improvement in
the function of the subjects, so that they were able to
walk and move using the right extremities. Liu's
RCT study, published in the 2009 Hongkong Med
Journal, involved 17 subjects with visual imagery
interventions, finding improved sensorimotor
function in post-stroke patients compared with the
conventional rehabilitation group, as measured by
the Fugl-Meyer Assessment of Sensorymotor
Recovery After Stroke. Holroyd et al from the
University of California’s Neurophysciatric Division
gave suggestions to 66-year-old women with
Goutama, E. and Setiono, S.
Effects of Visual Imagery Techniques on Improving Motor Function of Upper Limb in Chronic Ischemic Stroke Patients: A Serial Case Repor t.
DOI: 10.5220/0009090303310336
In Proceedings of the 11th National Congress and the 18th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation Association (KONAS XI and PIT XVIII PERDOSRI
2019), pages 331-336
ISBN: 978-989-758-409-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
331

complete paralysis of the left arm due to carotid
artery blockage. Obtained after 5 times of imagery
interventions to do daily activities that are popular,
there is a movement of the left arm that is much
better than before therapy, and subjects are able to
do daily activities even without help (Liu, 2009).
The main objective of this study is to report our
success in improving the motor function of the
paresis hand of chronic stroke patients using visual
imagery techniques This study also explains how
visual imagery can stimulate neuroplasticity in the
brain and its clinical effect on the functioning of the
paresis hand side.
2 METHOD
This study is a case series study of 3 people with
chronic ischemic stroke, with weakness of the right
arm and hand. Intervention of visual imagery
techniques is given 2 times a week for 3 weeks to
each subject, without stopping the occupational
therapy that is being undertaken by the subject. The
procedure of visual imagery is to relaxing the
subject using direct suggestion, and guiding the
patient to recall activities that can be carried out with
the paresis side of the upper limb before the subject
suffers from a stroke. The output is an assessment of
hand function using the DASH questionnaire before
and after the intervention.
3 CASE PRESENTATION
3.1 Case 1
Right-handed 50-year-old male, with long-standing
infarction in internal capsule, thalamus and right
putamen, right hemiparesis, motor strength score
with Manual Muscle Testing (MMT) is 4, getting
occupational therapy 2 times a week, and additional
visual imagery therapy 6 sessions. Significant
improvements were found in the activities of holding
the steering wheel of a motorcycle and car, carrying
shopping bags, and washing hair, with a score before
getting intervention was 5, and after getting
intervention was 2 (where the lower the score
showed more improvement). Other activities such as
sweeping the floor and holding a knife also
improved with a score before the intervention was 4,
and the score after the intervention was 2.
Weaknesses in the arms, shoulders, or hands also
experienced significant improvements. The subjects
also rated the subject's confidence in the function of
his arms, hands, or shoulders to increase.
3.2 Case 2
67-year-old, right-handed male with multiple
infarcts in the right subcortical lobe, right-left lateral
periventricle, right basal ganglia, and right-sided
pons, right hemiparesis, motor limb strength scores
over MMT 4, get therapeutic intervention by
technique 6 sessions of visual imagery, as additional
therapy. Subjects received occupational therapy
twice a week in the hospital. Significant
improvements occurred in the opening and closing
of the jar, opening the door handle, and holding the
steering wheel of the motorcycle, with a score of 5
before getting visual imagery intervention, and a
score of 1 after getting visual imagery intervention.
Other activities such as turning a door lock, putting
an object on a shelf, and cleaning your back also
improved, with a score of 5 before the intervention
and a score of 2 after getting the intervention.
Weakness of arms, shoulders, or hands also
experienced significant improvement. Subjects were
also more confident with the development of hand
functions experienced by the subjects during the
study.
3.3 Case 3
A 38-year-old, right-handed woman with right
periventricular frontal lobe infarction, left
hemiparesis, with an upper limb muscle strength
score of MMT 4, received 6-session therapeutic
intervention with visual imagery techniques, as
additional therapy. Subjects received occupational
therapy once a week. Qualitatively, there was a
significant increase in hand function in the activity
of carrying shopping bags, lifting heavy objects, and
wearing clothes, with a score before the intervention
was 4, and after the intervention was 1. Weakness in
the arms, shoulders, or hands did not experience
significant improvement. Subjects still felt
inadequate and lacked confidence in the function of
the arms, shoulders, or hands after the study.
