
Validity of a Structure Sensor-based Anthropometric Measurement:
Performing a Pilot Study
Darko Katović
1
, Marjeta Mišigoj-Duraković
1
and Anita Bušić
2
1
Faculty of Kinesiology, University of Zagreb, Horvaćanski Zavoj 15, Zagreb, Croatia
2
Live Good d.o.o., Zagreb, Croatia
Keywords: Anthropometry, Kinanthropometry, Reliability, Validity, 3D Body Scaning, Structure Sensor.
Abstract: Development of new technologies is offering possibilities to overcome “traditional” limitations of
anthropometric measures and enable the production of a new generation of simple, high-speed, inexpensive,
highly defined and precise scanners for superficial body imaging. This study is an attempt to determine the
metric characteristic of the instrument (BodyRecog PRO) which technology is based on the method of deep
infrared 3D-scanning (Structure sensor). Reliability of the digitally obtained anthropometric measures was
tested in the process of relating them with the measures obtained via the traditional anthropometric
quantification.
1 INTRODUCTION
A contemporary level of technological development
makes it possible to construct instruments that are
portable and mobile enough to meet requirements of
versatile scientific branches in the field of data
acquisition.
In this paper, the focus is on the need to acquire
anthropometric measures. The intense development
of technology in a couple of the last decades has
gradually upgraded a “traditional” model of
anthropometric measures (length, width, skinfolds’
thickness, circumferences) with more complex
measures such as volumes and surface sizes of the
measured objects, by which changes in body size and
shape can, relatively inexpensively, be detected in
real time quite precisely, the goal hardly achievable
by the traditional measuring instruments (Rønnestad,
Hansen & Raastad, 2010; Schranz et al., 2010, 2012).
The application of the already well-known and
generally accepted techniques of digital body
measuring, founded upon the three dimensional (3D)
systems for superficial imaging, is limited due to their
high purchase costs, complex implementation and
constrained accessibility. However, the development
of new technologies (sensors and cameras of high
definition, data processing using machine learning
and artificial intelligence…) is offering posibilities to
overcome the mentioned limitations; it has enabled
the production of a new generation of simple, high-
speed, inexpensive, highly defined and precise
scanners for superficial body imaging (Simmons &
Istook, 2003; Zhang et al., 2014; Ryder & Ball, 2012;
Bragança et al.).
Different types of body scan sensing based
technologies can be found at the market. They differ
regarding ease of use, and quality of 3D models
reconstructed.
Applicable value of such technologically
saturated instruments depends on various factors that
have a direct influence on reliability and validity of
the process of measurement.
This paper investigates the utility of specific 3D
body scan technology in relation to classical
anthropometric approach.
2 METHODS
Besides the classical antropometric instruments, a
newly constructed measuring instrument assessing
girths of body segments – BodyRecog PRO has been
used in the research. The objective was to test metric
characteristics of the instrument founded upon the
method of a infrared depth-sensing 3D-scanning
technology. Therefore, reliability of the digitally
obtaine anthropometric measures was tested in the
process of relating them with the measures obtained
via the traditional anthropometric quantification, thus
also testing validity of the new instrument.
Katovi
´
c, D., Mišigoj-Durakovi
´
c, M. and Buši
´
c, A.
Validity of a Structure Sensor-based Anthropometric Measurement: Performing a Pilot Study.
DOI: 10.5220/0008506902450250
In Proceedings of the 7th International Conference on Sport Sciences Research and Technology Support (icSPORTS 2019), pages 245-250
ISBN: 978-989-758-383-4
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
245

2.1 Digital Mesurement Technology
The digital measurement was conducted by an iPad
Air 2 tablet with the iOS (ver. 10) operational system
and a 3D-scanner Structure Sensor - model: ST01
(Occipital, 2019) and with support of BodyRecog
PRO software (ver. 0.9.19).
Structure Sensor’s technical specification
includes the following technical elements important
for the study: Maximum recommended range
(3.5m+), minimum recommended range (40cm),
precision (0.5mm at 40cm, 30mm at 3m), field of
view (Horizontal: 58 degrees, Vertical: 45 degrees),
Resolution (VGA 640x480, QVGA 320x240).
Each of the above mentioned has a direct impact
on the result obtained.
