
Gait in Obese Patient
Tirza Z. Tamin
Department of Physical Medicine and Rehabilitation, Dr. Cipto Mangunkusumo General Hospital,
Faculty of Medicine, University of Indonesia, Jakarta, Indonesia
tirzaediva.tamin@gmail.com
Keywords: Gait, Obesity
Abstract: Obesity is a known risk factor for several diseases, and also negatively affects physical functioning,
especially walking ability and performance. Some walking abnormalities in gait could be down to foot
problems as increased pressure is placed on the tendons and muscles of the foot, in particular, the plantar
fasciitis. It is widely known that overpronation is a very common occurrence in the obese. Understanding
mechanisms that may affect the ability to walk in older individuals may help to identify the target for
prevention and rehabilitation.
1 INTRODUCTION
Obesity is a known risk factor for several diseases,
and also negatively affects physical functioning,
especially walking ability and performance. Studies
have shown that walking ability is an important
prerequisite for autonomy in activities of daily living
(Seung-uk et al, 2011). Understanding mechanisms
that may affect the ability to walk in older
individuals may help to identify the target for
prevention and rehabilitation. Interestingly, obesity
is one of the main risk factors for knee and hip OA
and recent data have shown that obesity is cross-
sectionally associated with low walking speed and
predicts the development of mobility disability
(International Diabetes Institute, 2000).
2 DISCUSSION
2.1 Obesity
The prevalence of Obesity in Indonesia according to
Riskesdas 2018 increases when compared to 2013,
male 15% to 20% and women 26% to 35% (Kadouh,
2016). Department of Medical Rehabilitation of
RSCM increase in the number of patient visits to
The Obesity Polyclinic from 2015-2016 (from
1174 to 2272) and 2017-2018 (from 2821to 3370).
The high prevalence increases the morbidity and
disability caused by obesity (Winter, 1989).
Obesity can be diagnosed by 2 easily methods,
body mass index and waist size. Body Mass Index
(BMI) is calculated by dividing body weight in
kilograms by height in square meters. BMI
correlates with the amount of body fat to the risk of
disease. World Health Organisation (WHO) says
that central obesity in Asian people can be count
from their waist size > 90 cm for men and > 80 cm
for women.
2.2 Gait
Normal Gait
Gait means the way a person walks. Abnormal
gait or gait abnormality occurs when the body
systems that control the way a person is unable to
walk in the usual way. There are 2 concepts of
normal gait:
Stride length: the distance between points
of contact of the same foot (also one gait cycle).
Step length: the distance between points of
contact of opposite feet (normal is 15-20 in)
Gait cycle has two phases:
• Stance phase: time in which limb is in
contact with the ground (60% of the gait cycle)
• Swing phase: time in which limb is in the
air (40 % of the gait cycle).
58
Tamin, T.
Gait in Obese Patient.
DOI: 10.5220/0009062300580061
In Proceedings of the 11th National Congress and the 18th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation Association (KONAS XI and PIT XVIII PERDOSRI
2019), pages 58-61
ISBN: 978-989-758-409-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
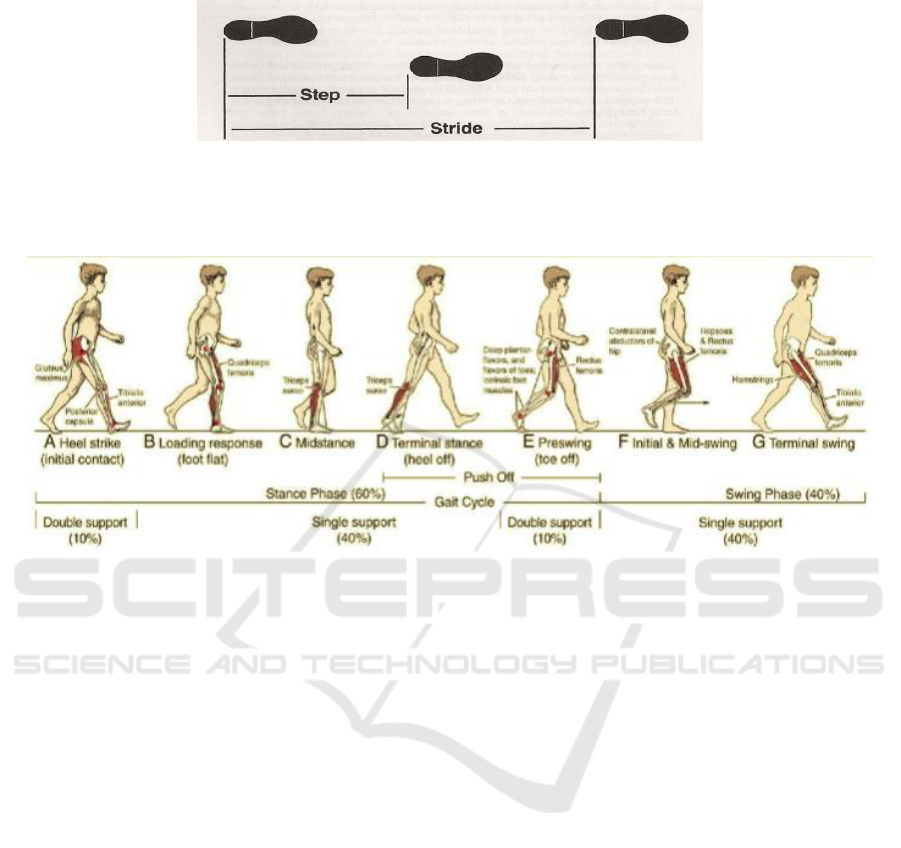
Figure 1: Normal Gait (Kadouh et al, 2016)
Figure 2: Types of Gait Cycle
Gait has its determinants that consist of how
anybody walks properly, there are
• Pelvic rotation
• Pelvic tilt
• Knee flexion in stance phase
• Foot mechanics
