
Myofascial Release and Ultrasound, versus Deep Friction Treatment:
Which Is the Best for Patients with Tennis Elbow Injuries?
Safrin Arifin
1
and Karin Amalia Safitri
2
1
Physiotherapy Laboratory, Vocational Education Program, Universitas Indonesia, Depok, Indonesia
2
Insurance Administration and Actuary, Vocational Education Program, Universitas Indonesia, Depok, Indonesia
Keywords: Myofascial Release, Ultrasound, deep friction, tennis elbow.
Abstract: Tennis elbow is an inflammation of the tendons that join the forearm muscles on the outside of the
elbow. The forearm muscles and tendons become damaged from overuse repeating the same motions
again and again. This leads to pain and tenderness on the outside of the elbow. Rehabilitation programs
do help reduce the pain. Research aims: This research aims to compare between myofascial Release and
Ultrasound versus deep friction treatment and determine the best treatment for reducing pain for Tennis elbow
patients. Methodology: This study used a double-blind experimental design with an alpha value of 5%. The
study was conducted at the Clinic "Rumah Fisio." Based on the randomization technique, the sample was
drawn from the list of patients who are diagnosed with Tennis elbow and undergoing physiotherapy from
December 2018 to February 2019. The pain was measured using the Visual Analogue Scale (VAS). Research
findings: The results of the t-test analysis showed that Deep Friction (DF) [mean = 6,6 ; SD = 0.41, p = 0.000]
is more effective than Myofascial Release techniques and Ultrasound (MrU) (mean = 4.8 ; SD = 0,82) in
reducing pain for Tennis Elbow patients. Practical implications: This study offers an understanding of the best
treatment that would help in reducing the tennis elbow pain.
1 INTRODUCTION
Tennis elbow is a local inflammation near the
proximal (upper) attachments of wrist extensor
muscles, characterized by pain on palpation of the
lateral epicondyle of the humerus and in resisted
movements against wrist extension. It is a syndrome
of overuse (e.g., use of computer mouse, racquet
sports) that can result in considerable socioeconomic
costs resulting from a prolonged leave of absence
from work
11'
Myofascial release technique is the
facilitation of mechanical, neural and psycho-
physiological adaptive potential as interfaced via the
myofascial system.
Ultrasound therapy used in
physical medicine to relieve pain and increase joint
mobility
5
. Ultrasound increases blood flow and
oxygen to the affected area by increasing muscle
temperature. Clinical studies show that it has limited
effectiveness in reducing disability caused by tennis
elbow. However, when ultrasound is combined with
physical therapy such as massage and strengthening
and stretching exercises, its effectiveness increases.
In the research conducted by Haris Begovic and
Guan-Quan Zhou, showed, Ultrasound and Strain
gauge trigger changes in contractile properties and
transmission of style after the friction massage
Transfer is applied to the quadriceps tendon. This
change is displayed by the signal onset, which
provides information about the transmission of force
and stiffness in the elastic component. There is
evidence to justify the widespread use of ultrasound,
and one of them is related to its potential analgesics.
Our findings indicate that therapists pay attention to
increased pain after the use of ultrasound. These
results were also found by other studies that showed
ultrasound as an analgesic promoter that has the
potential to produce satisfactory results for pain
associated with the trigger point and decrease in
reported low back pain. Deep transverse friction is
applied perpendicular to the fibre in pushing each
strand in the trigger area which gives a mechanical
effect, local hyperemia, analgesia, and the
relationship of scar tissue to the structure of the
ligaments, tendons and muscles. Deep, transverse
friction can cause stimulation of nociceptive ends
connected to Aδ fibres and mechanoreceptors found
in soft tissue attached to large diameters of Aβ fibres.
This large diameter fibre affects cells in the posterior
Arifin, S. and Amalia Safitri, K.
Myofascial Release and Ultrasound, versus Deep Friction Treatment: Which is the Best for Patients with Tennis Elbow Injuries?.
DOI: 10.5220/0010684100002967
In Proceedings of the 4th International Conference of Vocational Higher Education (ICVHE 2019) - Empowering Human Capital Towards Sustainable 4.0 Industry, pages 345-348
ISBN: 978-989-758-530-2; ISSN: 2184-9870
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
345
horn cell and also facilitates the transmission of
small-diameter nociceptive information until the
safety gate is closed
From some of the studies above, no one has done
research directly between myofascial Release and
ultrasound versus deep transfer friction, because from
my practice experience at Rumah Fisio clinic, two
streams are used for patient therapy with each
claiming is that my flow is the best result because the
latest scientific journal supports it. Therefore I am
very interested in conducting a study based on
experimental studies.