2.2 Subjects
A convenience sample consisted of 71 participants of
both genders (men: n=52, age in years: mean±21,7;
SD±0,7; women: n=19; age in years: mean±20,9;
SD±0,4), students of the Faculty of Knesiology in
Zagreb. Participants were first manually measured –
by a set of standard anthropometric measurements of
circumferences, and then a digital measurement was
conducted using a newly constructed measuring
instrument BodyRecog PRO.
2.3 Variables
Entities were described by the sample of 34
variables
1
, out of which 18 were variables obtained by
the classical measurement of anthropometric
dimensions, whereas 16 variables were obtained by
the digital measurement of anthropometric
dimensions; the latter variables were defined by the
body sites and points that were either equivalent to
the ones of the traditional anthropometric
measurement (three measurement trials), or were
repositioned in an acceptable way.
A group of the traditional anthropometric
measures consisted of the following variables: body
height (BH), body mass (BM), waist circumference,
abdominal circumference, hip circumference, neck
circumference, breast circumference, chest cavity
circumference, left upperarm circumference, right
upperarm circumference, left forearm circumference,
right forearm circumference, left wrist circumference,
right wrist circumference, left thigh circumference,
1
Measurement units (classical and digital measurement):
BodyMass (kg), BodyHeight (cm), Girths (cm), Diameters
(cm).
right thigh circumference, left lowerleg (calf)
circumference, right lowerleg (calf) circumference.
A group of the digital anthropometric measures
consisted of the following variables
2
: D-BodyHeight,
D-NeckGirth, D-WaistGirth, D-AbdominalGirth, D-
HipsGirth, D-ChestGirth, D-BreastGirth, D-
RightUpperArmGirth, D-LeftUpperArmGirth, D-
RightForearmGirth, D-LeftForearmGirth, D-
RightWristGirth, D-LeftWristGirth, D-
RightWristDiameter, D-LeftWristDiameter, D-
RightUpperLegGirth, D-LeftUpperLegGirth, D-
RightLowerLegGirth, D-LeftLowerLegGirth.
2.4 Measurement Protocols
The traditional anthropometric measurement used the
standard procedure, conducted according the
International Biological Programme (IBP) and using
the standard measurement instruments but for a slight
modification – the examinee’s position was adjusted
to the position assumed in the digital scanning (the
feet hip-width apart and the extended arms raised
laterally at the shoulder height). Extremity
circumference measurements were executed on both
sides.
The digital anthropometric measurement
followed the traditional one. For the standardisation
purposes, the digital anthropometric measurement
protocol was designed. Here is a shortened version:
The space within which measurement scanning is
conducted must be at least 3 x 3 m with the central
marker for the participant. The examinee stands
quietly with the feet hip-width apart facing the
measurer. The arms are in side raise, paralell with the
floor, with the palms facing the floor. The
participant’s gaze is directed straight forward
throughout the measurement procedure. The
measurer, facing the participant 2-2.5 m apart
(distance in calibration phase) and holding the iPad
with the scanner perpendicular to the floor and at the
height corresponding to the participant’s abdomen,
positions the reference framework of the software
(guided by the software). Upon the software signal
saying that the action has been executed properly, the
measurer circles around the examinee 1 m apart
(distance in digital scaning phase); iPad must be
perpendicular to the floor all the time and at the half
of the participant’s height. The measurer stops
circling for a while after every circle quarter in order
to enhance body contours’ imaging. The measurement
2
Prefix “D” denotes a digital measurement.
K-BioS 2019 - Special Session on Kinesiology in Sport and Medicine: from Biomechanics to Sociodynamics
246
is over after three successfully registered/recorded
repetitions.
2.5 Statistical Analysis
Data were processed using the statistical package
StatisticaDell Inc. (Dell, 2017). The used procedures
included the computation of descriptive parameters
(mean, standard deviation, total range, variability
coefficient, distribution form parameters: skewness
and kurtosis). Reliability, based on the traditional
anthropometric measurement model, was assessed
using the method of internal consistency to establish
the following reliability coefficients: Cronbach and
Spearman-Brown’s (standardised) alpha. Pearson’s
correlation coefficient was applied to determine a
diagnostic validity of the newly constructed measuring
instrument (BodyRecog PRO).
3 RESULTS AND DISCUSSION
Descriptive parameters of both the traditionally and
digitally measured circumference variables were
computed for each of the convenience subsamples of
female and male students.
