
Testbed Requirements for Technology Enhanced Stroke
Rehabilitation to Support Independent Living
Awais Ahmad, Peter Mozelius and Karin Ahlin
Department of Computer and System Science, Mid Sweden University, Östersund, Sweden
Keywords: E-Health, Stroke Rehabilitation, Independent Living, Ageing Well, Testbed Requirements.
Abstract: An identified global phenomenon is that, as the percentage of older adults increases, new challenges arise for
medical care and rehabilitation. Several research studies have presented e-health as a promising concept to
support the idea of independent living among patients with chronic diseases. The Mid Sweden region has a
relatively old population and is a region where people live with long distances to the nearest hospital or health
care centres. This study had a focus on defining testbed requirements for a technology enhanced stroke
rehabilitation adapted to the specific region. The focal research question to answer in this study was: What
are the requirements and their associated benefits and barriers of using technology-enhanced systems instead
of traditional techniques for stroke rehabilitation in the Mid Sweden region? With Design Science as the
overall research strategy, data was collected by semi-structured interviews with key stakeholders in the field
of stroke rehabilitation. A deductive thematic analysis was conducted where important themes were grouped
into the four main requirement categories of: Technical, Human-computer-interaction, Clinic and
Sustainability. Beside the more specific requirements, an interesting finding was the division of stroke
rehabilitation into the categories motoric, cognitive and speech rehabilitation; also, how technology enhanced
solutions might be used in these categories. Each category has a potential for a successful use of technology
enhanced services, but as the standard procedure in traditional stroke rehabilitation each patient needs a
personalised treatment.
1 INTRODUCTION
Because the population of older adults is increasing
significantly all over the world, leading to current
and future demographic changes, the world is facing
substantial challenges (Chaaraoui and Florez-
Revuelta, 2016). According to United Nations’ global
ageing indicators, number of people aged more than
60 years was 801 million in 2015 which will become
1.4 billion in 2030 and mover over in 2050, it will
increase to 2.1 billion which means that 20% of the
total papulation will be 60 years or older.
Consequently, the number of people requiring long-
term medical care will also be increased and more
medical and social services will be needed that are
designed to support chronic diseases (Ehn et al., 2015,
Chaaraoui and Florez-Revuelta, 2016). Traditional
rehabilitation systems require a large number of
clinical staff and they are difficult to deploy because
of high running costs (Zhang et al., 2016).
In the last two decades, Technology Enhanced
Systems (TES) has emerged as potential tools for
many treatments in therapy and rehabilitation. Those
technologies are not only cost effective, they are
helpful to develop more usable, useful, and accessible
e-health services that can be helpful for physical,
cognitive and psychological rehabilitation (Zhang et
al., 2016, Rizzo and Kim, 2005, Broeren et al., 2008).
Some other theoretical findings show that there are
some critical requirements, which need to be
addressed in order to adopt those e-health
technologies such as trust, personal integrity,
technology acceptance, e-health literacy and
accessibility of ICT (Fischer et al., 2014, Ahmad and
Mozelius, in press). These findings therefore need to
be meet with requirements from the user perspective.
Thusly, this study had a focus to understand the
requirements of technology enhanced systems (TES)
for independent living and to determine the
challenges for deployment of TES.
Stroke is one of the biggest causes of death around the
world and a main reason of chronic disabilities in
adults (Yamato et al., 2016). It is considered a
primary cause of permanent physical damage in the
174
Ahmad, A., Mozelius, P. and Ahlin, K.
Testbed Requirements for Technology Enhanced Stroke Rehabilitation to Support Independent Living.
DOI: 10.5220/0007658101740182
In Proceedings of the 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2019), pages 174-182
ISBN: 978-989-758-368-1
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

adult population and, due to those physical
disabilities, the affected people fail to continue a
healthy social life and they must compromise the pure
joy of life; the older adults are the most affected age
group (Broeren et al., 2008).
Although the challenges for stroke rehabilitations
are common all over the world, our main focus was
the Mid Sweden region. According to “Statistics
Sweden”, the population of the Mid Sweden Region
is scattered in the whole region and a large number of
people are living outside the cities (SCB, 2016).
Consequently, providing rehabilitation services in the
remote areas is even more challenging and a large
amount of resources are needed to meet these
challenges. Technology enhanced systems can play a
vital role there.
1.1 Aim
The aim of the study was to define the testbed
requirements for a technology enhanced stroke
rehabilitation to support independent and active
living. The main research question was: What are the
requirements, benefits and barriers of using
technology enhanced systems instead of traditional
techniques for stroke rehabilitation in the Mid
Sweden region?
2 EXTENDED BACKGROUND
2.1 Stroke Rehabilitation
After stroke, rehabilitation has been challenging for
both patients and healthcare providers, as it requires
high motivation and hard work from patients and
extensive resources from health care providers
(Yamato et al., 2016, Broeren et al., 2008). Most
commonly, a stroke patient may suffer from some
serious motor, cognitive and speech impairments
(Langhorne et al., 2011). Various treatments are
available for stroke rehabilitation that involves
physical therapy, cognitive recovery and speech
restoration with language therapy (Seniów et al.,
2009, Langhorne et al., 2011, Veerbeek et al., 2014,
Pollock et al., 2014).