• Knee mechanics
• Lateral displacement of the pelvis
These factors help minimize the excursion of
COG to maximize forward progression with the least
expenditure of energy.
Abnormal gait
There are many causes of abnormal gait such as
focal weakness (example: dorsiflexion weakness),
joint contractures (example: tight heel cord), pain
(example: hip osteoarthritis), neurological conditions
(examples: stroke, Parkinson disease, CP).
Abnormal gait is categorized as one of five types
based on the symptoms or appearance of an
individual's walk. They are:
1. spastic gait
2. scissors gait
3. steppage gait
4. waddling gait
5. propulsive gait
Spastic gait
Spastic gait occurs when a person drags his or
her feet while walking. This type can also make
someone appear to be very stiff when walking.
Scissors gait
A person whose legs bend inward will often have
a scissors gait. With this type, a person's legs cross
and may hit each other while walking. The crisscross
motion may resemble scissors opening and closing.
Steppage gait
Steppage gait occurs when a person's toes point
towards the ground while walking. Often, the toes
will scrape against the ground as the person steps
forward.
Gait in Obese Patient
59

Waddling gait
As the name suggests, a person with a waddling
gait moves from side to side when walking.
Waddling involves taking short steps as well as
swinging the body.
Propulsive gait
Propulsive gait is when a person walks with his
or her head and neck pushed forward. It can appear
as though the person is rigidly holding a slouched
position.
In addition to these five types, a person with a
limp is also considered to have an abnormal gait.
Similarly, to other abnormalities, a limp may be
either temporary or permanent. A limp may also
clear up without medical intervention (Ferreira et al,
2013).
Measurement
There are about six quantitative measurements to
know is there any gait problems in an obese patient.
Direct Method
Normal gait movement, rotation, and procedures
can up to 5 times bodyweight at the ankles and 3
times at the knees (shear force). It’s using
intraarticular pressure equipment
is rarely used in
humans. In animal models can causes excessive
dynamic load-cartilage destruction and progressive.
Kinematic Analysis
Obtain hip, knee, and pelvic angles to move the
reflection mark on the joint with 4-6 cameras to
trajectory on the walking track. It is using the
internal axis and rotation angle to describes the 3D
movement of the joint during walking and includes
pelvic tilt and rotation angle, hip flexion, abduction
and adduction angles; knee flexion and abduction
angle; dorsiflexion of the ankle and angle of flexion
of the big toe; and scope of joint motion of the toe.
Weaknesses are complex and time-consuming and
difficult to use in clinical use.
EMG Dynamic
Effective for detecting muscle activity during
walking to analyzing and recording the time and
intensity of muscle activity. Superficial muscles use
surface electrodes, muscles in implanted wire
electrodes. It is important for a gait that is abnormal
with causes on nerves, and muscles. Weaknesses can
make the costs required are quite high and difficult
to accept widely.
Oxygen Consumption
Analyze energy consumption when walking to
using a portable oxygen analyzer. Gas released
during the walk to oxygen consumption analysis
related to mileage: the lower the oxygen cost to the
lower the energy consumption for walking.
Detecting oxygen consumption during walking with
prostheses, orthosis to the assessment of
rehabilitation efficiency.