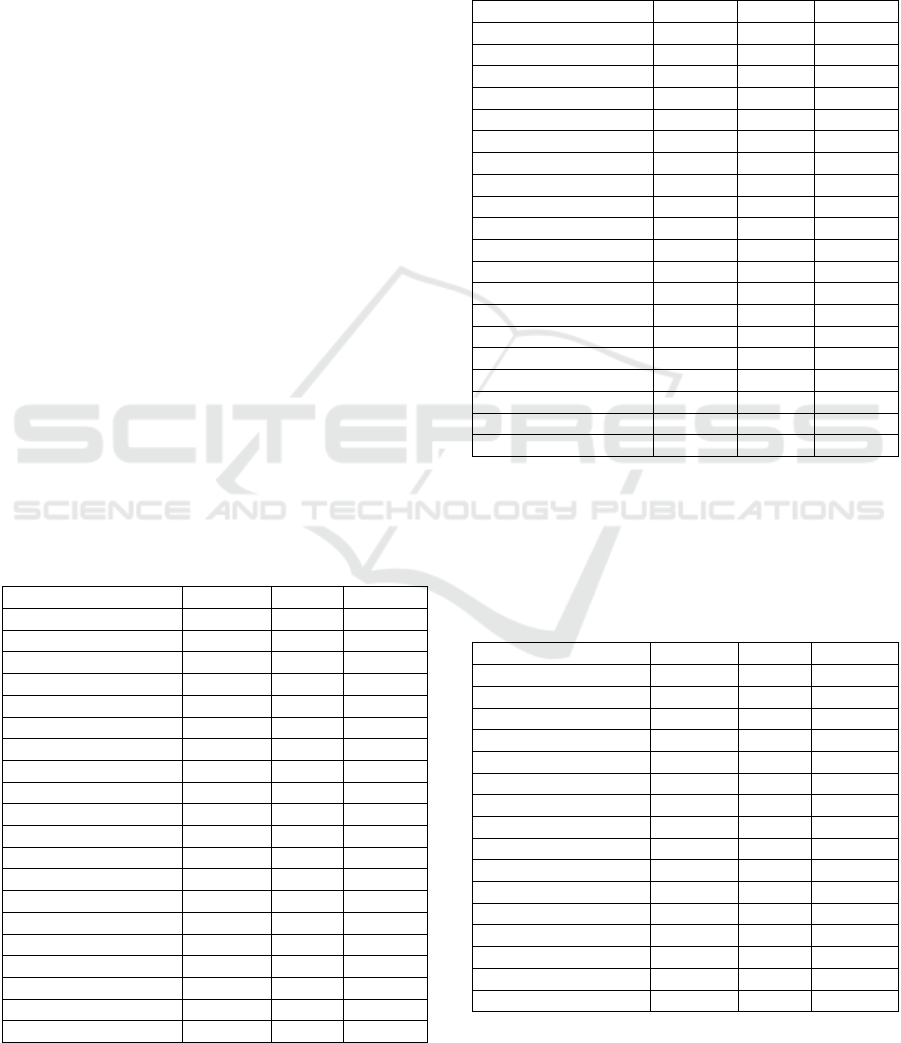
Basic descriptive parameters (central – arithmetic
mean, dispersive – range and standard deviation) of the
traditionally measured variables are presented in
Tables 1 and 2.
Table 1: Descriptive parameters (clasical measuremet) –
male students.
Variable name Mean Ran
g
e Std.Dev.
Bod
y
Mass 80,346 41,900 8,537
BodyHeight 183,138 34,200 7,455
NeckGirth 39,048 6,300 1,442
WaistGirth 79,950 17,600 4,081
AbdominalGirth 82,627 20,300 4,897
Hi
p
sGirth 100,921 20,400 4,471
ChestGirth 98,950 24,000 4,607
BreastGirth 95,867 23,400 4,308
RightUpperArmGirth 31,548 9,200 2,331
LeftU
pp
erArmGirth 31,244 10,600 2,431
Ri
g
htForearmGirth 28,469 8,000 1,440
LeftForearmGirth 28,062 7,300 1,479
RightWristGirth 17,677 3,800 0,765
LeftWristGirth 17,510 3,400 0,708
RightWristDiamete
r
5,946 1,400 0,298
LeftWristDiamete
r
5,871 1,100 0,255
Ri
g
htU
pp
erLe
g
Girth 57,085 15,200 3,152
LeftU
pp
erLe
g
Girth 56,692 16,100 3,189
RightLowerLegGirth 38,554 7,200 1,734
LeftLowerLegGirth 38,285 8,000 1,802
Values of the traditionally measured variables and
their parameters were in line with the values obtained
in the many same or similar previous measurements
conducted with the population of female and male
students of the Faculty of Kinesiology in Zagreb.