Stroke patients experience motor impairments in
the left or right side of the body that can limit their
physical activity and consequently the patient’s
ability to perform their daily routine tasks decreases
immensely (Langhorne et al., 2009, Palmcrantz et al.,
2017). In order to overcome the aftereffects of stroke,
and to increase the quality of patient's life, intense and
long-term physical training is needed and should be
started as early as possible (Ehn et al., 2015). Many
of the currently used treatments for motor injuries
involve physiotherapy and guided physical exercises;
the perceived benefits of using physical therapy in
stroke rehabilitation are continually increasing
(Veerbeek et al., 2014). In the last two decades,
several technology-enhanced rehabilitation systems
for stroke have been suggested in different studies
with their own benefits, drawbacks and limitations
(Rizzo and Kim, 2005, Broeren et al., 2008,
Palmcrantz et al., 2017). A number of novel therapies
has been developed and tested and, in few of them,
virtual reality and robotics are also involved.
Although the perceived benefits of these
interventions are not well known yet, there are strong
possibilities of progress in these types of therapies
(Langhorne et al., 2009).
2.2 Independent Living and Ageing
Well
Considering the rapid increase of older population,
several research studies have highlighted the
importance of designing new e-health services to
support the ideas of independent living and ageing
well (Bowes and McColgan, 2013, Christophorou et
al., 2016). Recent research studies have found that
most older adults prefer to age in place, and that this
concept is favored by policy makers (Peek et al.,
2016), but also that contextual and psychosocial
factors must be carefully explored if e-health services
should result in a beneficial impact (Bowes and
McColgan, 2013, Axelsson and Wikman, 2016).
The concepts of ageing well and older adults’
possibilities for independent living are related and
intertwined (Billis et al., 2015). Ageing well, or
healthy ageing, has been described as a lifelong
process to optimise the opportunities for improving
and preserving health and physical, social and mental
wellness to obtain independence and quality of life
(Peel et al., 2004). Stroke is one of several acute
health conditions that often results in lost
independence, and a main objective in the
rehabilitation must be to reestablish and facilitate
patients’ independent living to obtain their quality of
life (Gwozdz and Sousa-Poza, 2010).
3 METHOD
The overall research strategy for the study was a
Design Science approach inspired by the fivefold
Testbed Requirements for Technology Enhanced Stroke Rehabilitation to Support Independent Living
175
process outlined by Johannesson and Perjons (2014).
In the general definition, Design Science should
involve a rigorous process where the design of
artefacts should try to solve observed problems and
make research contributions (Hevner et al., 2004,
Peffers et al., 2007; Johannesson and Perjons, 2014).
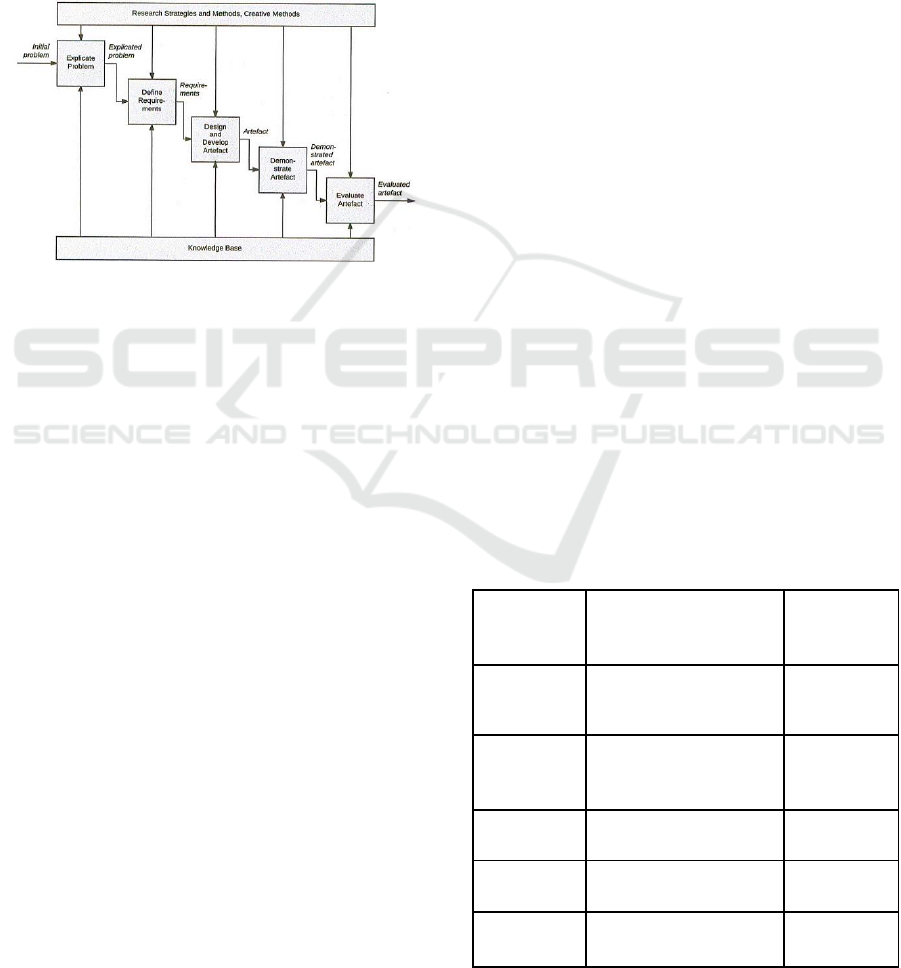
This study was carried out for the first two phases of
the process that is illustrated below in Figure 1.