2 METHODOLOGY
This study used a double-blind experimental design
with a pre-post-test design of two groups. The study
was divided into two groups, consisting of group 1
with Myofascial Release techniques and ultrasound
and group 2 with deep, transverse friction . with an
alpha value of 5%. The study was conducted at the
Clinic "Rumah Fisio." Based on randomization
technique, The number of study respondents was ten
people, treatment group 5 people and control group 5
people the sample was drawn from the list of patients
who are diagnosed with Tennis elbow and
undergoing physiotherapy from December 2018 to
February 2019. The pain was measured using the
Visual Analogue Scale (VAS).
3 RESULTS
Table 1: Distribution of Respondents by Gender.
Gender Mr
Per cent
(
%
)
D.F.
Per cent
(
%
)
Male 5 100 5 100
Female 0 0 0 0
Total 5 100 5 100
Based on table 1. Appears in the group treatment
MrU (group 1) has a sample with gender five male
(100%). Whereas at group treatment D.F. (group 2)
has an example with gender five male (100%)
Table 2. Distribution of respondents by age.
M
rU D
F
characteristic mean S.D. mean SD
age 29.50 3.37 29.56 2.92
Table 2 shows, the sample MrU has a mean age
of 29.50 years old and in D.F. groups has an average
age of 29.56 years past.
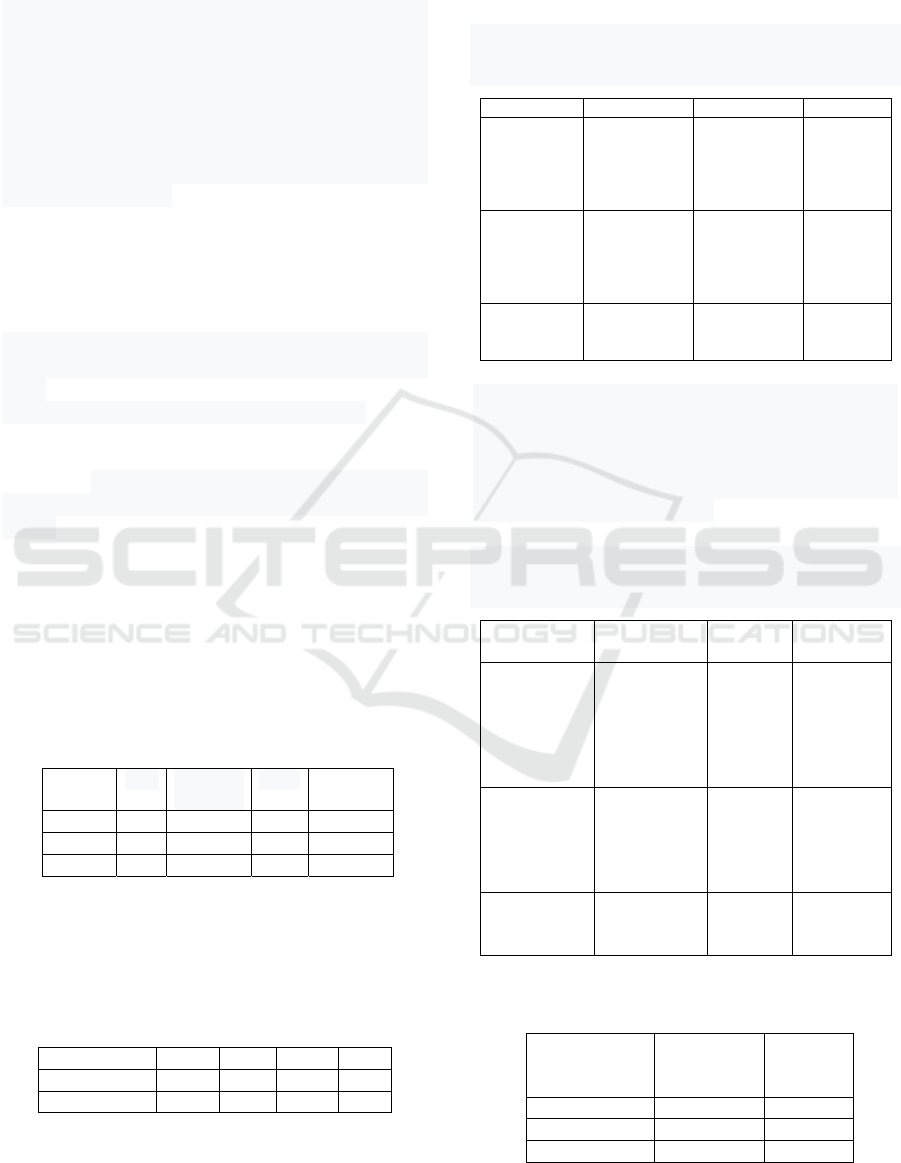
Table 3.: Distribution of Respondents Based on Pain
Measurement with VAS (Visual Analogue Scale) units of
mm (millimeters) in groups MrU.