Table 2: Descriptive parameters (clasical measurement) –
female students.
Variable name Mean Ran
g
e Std.Dev.
Bod
y
Mass 62,000 28,300 6,929
BodyHeight 168,668 20,500 5,783
NeckGirth 32,837 5,900 1,408
WaistGirth 69,921 15,700 4,126
AbdominalGirth 77,363 15,700 5,032
Hi
p
sGirth 97,979 15,500 4,160
ChestGirth 86,174 16,200 3,583
BreastGirth 88,247 17,800 4,456
RightUpperArmGirth 27,132 7,000 1,778
LeftU
pp
erArmGirth 26,595 6,600 1,713
Ri
g
htForearmGirth 24,068 4,000 0,949
LeftForearmGirth 23,711 3,800 1,056
RightWristGirth 15,632 2,900 0,791
LeftWristGirth 15,532 3,000 0,799
Ri
g
htWristDiamete
r
5,253 1,000 0,284
LeftWristDiamete
r
5,121 1,200 0,288
Ri
g
htU
pp
erLe
g
Girth 54,226 12,400 3,269
LeftUpperLegGirth 53,847 12,200 3,363
RightLowerLegGirth 35,668 7,200 1,991
LeftLowerLegGirth 35,595 7,300 1,902
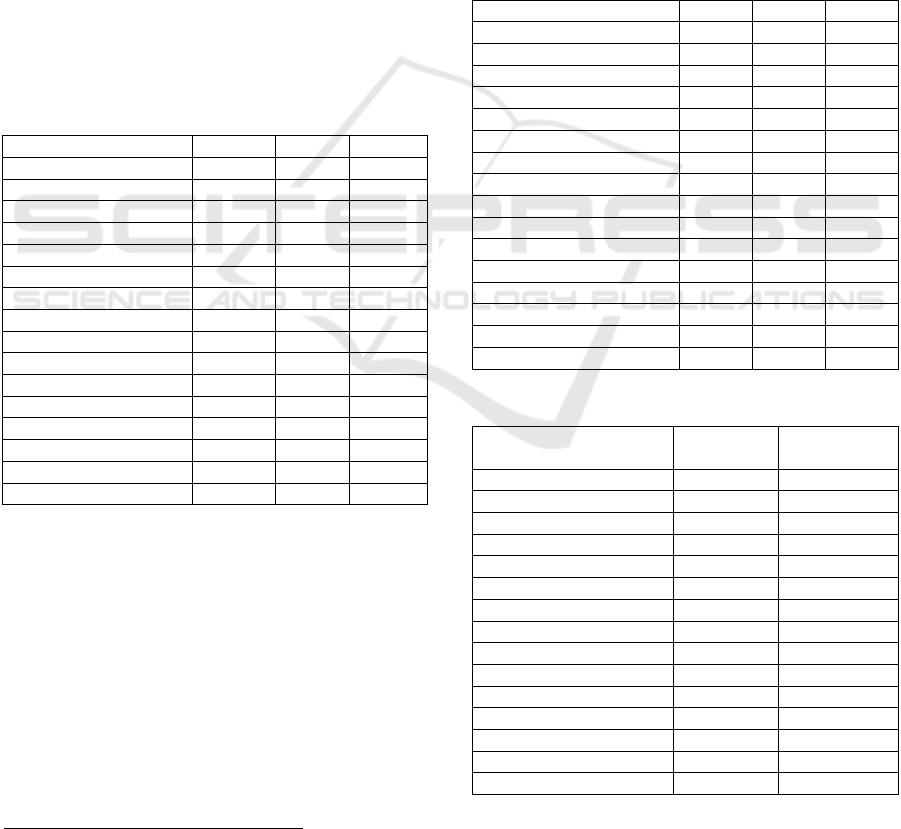
Tables 3 and 4 show basic descriptive parameters
(central – arithmetic mean, dispersive – range and
standard deviation) of the variables mesured digitally
by the BodyRecog PRO instrument.