Firstly, a problem was identified and formulated, and
in the second phase the testbed design requirements
were defined.
Figure 1: Phases in the Design science process.
Many design science studies do not carry out all the
five phases of the method framework depicted in
Figure 1. This study was conducted as a Requirement-
Focused Design Science project, with a focus on
defining requirements. This type of study starts with
an existing problem and defines requirements in a
combination of a literature study and interaction with
relevant key stakeholders. In Requirement-Focused
Design Science Research, the artefact design is only
outlined and involves neither artefact demonstration,
nor artefact evaluation. (Johannesson and Perjons,
2014).
Defined requirements will be the foundation for
future work, where the remaining phases in Figure 1.
will be carried out. Defined testbed requirements
were divided into the categories of 1) Technical
requirements, 2) HCI requirements, 3) Clinic
requirements, and 4) Sustainability requirements, as
the four fundamental pillars for a successful
implementation of a testbed for stroke rehabilitation
to support independent living.
3.1 Data Collection
Some type of interviews may be the most common
data collection method for defining requirements. A
direct approach to requirement specification is to
interview different stakeholders about which explicit
requirements they would suggest. Interviews can be
highly efficient, but they also risk stifling creativity if
they are too structured. Best practice is often to use
semi-structured or unstructured interviews to
encourage informant initiatives. It is also of
importance to select informants with a competency
and engagement that add value to the requirement
specification process (Johannesson and Perjons,
2014).
Data for defining the requirements in this study
were gathered in a combination of semi-structured
interviews and by a literature study. All interviews
were carried out following a common instrument,
with a basic question schedule that allowed
adaptation to the various interviewees. The basic
question schedule included themes such as work
relation to stroke rehabilitation, current knowledge,
use, and understanding of use of ICT and its
usefulness in relation to stroke rehabilitation, future
wishes for use of ICT in relation to stroke
rehabilitation, and budget for using ICT in relation to
stroke rehabilitation. Keywords for searching
literature were: e-health, stroke rehabilitation,
independent living, and ageing well. Interviews were
also combined with taking handwritten notes, to
provide a backup to the audio recording, but also to
facilitate the analysis process. The analysis process
has been reflexive for the researchers, looking at the
novelty of the requirement area, stroke rehabilitation
(Thomsson, 2002). The impact has been further
knowledge building and reflection following each
interview session and further reading to understand
the area.
Table 1: Informants’ professional roles and years of
experience of Stroke rehabilitation.
Informant
Professional role
Years of
experience
Informant 1
Speech therapist
25
Informant 2
The region’s medically
responsible doctor
25
Informant 3
Therapist #1
5
Informant 4
Physiotherapist #1
18
Informant 5
Physiotherapist #2
3
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
176

Data were collected from five informants with
different roles in contemporary stroke rehabilitation.
This was a purposive sampling where all informants
have special expertise and deep knowledge in the
investigated area. Purposive sampling is a sampling
technique where researchers rely on their own
judgment when choosing informants to participate in
ta study. Chosen informants’ roles and their years of
experience are described below in Table 1.
Informants 3 - 5 work as part of a mobile team for
stroke rehabilitation located at the region’s hospital.
The mobile team includes one manager and four co-
workers, adding one more therapist. The mobile team
is responsible for rehabilitation after clinical care as
the patients have been relocated to their homes. The
mobile team offers care for patients living 70 km from
the hospital, which covers parts of the region. Patients
living further away are not provided with any support
from the mobile team.
3.2 Data Analysis
A deductive thematic analysis was conducted with
Technology, HCI, Clinics and Sustainability as the
four predefined themes. The analysis was conducted
as content analysis based on audio recordings and the
transcribed recordings. Each researcher conducted an
individual analysis, followed by discussions on the
various findings to conclude the material. The
individual analysis was formed by the steps in
meaning units, condensation, code, category, and
themes (Elo and Kyngäs, 2008, Bengtsson, 2016,
Erlingsson and Brysiewicz, 2017).