Temporal-spatial Analysis
Temporal-spatial gait measurement with
footprint method (manual ink) pul computerized
(platform). Limitations do not record body and arm
movements. In the form of an electronic walk pad
inserted with baroreceptors to recording real-time
walking variables to measuring time-space variables
(single foot/feet support time, swing time and pace).
Use the comparison before treatment, determine
pathological pathology and see the effects of therapy
Its use is not much too expensive equipment prices.
Footprint
Implementation using the sole covered in ink and
runs through 4-6 m of cloth or white paper. Some
literature trajectories up to 10 m, with a starting
point of at least three steps before reaching the
platform to ensure a steady-state walking pattern.
The results were considered satisfactory for both
legs full contact with each white paper platform
(Ferreira, 2013).
3 CONCLUSION
Abnormalities in gait could be down to foot
problems as increased pressure is placed on the
tendons and muscles of the foot, in particular, the
plantar fasciitis. It is widely known that
overpronation is a very common occurrence in the
obese. In the study of walking pattern in obesity
with osteoarthritis knee has a result that obesity can
make changes in walking pattern, the step length is
become shorter and also minimize loading of the
knee joint. Increased BMI also has a major
KONAS XI and PIT XVIII PERDOSRI 2019 - The 11th National Congress and The 18th Annual Scientific Meeting of Indonesian Physical
Medicine and Rehabilitation Association
60

spatiotemporal modification, so it comes to shorter
step length, lower number of steps and lower
walking speed.
Loading in the musculoskeletal system of obese
patients can make a change in pathological walking
patterns, loss of mobility, and progression becoming
knee disability in osteoarthritis. Bodyweight also can
increase the joint load. Obese patients have an
increased external knee adduction movement
(EKAM) compared to patients with normal body
weight coupled with systemic factors from adipose
tissue and accelerate knee cartilage degeneration in
obese patients.
Quadriceps muscle weakness makes rapid
deceleration before heel strike and reduces high joint
loading adaptation to a walking pattern, so it
decreases ground reaction force and decreases
walking speed (Ferreira, 2013).
Bwop et al say in 55 obese patients with knee
osteoarthritis (OA), who run slower and have a
shorter stride length and higher EKAM than
normoweight with OA knee. So, the weight has a
role in EKAM. Changing the gait pattern can reduce
walking speed and decreases EKAM and smaller
foot length can reduce peak loading in the knee joint.
Harding et al. say that the relationship between
BMI with changes in walking patterns can make
changes in biomechanical patterns, so it decreased
walking speed and step length in obese subjects with
moderate knee OA compared to non-obese with
moderate OA (Butler, 2007).
Older adults with obesity show spatiotemporal
gait patterns which may help to reduce contact
impacts. Also, in obese persons, mechanical energy
usages tend to be lower in the anterior-posterior
plane and higher in the medial-lateral plane. Since
forward progression forces are mainly implicated in
normal walking, this pattern found in obese
participants is suggestive of lower energetic
efficiency (Stein, 2007).
REFERENCES
Seung-uk Ko, Sari Stenholm, and Luigi Ferrucci.
Characteristic Gait Patterns in Older Adults with
Obesity - Results from the Baltimore Longitudinal
Study of Aging. NIH-PA, 2011
International Diabetes Institute/ Western Pacific World
Health Organization/ International, Force A for the
study of OIOT. The Asia-Pacific perspective:
redefining obesity and its treatment. Geneva,
Switzerland: World Health Organization. 2000. p. 56.
Kadouh HC, Acosta A. Current paradigms in the etiology
of obesity. Tech Gastrointest Endosc [Internet].
2017;19(1):2–11. Available from:
http://dx.doi.org/10.1016/j.tgie.2016.12.001
Ferreira LAB, Neto HP, Grecco LAC, Christovao TCL,
Cuarte NAC, Lazzari RD, Galli M, Oliveira CS. Effect
of Ankle-foot Orthosis on Gait Velocity and Cadence
of Stroke Patients: A Systematic Review. J. Phys Ther
Sci. 2013 Nov; 25(11): 1503–8.
Butler PB, Farmer SE, Stewart C, et al. The effect of fixed
ankle-foot orthoses in children with cerebral palsy.
Disability & Rehabilitation. Assist Technol.
2007;2(1):51–58. DOI:10.1080/17483100 600662009.
Stein RB. Historical Overview of FES. Presented at 2007
Annual Meeting of the American Academy of
Orthotists & Prosthetists, San Francisco, CA.
Gait in Obese Patient
61