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
332
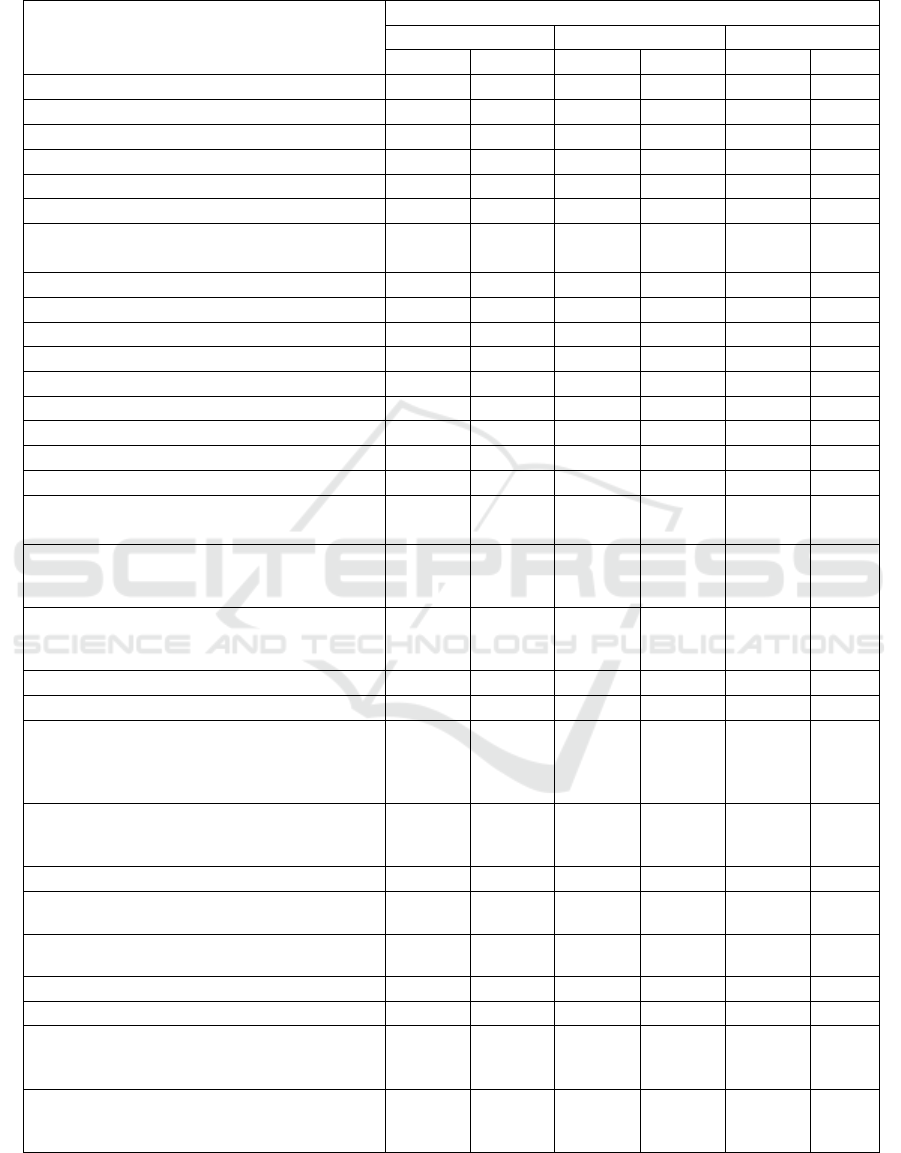
Table 1: DASH Questionnaire Score.