As pointed out by Gibbs (2018) there are both pros
and cons with the use of Computer Assisted
Qualitative Data AnalysiS (CAQDAS) tools to assist
the analysis process. CAQDAS, is a term, introduced
in 1991, that refers to the wide range of software now
available that supports data analysis in qualitative
work. At the same time as the software provides a
structured and powerful way to manage the analysis,
CAQDAS has also been criticised for inflexibility,
and for creating distance between the researcher and
the data (Gibbs, 2018). However, the latest versions
of CAQDAS tools have improved the flexibility, and,
when several researchers collaborate, a common
computer assisted structure can be of value. A
CAQDAS tool facilitates the process of storing,
organising, categorising and visualising the gathered
data. The common CAQDAS used in this study was
the NVivo tool (Alfasoft, 2018).
3.3 Ethical Considerations
The ethical considerations relate to the informants
taking part in this study and the consequences of the
actual research (Helgesson, 2015). The informants
were all briefed on and responded to informed
consent, including details such as the right to
withdraw from the interview or interview questions
and personal integrity. Further, the purpose of
collecting the informant material is solely for research
purposes.
This study does not consider the individual third
person, such as patients performing stroke
rehabilitation, but does discuss stroke rehabilitation in
general. Therefore, interview questions related to
individual patients were omitted, as well as specific
training programs or patient names for further
interviews. To protect the informants, their names are
omitted in the transcriptions, while the transcriptions
are stored at the local university’s appointed and
password saved information system for empirical
material.
The consequences of the actual research is
determined by clinical and social aspects, since the
focus is on the usability for stroke rehabilitation and
the patient. The technology requirements are
subordinated, since technology is supposed to support
the patient.
4 FINDINGS
The process of defining testbed requirements for
technology enhanced stroke rehabilitation was
conducted holistically, but with requirements divided
into the categories of Technical, HCI, Clinical and
Sustainability requirements. The categories have
several interrelations, but findings are presented
separately.
4.1 Technical Requirements
Physical damage has large variations between
different persons and stroke recovery is
heterogeneous in its nature (Langhorne et al., 2011).
As highlighted by Informant 1, the rehabilitation has
to be individually adapted with more advanced
technology enhanced solutions for patients that have
the cognitive ability to use a text based and complex
interface. For this target group, the use of virtual
reality and interactive video gaming may be
beneficial for the motoric recovery (Laver et al.,
2015), and that the language relearning can be
facilitated by various standard applications for
Testbed Requirements for Technology Enhanced Stroke Rehabilitation to Support Independent Living
177

language training. Preferably, these applications
should involve features for recording and replaying
the patients’ pronunciation exercises. (Informant 1)
Considering more severely damaged patients,
language skills can be lacking and the
recommendation is to use image based applications,
which can be used to diagnose the damage level
(Dobkin, 2004). An example of an image based tool
are the so-called ‘Talking photographs’, applications
that can be run from a tablet or a smart-phone
(Informant 1). Some patients have a damage level
where the initial training has to be carried out by oral
exercises with repetition and mimicking only, and
many patients have a visual impairment caused by the
stroke. (Informant 1)
For patients with mild-to-moderate upper
extremity motor impairment, low-cost, off-the-shelf
exergames connected to sensors seem an interesting
add-on alternative (Laver et al., 2015, Tsekleves et
al., 2016). Considering patients with more severe
motor impairment, a solution might be to use
technology based on eye-tracking navigation
(Informant 2). Finally, a crucial factor for technology
enhanced services is the quality, or existance, of
internet connections in the patients’ homes. There are
still several blank spots without internet access in
some the region’s remote areas (Informant 3-5).
4.2 HCI Requirements
Human-computer interaction (HCI) is an established
field in computer science where designing, evaluating
and implementing interactive computing systems is
considered from the user’s perspective (Gulliksen,
2017). The requirements should be considered from
the HCI prospective and some important HCI factors
need to be addressed. Several theoretical findings
showed those critical HCI factors are trust in different
forms, personal integrity, technology acceptance and
e-health literacy (Fischer et al., 2014, Veer et al.,
2015, Ahmad and Mozelius, in press).
The approach of older adults towards e-health
applications is different from younger people and
they feel difficulty in adopting those applications
(Fischer et al., 2014). As reported by Informant 1, not
all people accept Technology Enhanced Systems and
few of them are actually set against them. Older
adults especially have difficulty using e-health
applications (Informant 1).
Despite the fact that a large amount of resources
are invested on Technology Enhanced Systems, they
are not easy to adopt for patients and there are some
issues regarding usability and perception of
usefulness which need to be addressed (Haslwanter,
2018). During the interviews, both Informants 1 and
2 emphasized heavily the importance to consider the
aspects and requirements of usability and usefulness
of technology enhanced services (Informant 1;
Informant 2). Informant 1 described that there are
many different kinds of mobile phone or iPad based
applications available for stroke rehabilitation and
they recommend them for the patients’ use. The
usability of those applications depends heavily how
much a patient is affected by stroke and how much
their brain has been damaged (Informant 1).