Table 3: Descriptive parameters (digital measurement) –
male students.
Mean Range Std.Dev.
D-Bod
y
Mass 80,177 41,900 8,613
D-Bod
y
Hei
g
ht 184,570 36,107 7,646
D-AbdominalGirth 84,736 21,993 5,255
D-HipsGirth 101,436 22,833 4,766
D-ChestGirth 104,205 27,230 4,920
D-BreastGirth 97,753 23,763 4,577
D-Ri
g
htU
pp
erArmG 33,221 10,673 2,536
D-LeftU
pp
erArmG 32,673 10,397 2,617
D-Ri
g
htForearmG 30,525 15,037 2,737
D-LeftForearmG 31,118 33,343 6,276
D-RightWristGirth 19,789 11,057 2,207
D-LeftWristGirth 20,977 15,980 3,939
D-Ri
g
htU
pp
erLe
g
G 54,709 31,893 5,496
D-LeftU
pp
erLe
g
G 54,817 35,467 6,058
D-RightLowerLegG 37,770 19,913 2,982
D-LeftLowerLegG 37,226 20,037 3,043
Validity of a Structure Sensor-based Anthropometric Measurement: Performing a Pilot Study
247
We should emphasise here that the descriptive
parameters of the marked variables of the subsamples
of men and women (Tables 3 and 4) were computed
from the data saturated with the perceived and
recorded measurement errors. Unsuccessful scans
were reported primarily due to body movement -
examinee was not able to stand upright absolutely
still, low iPad battery or other types of software
issues.
The proportional contribution of the so
contaminated data to particular variables (no gender
differentiation) was the following: D-
RightForearmGirth (9.38%), D-LeftForearmGirth
(11.73%), D-RightWristGirth (13.14%), D-
LeftWristGirth (18.77%), D-RightUpperLegGirth
(3.28%), D-LeftUpperLegGirth (3.28%), D-
RightLowerLegGirth (10.79%), D-
LeftLowerLegGirth (10.79%). Although the research
was a pilot-project, the analysis results should be
observed with additional caution.
Table 4: Descriptive parameters (digital measurement) –
female students.
Mean Range Std.D.
D-BodyMass 61,953 28,300 7,267
D-BodyHeight 169,753 20,810 6,031
D-AbdominalGirth 81,307 18,793 4,951
D-Hi
p
sGirth 99,353 16,743 4,956
D-ChestGirth 90,936 19,363 4,660
D-BreastGirth 90,528 18,883 4,969
D-RightUpperArmG 30,266 8,520 1,905
D-LeftUpperArmG 30,229 8,353 2,016
D-Ri
g
htForearmG 26,233 10,493 2,576
D-LeftForearmGirth 26,148 7,310 1,757
D-RightWristGirth 17,490 7,800 2,257
D-LeftWristGirth 18,262 8,373 2,280
D-RightUpperLegG 51,769 26,203 5,687
D-LeftU
pp
erLe
g
G 50,674 12,933 4,148
D-Ri
g
htLowerLe
g
G 39,829 16,203 4,359
D-LeftLowerLe
g
Girth 40,250 13,093 3,747
Deviation magnitudes
3
of the corresponding
variables (the ones with the matching measuring
points) in the group of the traditional and the digital
measurement are significantly different (Table 5).
The biggest deviation (in the form of average
increase in the results) was observed in the variable
delta-ChestGirth, followed by the variables of the
upper segments of the arms.
Only the circumferences of both the left and the
right thigh demonstrated a tendency of a significant
decrease in the results when compared with the
reference, traditional, measurement.
3
Prefix “delta” denotes a deviation magnitude.
It is interesting to notice that the first six variables,
whose measurement points are within the centrally
positioned reference framework of the instrument
(including the height of the instrument relative to the
measurement object), delta-BodyHeight, delta-
AbdominalGirth, delta-HipsGirth, delta-ChestGirth,
delta-BreastGirth, delta-RightUpperArmGirth, delta-
LeftUpperArmGirth, follow most proportinally
average deviations (with the increase in the results)
and adequate dispersion.