Score
Subject 1
Subject 2
Subject 3
Pre
Post
Pre
Post
Pre
Post
Open a tight or new jar
3
1
5
1
5
4
Write
5
5
4
3
1
1
Turn a key
4
3
4
1
4
3
Prepare a meal
-
-
-
-
2
2
Push open a heavy door
4
2
5
1
3
2
Place an object on a shelf above · your head
4
4
5
2
5
4
Do heavy household chores (eg · wash walls,
wash floors)
3
2
4
4
4
4
Garden or do yard work
4
2
2
2
4
3
Make a bed
2
2
2
2
2
2
Carry a shopping bag or briefcase
5
2
3
2
4
1
Carry a heavy object (over 10 lbs)
3
3
2
2
4
1
Change a lightbulb overhead
5
5
5
3
-
-
Wash or blow dry your hair
5
2
5
2
2
2
Wash your back
3
3
5
2
4
3
Put on a pullover sweater
3
2
4
2
4
1
Use a knife to cut food
4
2
4
2
-
-
Recreational activities which require little
effort (eg card playing, knitting, etc)
2
2
2
2
4
3
Recreational activities in which you take some
force or impact through your arm, shoulder or
hand (eg golf, hammering, tennis, etc)
-
-
-
-
5
5
Recreational activities in which you move
your arm freely (eg playing frisbee,
badminton, etc)
3
2
3
2
5
4
Hold the steering wheel of a motorcycle or car
5
2
5
1
4
2
Sexual activities
-
-
-
-
-
-
During the past week, to what extent has your
arm, shoulder or hand problem interfered with
your normal social activities with family,
friends, neighbours or groups
5
4
4
3
4
3
During the past week, were you limited in your
work or other regular · daily activities as a
result of your arm, shoulder or hand problem?
4
3
3
2
3
3
Arm, shoulder or hand pain
5
4
1
1
5
4
Arm, shoulder or hand pain when you
performed any specific activity
4
3
2
1
5
4
Tingling (pins and needles) in your · arm,
shoulder or hand
1
1
1
1
1
1
Weakness in your arm, shoulder or hand
4
2
3
1
4
3
Stiffness in your arm, shoulder or hand
4
3
3
2
3
3
During the past week, how much 29 difficulty
have you had sleeping · because of the pain in
your arm, shoulder or hand?
5
4
1
1
1
1
I feel less capable, less confident or 30. less
useful because of my arm, shoulder or hand
problem
4
1
4
1
4
3
Effects of Visual Imagery Techniques on Improving Motor Function of Upper Limb in Chronic Ischemic Stroke Patients: A Serial Case
Report
333

4 DISCUSSION
One of the goals of the rehabilitation program in
patients with chronic ischemic stroke is to restore
the function of limbs affected as optimal as possible.
The process of recovering neuronal damage after
ischemic stroke can occur spontaneously, and or
stimulated by rehabilitation interventions, to
stimulate brain neuroplasticity through the mediation
of Brain Derived Neurotrophic Factor (BDNF)
(Pascotini et al., 2018). Most BDNF is produced in
synapses in the hippocampus after ischemic-induced
brain injury, including stroke.(Lu et al., 2014) The
hippocampus is a center of learning and long-term
memory. By imagining and recalling memory
regarding certain activities with the side of the
paresis arm, the hippocampus will be activated to
recall that memory. Activation of the hippocampus
is thought to stimulate BDNF secretion which
triggers the process of neuroplasticity (Vertes, et al,
2001).
In addition, studies show that when a person
performs visual imagery, it appears that the
distribution of blood flow occurs in the occipital,
parietal, prefrontal, and anterior cingulate cortex
using Positron Emission Tomography (PET) (Jensen
et al., 2015). Activation of these areas turns out to be
the same as when a person gets sensory input and
performs certain motor movements significantly in
response to external stimuli. This shows that
performing visual imagery will have the effect of
increasing the firing rate of neurons in the same way
as doing real movements. Research by Ishai et al
found several studies of imagery that can evoke
response responses in the cortex that are visually
associated, namely occipitotemporal and
occipitoparietal (Ishai, Ungerleider and Haxby,
2000). Although there is no voluntary movement
that occurs during visual imagery, various studies
show that brain neuroplasticity occurs when visual
imagery is carried out, which is characterized by
improved function.
The post-stroke visual imagery technique is done
by giving the patient suggestions in a state of
relaxation, to imagine the body part that the paresis
is moving for a particular purpose. It has been
investigated that visual imagery when the brain is in
theta waves will increase firing and stimulate
neurons to make impulse pathways to the cortical
area, stored as memory, as if the imagery were
actually done and were happening at that time
(Faymonville, Boly and Laureys, 2006).