While designing e-health services, personal
integrity and patient’s privacy should be considered
as a critical issue and Healthcare providers need to
consider it while deploying technology-enhanced
systems such as monitoring cameras (Courtney et al.,
2008, Ahmad and Mozelius, in press). Three
informants mentioned that patients are very much
concerned about their privacy and personal integrity
(Informant 3 - Informant 5).
Several studies highlighted the importance of e-
health literacy to increase the usability of e-health
services for older adults (Ahmad and Mozelius, in
press, Vines et al., 2015). The use of web applications
in stroke rehabilitation depends on the understanding
of these applications and there should be clear
guidelines and instructions to use these applications
(Informant 1, Informant 5). Older adults especially
have more difficulties using mobile applications
because of their lesser understanding of how to use
them (Informant 1).
4.3 Clinic Requirements
This striking disease is caused by interruption of the
blood supply to the brain because an artery to the
brain is either blocked (ischaemic stroke) or bursts
(hemorrhagic stroke) and it damages the brain tissues
(Yamato et al., 2016).
The rehabilitation must be carefully adapted to
each individual, and how stroke has affected a
patient’s abilities show large variations (Informant 1).
Depending on where in the patient’s brain the damage
is located, there can be a wide variety of disabilities
that need rehabilitation (Informant 2). An important
principle is to start the rehabilitation as soon as
possible (Informant 1; Informant 2), and preferably in
two or three days after the stroke has occurred
(Informant 2). How the rehabilitation should be
carried out in detail depends on the patient’s cognitive
and motoric condition, and a technology enhanced
rehabilitation has the best probability to be successful
for patients with milder cognitive and motoric
disabilities (Informant 1; Informant 2).
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
178

Stroke rehabilitation could be divided into three
main categories: cognitive, motoric and speech
rehabilitation (Informant 3-5). According to the
informants, there is a potential for technology
enhancement in all the categories, but probably not
for stroke patients with more severe disabilities
(Informant1; Informant 3). In a rough estimation at
least 25% of the patients could benefit from various
types of technology enhanced support (Informant 1).
Specific to the investigated region is that the
population is evenly spread out with the city of
Östersund as the central hub (Informant 2). The
mobile stroke team visits patients in their homes if
they live inside the 70 kilometre radius that defines
their working range. Patients living outside the radius
are excluded from the services that are carried out by
the mobile stroke team.
4.4 Sustainability Requirements
Sustainability is created by finding the balance
between its three pillars: environmental, social and
economic (Brundtland, 1987), aiming for a wished
end-goal, here the stroke rehabilitation.
Sustainability is usually discussed as a direction for
fulfilling today’s need by not sacrificing the coming
generations’ possibilities to fulfilling their needs.
Detailing the pillars shows that environmental
sustainability, often viewed as the fundamental part,
deals with maintaining long-term human and material
resources. Here the human resources, looked upon as
social sustainability, includes every possible patient
in need of stroke rehabilitation and their specific
needs (Informant 1 - Informant 5).
The economic sustainability derives from the
ability for everyone to afford to take part in stroke
rehabilitation and the efficient use of co-workers’
time (Informant 1 - Informant 5). One primary reason
for economic sustainability equalising efficiency
might be the lack of financial resources in the region.
Equalisation between technological development and
economic growth, and further between economic
growth and sustainable development, is far from
unproblematic. One problem is to understand the
equalisation in itself, and another is defining
development as sustainable.
Social sustainability includes meeting the patient
at their level, supporting them in feeling secure,
performing everyday courses, and performing
exercises related to their physical level (Informant 3 -
Informant 5). There is, therefore, a need for flexibility
related to social sustainability, e.g. while using TES
in a health care context or at home. One such could
be the variation for cognitive rehabilitation, where
some of the patients need everyday instruction and
evaluation. Another social perception is that of joyful
and inspirational rehabilitation. Their view is that
younger patients might view using TES as more
inspiring than physical rehabilitation and thereby be
more likely to use it.
The economic sustainability was discussed
concerning both the patients and the co-workers. For
rehabilitation in the patient’s home, the software
needs to be affordable, both in consideration to the
investment, implementation, and maintenance. The
latter is discussed as the Mid Sweden region does not
offer any maintenance technicians for home support
(Informant 3 - Informant 5). Related to that is the cost
for power supply and other surrounding costs.
Therefore, the informants view the health care
context as more economically sustainable, regarding
implementation and maintenance. The other view on
economic sustainability is that of the co-workers.
Using TES, regardless of context, can make them
more efficient timewise. They view driving far to
meet the patient for half an hour as a waste of time in
comparison to talking to them, e.g., using Skype or
cell phone. The saved time could be used for quality
improvements, not further specified. They did discuss
the office situation, and finding needs for
reconstruction related to privacy concerns.