A higher dispersion of the
results was emphasised in every variable of the digital
circumference measurement positioned distally from
the body trunk and upper segments of the upper
extremities. The mentioned can also be followed via
the standard deviation magnitudes (Table 5).
Table 5: Deviation magnitudes.
Variable name Mean Ran
g
e Std.D.
delta
_
Bod
y
Mass -0,137 10,700 1,076
delta_BodyHeight 1,339 8,090 1,225
delta_AbdominalGirth 2,600 18,543 2,826
delta_HipsGirth 0,745 9,663 1,996
delta
_
ChestGirth 5,123 16,817 2,406
delta
_
BreastGirth 1,991 10,990 1,760
delta_RightUpperArmG. 2,064 4,910 1,142
delta_LeftUpperArmG. 2,019 7,120 1,479
delta_RightForearmG. 2,085 12,517 2,132
delta
_
LeftForearmGirth 2,891 28,920 4,892
delta
_
Ri
g
htWristGirth 2,044 9,607 2,097
delta
_
LeftWristGirth 3,270 14,837 3,332
delta_RightUpperLegG. -2,397 30,030 4,568
delta_LeftUpperLegG. -2,223 28,523 4,372
delta_RightLowerLegG. 0,540 19,173 3,649
delta
_
LeftLowerLe
g
G. 0,471 18,530 3,699
Table 6: Reliability measures.
Variable name
Crombach
al
p
ha
Standardized
al
p
ha
D-Bod
y
Hei
g
ht 0,989 0,990
D-AbdominalGirth 0,952 0,952
D-HipsGirth 0,897 0,898
D-ChestGirth 0,968 0,969
D-BreastGirth 0,987 0,988
D-Ri
g
htU
pp
erArmG. 0,969 0,970
D-LeftU
pp
erArmGirth 0,897 0,908
D-Ri
g
htForearmGirth 0,739 0,748
D-LeftForearmGirth 0,828 0,869
D-RightWristGirth 0,575 0,579
D-LeftWristGirth 0,672 0,696
D-Ri
g
htU
pp
erLe
g
Girth 0,604 0,717
D-LeftU
pp
erLe
g
Girth 0,621 0,721
D-RightLowerLegG. 0,454 0,523
D-LeftLowerLegGirth 0,539 0,574
K-BioS 2019 - Special Session on Kinesiology in Sport and Medicine: from Biomechanics to Sociodynamics
248

Reliability of the anthropometric measurement
using the digital instrument was expressed by the
method of internal consistency among the
measurement items; Cronbach’s and standardised
alpha were computed.
Reliability measures (Table 6) indicated an
acceptable reliability of the following digital girth
measures (variables): Body Height, AbdominalGirth,
HipsGirth, ChestGirth, BreastGirth,
RightUpperArmGirth, LeftUpperArmGirth. As
regards the other digital measures, a considerable
further work is needed.
The magnitudes of average correlation among the
items of digital measurement (which could also be
recognised as a homogeinity measure) expectedly
follow reliability decrements in case of the distal
measurement points.
Correlation coefficient magnitudes (Table 7)
indicate the correlation power of the corresponding
variables.
Table 7: Correlation magnitudes.
Classic
r
Di
g
ital
Bod
y
Mass 0,996
*
D-Bod
y
Mass
Bod
y
Hei
g
ht 0,992
*
D-Bod
y
Hei
g
ht
AbdominalGirth 0,863
*
D-AbdominalGirth
HipsGirth 0,912
*
D-HipsGirth
ChestGirth 0,949
*
D-ChestGirth
BreastGirth 0,951
*
D-BreastGirth
Ri
g
htU
pp
erArmG 0,922
*
D-Ri
g
htU
pp
erArmGirt
LeftU
pp
erArmG. 0,875
*
D-LeftU
pp
erArmGirth
RightForearmG. 0,763
*
D-RightForearmGirth
LeftForearmG. 0,578
*
D-LeftForearmGirth
Ri
g
htWristGirth 0,506
*
D-Ri
g
htWristGirth
LeftWristGirth 0,502
*
D-LeftWristGirth
Ri
g
htU
pp
erLe
g
G 0,591
*
D-Ri
g
htU
pp
erLe
g
Girth
LeftUpperLegG. 0,674
*
D-LeftUpperLegGirth
RightLowerLegG 0,244
*
D-RightLowerLegGirth
LeftLowerLegG. 0,212 D-LeftLowerLegGirth
The Pearson's correlation coefficient was used as
a measure of validity. Marked correlations (*) are
significant at p<0,05. An gradation of correlation
coefficients magnitudes (both in size and colour –
from cool colours to warm ones) clearly illustrates
association between the traditional measures and the
corresponding digital measures corroborating poorer
validity of distal measures in the comparison to the
central ones.