In this study, the three subjects were right-
handed, namely the dominance of the right hand to
carry out daily activities. Subjects 1 and 2 had right
hemiparesis, and were undergoing occupational
therapy 2 times a week. Whereas subject 3 was left
hemiparesis, and was undergoing occupational
therapy once a week. Improved hand function in
certain activities which is qualitatively significant is
seen to be more common in subjects 1 and 2 than in
subject 3. Similarly, weakness in the arms,
shoulders, or hands improved significantly in
subjects 1 and 2. These results are consistent with
Harris et al in a study concluded that functional
disorders that occur on the dominant side will be
lighter than if the affected side is non-dominant.3 In
addition, a randomized controlled trial (RCT) study
by Liu et al published in the Hong Kong Medical
Journal indicates that patients who received
additional visual imagery interventions for 3 weeks,
doing daily activities better than the group that only
received occupational therapy (Liu et al., 2004).
Likewise, a study by Park et al who divided the two
groups of subjects with stroke. Each group received
occupational therapy 20 minutes a day for five
sessions a week for two weeks. In the intervention
group visual therapy was added as many as five
sessions a week for two weeks. The results obtained
in the intervention group, there was an increase in
upper limb function and Activity Daily Living
(ADL) significantly compared to the control group
(Park et al., 2015).
In all three cases, there was an increase in the
motor function of the subject's hands on the paresis
side in certain activities, as measured by the DASH
questionnaire. Hand function activities that have
improved significantly are related to specific
activities that are carried out repetitively as subjects'
daily lives. Studies by Israely et al mention that
specific hand function exercises such as reaching,
grasping and object manipulation, which are carried
out 4-5 sets with each set of 8-15 reps, will improve
hand function as measured by the Fugl Meyer score
score (Israely, Leisman and Carmeli, 2017).
Literature review from Oujamaa et al showed that
exercise on the wrist and hand side of the paresis is
very important in all phases of the stroke
rehabilitation program. Recent neuroscience data
suggest that ipsilesional corticospinal stimulation
should be a priority. To get optimal functional
outcomes, stroke rehabilitation programs must be
based on specific activities and are repetitive
(Oujamaa et al., 2009).
In this study, psychologically it appears that
feelings of inadequacy, less useful, and lack of
confidence in the function of the arms, shoulders, or
hands of subjects 1 and 2 have improved. This is
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
334

because there is a significant increase in many
activities undertaken by subjects 1 and 2. While the
increase in activities that are still limited to subject 3
has not been able to increase the subject's
confidence. This is consistent with the study by
Dogu et al. That there is a relationship between
impaired hand function and psychological effects on
sufferers of brain injury, where a person's stress
level or depression will improve along with the
improvement in hand function experienced (Dogu et
al., 2014).
Visual imagery technique is an effective and safe
technique. No side effects were reported in this
study. A meta-analysis states that the visual imagery
technique is a safe therapy for various procedures.
Suggestions given by doctors to patients become an
important component in establishing doctor-patient
communication in daily clinical practice (Häuser et
al., 2016).
The limitation of this study is the absence of a
control group, so it cannot be concluded clearly
whether the intervention of visual imagery therapy
significantly improves hand function. In addition,
the occupational therapy that was undertaken by the
patient during the study was not standardized, so that
it could cause bias in the results of the study. Factors
such as a person's ability to imagine, residual
sensorimotor capabilities, ability to follow
commands, attention, and motivation may be crucial
components not considered in these patients (Butler
and Page, 2006). Further studies are needed with a
larger sample size, taking into account these aspects
to increase internal validity in research.
In conclusion, therapy with visual imagery
techniques can be considered an additional therapy
in patients with chronic ischemic stroke, because it
is proven to stimulate brain neuroplasticity, so as to
improve the function of the hands on the paresis
side.
REFERENCES
Butler, A. J. and Page, S. J. 2006 ‘Mental Practice With
Motor Imagery: Evidence for Motor Recovery and
Cortical Reorganization After Stroke’, Archives of
Physical Medicine and Rehabilitation, 87(12 SUPPL.),
pp. 2–11. doi: 10.1016/j.apmr.2006.08.326.
Dogu, B. et al. 2014 ‘The relationship between hand
function, depression, and the psychological impact of
trauma in patients with traumatic hand injury’,
International Journal of Rehabilitation
Research,37(2),pp.105-109.
doi:10.1097/MRR.0000000000000040.
Faymonville, M. E., Boly, M. and Laureys, S. 2006.