The environmental sustainability was not
highlighted by the respondents, and was more viewed
as a foundation. Environmental sustainability refers
to the long distances, where the co-workers need to
drive for several hours per workday to meet the
patients in person (Informant 2 - Informant 5).
However, one idea to make the implementation more
environmental in a friendly way was to use
geographically closed health care centres that include
space for self-care situations, such as measuring
blood pressure (Informant 3).
5 DISCUSSION
What is specific for the investigated region is the
heterogenous demographic spread around Östersund
as the central hub for healthcare. The relatively long
distances inside the 70 km work radius for the stroke
team raised thoughts about telecommunication and
technology enhanced services. An ordinary 20
minutes home visit for the mobile stroke team could
involve a 2 hour car drive in both directions
(Informant 3-5). However, all informants agree on the
importance of human-to-human interaction and that
technology should be tested as a complement and not
as a replacement.
Testbed Requirements for Technology Enhanced Stroke Rehabilitation to Support Independent Living
179

There seems to be a potential for using e-services
in all three stroke rehabilitation categories with
obvious benefits in the motoric rehabilitation.
Exergames and other game-based solutions would be
interesting adjunctive alternatives (Karasu and Batur,
2018) but always with the principle of a careful
individual adaptation. As pointed out by Pollock et al.
(2014), the effectiveness of a treatment depends upon
the patient’s physical and mental condition. Therefore
physiotherapists should choose the treatment
according the patient’s medical requirements
(Pollock et al., 2014).
Considering the speech rehabilitation there are
also a wide range of software for articulation
exercises and language relearning (Informant 1). A
speech therapist can prescribe the combination of
hardware and software that has been selected for a
patient. However, not all patients have the computer
skills or the visual ability to use all existing
applications. A custom built, tablet-based stroke
rehabilitation platform with software applications for
speech rehabilitation has been tested with promising
results in Canada (Pugliese et al., 2017).
The cognitive rehabilitation might use both games
and software for telecommunication (Informant 3).
Patients often suffer from memory impairment and a
digital game based approach could be an appreciated
complement to traditional rehabilitation (Withiel et
al., 2018). Finally, the concept of telecommunication
was brought up by the mobile stroke team, and also
the idea of testing a mobile robot based
communication tool in patients’ home environments
(Informant 3-5).
Stroke is one of the most common causes of
physical, cognitive and speech disabilities. Right after
stroke, effective and urgent rehabilitation is needed in
order to overcome or decrease the disabilities.
Technology Enhanced Systems can play a vital role
here (Zhang et al., 2016). However, there are some
critical factors that need to be addressed while
constructing these systems. Things should be seen
from the user perspective and human requirements
should be fulfilled.
Technical requirements have to be carefully
outlined. The willingness to use Technology
Enhanced Systems heavily depends upon the
perceived benefits of using these technologies,
quality of information and training to use them,
degree of joyfulness in these technologies, the
medical condition of the patient after stroke and the
age group of the patient. All the informants agreed
that technology-supported solutions should be
interactive, interesting and joyful to increase the ease
of use and to meet the above mentioned requirements
(Informant 1 - Informant 5). As suggested by many
studies, attitude towards contemporary technologies
depends upon usefulness, usability, education and
training, previous experiences and trust on these
technologies (Broeren et al., 2008, Fischer et al.,
2014, Lee and Coughlin, 2015, Zhang et al., 2016).
An important part of the HCI requirements is to
consider trust and privacy. Patients are in general
concerned about privacy and integrity, and even more
when it comes to the use of monitoring devices
(Informant 3 - Informant 5). Finally, the economic
sustainability needs further investigation, and with
the perspective that efficiency always should be
related to patients’ personal integrity and social
sustainability. Technology must be a complement and
support social interaction and not only a cost-
effective substitute.
6 CONCLUSION
With the help of surprisingly collaborative and open-
minded informants, the study has generated useful
general requirements for further future testing and for
the planned implementation of a testbed. However,
in all of the three found rehabilitation categories,
motoric, cognitive and speech rehabilitation, there is
a need for more specific requirements.
Some important benefits and barriers have also
been discovered in the field of technology enhanced
stroke rehabilitation. Technology enhanced solutions
seem to have a potential to support independent
living, but only if HCI requirements such as trust,
privacy and user-friendliness are met. Stroke patients
often suffer from memory impairment and visual
impairment and therefore the requirements for user-
friendliness need to be stricter than for just any
ordinary technology enhanced solution. Finally,
findings have also contributed to a better
understanding of the specific health care conditions in
the Mid Sweden region.
7 FUTURE WORK
This study defined the more general requirements for
a future testbed implementation for technology
enhanced stroke rehabilitation. The natural next step
would be to define more specific testbed technical
and HCI requirements for each of the three found
rehabilitation categories. From a longer perspective,
the presented requirements should be used as part of
the design and implementation of a future testbed.