4 CONCLUSIONS
The analysed measurement instrument has not yet
met the targeted reliability level at all the measured
points (apart from, relatively, D-BodyHeight, D-
AbdominalGirt, D-ChestGirth, D-BreastGirth, D-
Hips Girth, D-RightUpperArmGirth and D-
LeftUpperArmGirth).
The obvious decrements in reliability of the
measures taken digitally distally from the body trunk
measures and upper segments of the upper extremities
indicate possible association with the technical
characteristics of the measuring instrument as well as
with the camera position management in relation to
the measurement object (the measures gathered at the
level of the central body trunk girth measures, with
no camera angle correction in relation to the measures
collected using the scanning angles corrections
towards the distal body segments while relatively
preserving the scanning height).
A needed additional partial analysis of varying
influences of measurement conditions and
techniques, as well as the analysis of their combined
influence on the measured results together with
additional software improvements will contribute to
the targeted measuring instrument’s utility.
The observed analytical limitations of the study
are closely related to the type of study conducted
(pilot study), therefore additional differences analysis
and standardized comparison methods will be made
after satisfactory hardware and software
modifications of the measuring instrument.
ACKNOWLEDGEMENTS
The research was conducted by the Joint Research
Group of Laboratory for Sports Medicine & Exercise
– Kinanthropometry and Biomechanics Laboratory of
the Institute of Kinesiology, Faculty of Kinesiology,
and companies Live Good d.o.o. Authors declare no
conflict of interest.
REFERENCES
Bragança, S., Carvalho, M., Xu, B.; Arezes, P., Ashdown,
S. A., 2014. Validation Study of a Kinect Based Body
Imaging (KBI) Device System Based on ISO
20685:2010. Conference. Lugano, 5th International
Conference on 3D Body Scanning Technologies.
Dell Statistica (data analysis software system), version 12.
software.dell.com.
Occipital, 2019. Technical Specification. Accessed May 15,
2019. https://support.structure.io/article/157-what-are-
the-structure-sensors-technical-specification
Rønnestad, B. R., Hansen, E. A., Raastad, T., 2010. Effect
of heavy strength training on thigh muscle cross-
sectional area, performance determi- nants, and
Validity of a Structure Sensor-based Anthropometric Measurement: Performing a Pilot Study
249

performance in well-trained cyclists. European Journal
of Applied Physiology, 108, 965–975.
doi:10.1007/s00421-009-1307-z
Ryder, J. R., Ball, S. D., 2012. Three-dimensional body
scanning as a novel technique for body composition
assessment: A preliminary investigation. J. Exerc.
Physiol. Online, 15(1):1-14.
Schranz, N. et al., 2010. ‘Three-dimensional
anthropometric analysis: Differences between elite
Australian rowers and the general population’, Journal
of Sports Sciences, 28(5), pp. 459–469. doi:
10.1080/02640411003663284.
Schranz, N. et al., 2012. ‘Is three-dimensional
anthropometric analysis as good as traditional
anthropometric analysis in predicting junior rowing
performance?’, Journal of Sports Sciences, 30(12), pp.
1241–1248. doi: 10.1080/02640414.2012.696204.
Simmons, K. P., Istook, C. L., 2003. Body measurement
techniques: A comparison of three-dimensional body
scanning and physical anthropometric methods for
apparel application. J. Fash. Mark. Manag., 7(3):306-
32.
Zhang, K.. Zheng, J., Gao, C., Thomas, D., Li, X.,
Heymsfield, S., 2014. Rapid-accurate anthropometric
body shape assessment with low- cost novel 3D
imaging system. F. A. S. E. B. J., 28(Suppl. 1):391.2, 2.
K-BioS 2019 - Special Session on Kinesiology in Sport and Medicine: from Biomechanics to Sociodynamics
250