‘Functional neuroanatomy of the hypnotic state’,
Journal of Physiology Paris, 99(4–6), pp. 463–469.
doi: 10.1016/j.jphysparis.2006.03.018.
Filipe, J. 2011. Agents and Artificial Intelligence. Edited
by S. Bernadette. Springer.
Hatem, S. M. et al. 2016. ‘Rehabilitation of motor function
after stroke: A multiple systematic review focused on
techniques to stimulate upper extremity recovery’,
Frontiers in Human Neuroscience, 10(SEP2016), pp.
1–22. doi: 10.3389/fnhum.2016.00442.
Häuser, W. et al. 2016. ‘Wirksamkeit, Sicherheit und
Anwendungsmöglichkeiten medizinischer Hypnose:
Eine systematische Übersicht von Metaanalysen’,
Deutsches Arzteblatt International, 113(17), pp. 289–
296. doi: 10.3238/arztebl.2016.0289.
Ishai, A., Ungerleider, L. G. and Haxby, J. V. 2000.
‘Distributed neural systems for the generation of
visual images’, Neuron, 28(3), pp. 979–990. doi:
10.1016/S0896-6273(00)00168-9.
Israely, S., Leisman, G. and Carmeli, E. 2017.
‘Improvement in arm and hand function after a stroke
with task-oriented training’, BMJ Case Reports, 2017,
pp. 1–7. doi: 10.1136/bcr-2017-219250.
Jensen, M. P. et al. 2015. ‘Mechanisms of hypnosis:
Toward the development of a biopsychosocial model’,
International Journal of Clinical and Experimental
Hypnosis. Routledge, 63(1), pp. 34–75. doi:
10.1080/00207144.2014.961875.
Johnson, W., Onuma, O. and Sachdev, S. 2016. ‘Stroke : a
global response is needed. Bulletin of the World
Health Organization 94(9), 634-634A’. doi:
10.2471/blt.16.181636.
Jones, D. 2014. Advanced Ericksonian Hypnotherapy
Script. 2nd edn. Lulu Publishing.
Liu, K. P. et al. 2004. ‘Mental imagery for promoting
relearning for people after stroke: A randomized
controlled trial’, Archives of Physical Medicine and
Rehabilitation, 85(9), pp. 1403–1408. doi:
10.1016/j.apmr.2003.12.035.
Liu, K. P. Y. 2009. ‘Use of mental imagery to improve
task generalisation after a stroke’, Hong Kong Medical
Journal, 15(3 SUPP4), pp. 37–41.
Lu, J. et al. 2014. ‘Synthesis , Trafficking and Release of
BDNF’, pp. 1955–1971. doi: 10.1007/978-1-4614-
5836-4.
Oujamaa, L. et al. 2009. ‘Rehabilitation of arm function
after stroke. Literature review’, Annals of Physical and
Rehabilitation Medicine, 52(3), pp. 269–293. doi:
10.1016/j.rehab.2008.10.003.
Park, J. H. et al. 2015. ‘Effects of mental practice on
stroke patients’ upper extremity function and daily
activity performance’, Journal of Physical Therapy
Science, 27(4), pp. 1075–1077. doi:
10.1589/jpts.27.1075.
Pascotini, M. E. T. et al. 2018. ‘Brain-Derived
Neurotrophic Factor Levels are Lower in Chronic
Stroke Patients: A Relation with Manganese-
dependent Superoxide Dismutase ALA16VAL Single
Nucleotide Polymorphism through Tumor Necrosis
Effects of Visual Imagery Techniques on Improving Motor Function of Upper Limb in Chronic Ischemic Stroke Patients: A Serial Case
Report
335

Factor-α and Caspases Pathways’, Journal of Stroke
and Cerebrovascular Diseases. Elsevier Inc., 27(11),
pp.3020–3029.doi:
10.1016/j.jstrokecerebrovasdis.2018.06.032.
Venketasubramanian, N. et al. 2017. ‘Stroke
Epidemiology in South , East , and South-East Asia :
A Review’, 19(3), pp. 286–294.
Vertes, R. P., Albo, Z., & Di Prisco, G. V. 2001. ‘Theta-
rhythmically firing neurons in the anterior thalamus:
Implications for mnemonic functions of Papez’s
circuit.’, pp. 619–625. doi: 10.1016/s0306-
4522(01)00131-2.
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
336