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
180

REFERENCES
Ahmad, A.,Mozelius, P. Critical Factors for Human
Computer Interaction of eHealth for Older Adults. In
proceedings of The 5th International Conference on e-
Society, e-Learning and e-Technologies (ICSLT 2019),
in press.
Alfasoft. 2018. What is NVivo? [Online]. from:
http://www.alfasoft.com/en/products/statistics-and-
analysis/nvivo.html. [Accessed 11/11/2018].
Axelsson, S. W.,Wikman, A. M. 2016. Ready for eHealth.
Older Swedes’ Perceptions of eHealth Services: Using
the PIADS Scale as a Predictor for Readiness.
Technologies, 4(3).
Bengtsson, M. 2016. How to plan and perform a qualitative
study using content analysis. NursingPlus Open, 2,8-14.
Billis, A. S., Papageorgiou, E. I., Frantzidis, C. A., Tsatali,
M. S., Tsolaki, A. C.,Bamidis, P. D. 2015. A decision-
support framework for promoting independent living
and ageing well. IEEE journal of biomedical and health
informatics, 19(1), 199 - 209.
Bowes, A.,McColgan, G. 2013. Telecare for older people:
promoting independence, participation, and identity.
Research on Aging, 35(1).
Broeren, J., Bjorkdahl, A., Claesson, L., Goude, D.,
Lundgren-Nilsson, A., Samuelsson, H., Blomstrand, C.,
Sunnerhagen, K. S.,Rydmark, M. 2008. Virtual
rehabilitation after stroke. Studies in health technology
and informatics, 136, 77.
Brundtland, G. H. 1987. Brundtland Report. Our Common
Future. In: MUNDIAL, C. (ed.).
Chaaraoui, A.,Florez-Revuelta, F. 2016. Technologies and
Applications for Active and Assisted Living. Current
situation.
Christophorou, C., Kleanthous, S., Georgiadis, D.,
Cereghetti, D. M., Andreou, P., Wings, C.,
Christodoulou, E.,Samaras, G. 2016. ICT
services for active ageing and independent living:
identification and assessment. Healthcare technology
letters, 3(3), 159 - 164.
Courtney, K. L., Demeris, G., Rantz, M.,Skubic, M. 2008.
Needing smart home technologies: the perspectives of
older adults in continuing care retirement communities.
Informatics in Primary Care, 16, 195 - 201.
Chaaraoui, A., Florez-Revuelta, F., 2016. Technologies and
Applications for Active and Assisted Living. Current
situation.
Dobkin, B. H. 2004. Strategies for stroke rehabilitation. The
Lancet Neurology, 3(9), 528-536. The Lancet
Neurology, 3(9), 528 - 536.
Ehn, M., Hansson, P., Sjölinder, M., I.L. Boman, Folke, M.,
Sommerfeld, D., Borg, J.,Palmcrantz, S. 2015. Users
perspectives on interactive distance technology
enabling home-based motor training for stroke patients.
In pHealth, 145 - 152.
Elo, S.,Kyngäs, H. 2008. The qualitative content analysis
process. Journal of advanced nursing, 62, 107-115.
Erlingsson, C.,Brysiewicz, P. 2017. A hands-on guide to
doing content analysis. African Journal of Emergency
Medicine, 7, 93-99.
Fischer, S. H., David, D., Crotty, B. H., Dierks, M.,Safran,
C. 2014. Acceptance and use of health information
technology by community-dwelling elders.
International journal of medical informatics, 83(9), 624
- 635.
Gibbs, G. R. 2018. Analyzing qualitative data, SAGE.
Gulliksen, J. 2017. Institutionalizing human-computer
interaction for global health. Global health action,
10(sup3), 1344003.
Gwozdz, W.,Sousa-Poza, A. 2010. Ageing, health and life
satisfaction of the oldest old: An analysis for Germany.
Social Indicators Research, 97(3), 397 - 417.
Haslwanter, J. D. H. Review of Telecare Technologies for
Older People. In International Conference on
Computers Helping People with Special Needs, 2018.
Springer, Cham, 407 - 415.
Helgesson, G. 2015. Forskningsetik, Lund,
Studentlitteratur.
Hevner, A. R., March, S. T., Park, J.,Ram, S. 2004. Design
Science in Information Systems Research MIS
Quarterly, 28, 75-105.
Johannesson, P.,Perjons, E. 2014. An introduction to design
science. , Springer.
Karasu, A. U., Batur, E. B. 2018. Effectiveness of Wii-
Based Rehabilitation in Stroke: A Randomized
Controlled Study. Journal of rehabilitation medicine,
50(5), 406-412.
Langhorne, P., Bernhardt, J.,Kwakkel, G. 2011. Stroke
rehabilitation. The Lancet, 377(9778), 1693-1702.
Langhorne, P., Coupar, F.,Pollock, A. 2009. Motor
recovery after stroke: a systematic review. The Lancet
Neurology, 8(8), 741-754.
Laver, K. E., George, S., Thomas, S., Deutsch, J. E.,Crotty,
M. 2015. Virtual reality for stroke rehabilitation.
Cochrane database of systematic reviews, (2).
Lee, C.,Coughlin, J. F. 2015. PERSPECTIVE: Older adults'
adoption of technology: an integrated approach to
identifying determinants and barriers. Journal of
Product Innovation Management, 32(5), 747 - 759.
Palmcrantz, S., Borg, J., Sommerfeld, D., Plantin, J., Wall,
A., Ehn, M., Sjölinder, M.,Boman, I. L. 2017. An
interactive distance solution for stroke rehabilitation in
the home setting–A feasibility study. Informatics for
Health and Social Care, 42(3), 303 - 320.
Peek, S., Luijkx, K. G., Rijnaard, M. D., Nieboer, M. E.,
Voort, C. S. v. d., Aarts, S., Hoof, J. B. v., Vrijhoef, H.
J. M. c.,Wouters, E. J. 2016. Older adults' reasons for
using technology while aging in place. Gerontology,
62(2), 226 - 237.
Peel, N., Bartlett, H.,McClure, R. 2004. Healthy ageing:
how is it defined and measured? Australasian Journal
on Ageing, 23(3), 115 - 119.
Peffers, K., Tuunanen, T., Rothenberger, M. A.,Chatterjee,
S. 2007. A design science research methodology for
information systems research. Journal of management
information systems, 24(3), 45-77. Journal of
management information systems, 24(3), 45 - 77.
Pollock, A., Baer, G., Campbell, P., Choo, P. L., Forster,
A., Morris, J., Pomeroy, V. M.,Langhorne, P. 2014.
Physical rehabilitation approaches for the recovery of
Testbed Requirements for Technology Enhanced Stroke Rehabilitation to Support Independent Living
181

function and mobility following stroke. Cochrane
Database of Systematic Reviews, (4).
Pugliese, M. W., Wilson, K., Guerinet, J., Atkinson, K. M.,
Mallet, K. H., Shamloul, R., ... & Dowlatshahi, D. 2017.
Mobile Tablet-Based Stroke Rehabilitation: Using
mHealth Technology to Improve Access to Early Stroke
Rehabilitation. International Journal of Interactive
Mobile Technologies (iJIM), 11(1), 148-157.
Rizzo, A. S.,Kim, G. J. 2005. A SWOT analysis of the field
of virtual reality rehabilitation and therapy. Presence:
Teleoperators & Virtual Environments, 14(2), 119 -
146.
SCB 2016. Sweden - Population in the provinces on 31
December 2014.
Seniów, J., Litwin, M., Litwin, T., Leśniak,
M.,Członkowska, A. 2009. New approach to the
rehabilitation of post-stroke focal cognitive syndrome:
Effect of levodopa combined with speech and language
therapy on functional recovery from aphasia. Journal of
the neurological sciences, 283(1-2), 214-218.
Thomsson, H. 2002. Reflexiva intervjuer. Studentlitteratur,
Lund, Studentlitteratur.
Tsekleves, E., Paraskevopoulos, I. T., Warland,
A.,Kilbride, C. 2016. Development and preliminary
evaluation of a novel low cost VR-based upper limb
stroke rehabilitation platform using Wii technology.
Disability and Rehabilitation: Assistive Technology,
11(5), 413-422.
UN 2015. Department of Economic and Social Affairs,
population division. Trends in contraceptive use
worldwide [Internet].
Veer, A. J. d., Peeters, J. M., Brabers, A. E., Schellevis, F.
G., Rademakers, J. J. J.,Francke, A. L. 2015.
Determinants of the intention to use e-Health by
community dwelling older people. BMC health services
research, 15(1), 103.
Veerbeek, J. M., Wegen, E. v., Peppen, R. v., Wees, P. J. v.
d., Hendriks, E., Rietberg, M.,Kwakkel, G. 2014. What
is the evidence for physical therapy poststroke? A
systematic review and meta-analysis. PloS one, 9(2),
e87987.
Vines, J., Pritchard, G., Wright, P., Olivier, P.,Brittain, K.
2015. An age-old problem: Examining the discourses of
ageing in HCI and strategies for future research. ACM
Transactions on Computer-Human Interaction
(TOCHI), 22(1), 2.
Withiel, T. D., Sharp, V. L., Wong, D., Ponsford, J. L.,
Warren, N., Stolwyk, R. J. 2018. Understanding the
experience of compensatory and restorative memory
rehabilitation: A qualitative study of stroke survivors.
Neuropsychological rehabilitation, 1-20.
Yamato, T. P., Pompeu, J. E., Pompeu, S. M.,Hassett, L.
2016. Virtual reality for stroke rehabilitation. Physical
therapy, 96(10), 1508 - 1513.
Zhang, H., Shen, Z., Lin, J., Chen, Y.,Miao, Y. 2016.
Familiarity design in exercise games for elderly. Int J
Inf Technol, 22, 1 - 19.
ICT4AWE 2019 - 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health
182