Respondents Pain scale
Before
intervention
Before
intervention
Differenc
es before
& after an
interventi
on
1
2
3
4
5
8,3
8,7
9,1
8,4
9,0
3,7
2,9
5,5
3,1
4,2
4,6
5,8
3,6
5,3
5,8
Total
Mean ±
SD
5
8,7
±0,35
5
3,88
±1,04
5
4,82
± 0,82
Based on table 3, the average value of pain
measurement using VAS in MrU group before
treatment is 8,7 and after surgery is 3.8. the average
difference of pain measurement value by using VAS
before and after treatment is 4.82, and the amount of
the standard deviation is 0.82.
Table 4: Distribution of Respondents Based on Pain
Measurement with VAS (Visual Analogue Scale) units of
mm (millimetres) in groups D.F.
Respondents Pain
scale
Before
intervention
Before
interven
tion
Differenc
es before
& after
the
interventi
on
1
2
3
4
5
9,1
8,7
9,3
8,4
8,9
2,6
1,9
2,2
1,6
2,9
6,5
6,8
7,1
6,8
6,0
Total
Mean ±
SD
5
8,8
±0,34
5
2,24
±0,5
5
6,6 ±
0,4
Table 5: The results of Normality Test data degree of tennis
elbow pain before and after treatment.
Pain scale P Value
(Saphiro
wilk test)
Tennis elbow MrU DF
Before 0,501 0,976
Afte
r
0,519 0,919
ICVHE 2019 - The International Conference of Vocational Higher Education (ICVHE) “Empowering Human Capital Towards Sustainable
4.0 Industry”
346

Based on table 5 it can be seen the results of
normality test data on the MrU group with the
probability value in the pre-test (p-value) is 0.501, so
it can be concluded that the data are normally
distributed (p> 0.05). The probability value in the
post-test (p-value) is 0.519, so it can be found that the
data has a normal distribution (p> 0.05). Data
normality test results in the D.F. group with the
probability value in the pre-test (p-value) is 0.976,
and it can be concluded that the data are typically
distributed (p> 0.05). The probability value in the
post-test (p-value) is 0.919, so it can be found that the
data is normally distributed (p> 0.05).
Tabel 6: Hasil T-test untuk Uji Hipotesis.
n Mean ± S.D. p
MrU 5 4,8 ± 0,82 0,000
DF 5 6,64 ± 0,41 0,000
Based on table 6. the value of pain measurement in
the treatment group I, namely the administration of
myofascial Release, which was analyzed using the
Paired Sample T-test obtained probability value (p-
value) of 0,000. The probability value is smaller than
0.05 (p <0.05), this means that Ha is accepted and Ho
is rejected. It can be concluded that in hypothesis I
there is an influence of myofascial Release and
Ultrasound on pain reduction in tennis elbow.
Hypothesis II test is to determine the effect of deep,
transverse friction on pain reduction in tennis elbow.
To test hypothesis II, the Paired Sample T-test was
used.
Based on table 6. the value of pain measurement
in treatment group II, namely the provision of deep,
transverse friction which was analyzed using the
Paired Sample T-test obtained probability value (p-
value) of 0,000. The probability value is smaller than
0.05 (p <0.05), this means that Ha is accepted and Ho
is rejected. It can be concluded that in hypothesis II
there is an effect of giving deep transversion friction
to decrease pain in tennis elbow
4 CONCLUSION
Based on the results of the research, it can be
concluded that DF [mean = 6,6, SD = 0.41, p = 0.000]
is more effective than MrU (mean = 4.8, SD = 0,82)
in reducing the pain of tennis elbow patients. The
results of One-Way ANOVA study also showed that
there was a significant difference in the decrease of
pain produced by frequency treatment of D.N. & E.S.
[F (1, 6) = 12,333, p = 0,007].
ACKNOWLEDGEMENTS
The author would like to thank Allah Azza Wa Jalla,
my dear Hannah, Vinka, Juno & Echa. Sincere
gratitude for Prof. Sigit and the doctor's team for the
valuable discussions and assistance during the
drafting process.
REFERENCES
Begovic, H., Zhou, G., Schuster, S., & Zheng, Y. 2016. The
neuromotor effects of transverse friction massage.
Manual Therapy, 26, 70-76
DOI:10.1016/j.math.2016.07.007.
Chaves, P., Simões, D., Paço, M., Pinho, F., Duarte, J. A.,
& Ribeiro, F. 2017. Cyriax's deep friction massage
application parameters: Evidence from a cross-
sectional study with physiotherapists. Musculoskeletal
Science & Practice, 32, 92–97.
https://doi.org/10.1016/j.msksp.2017.09.005
De Groef, A., Van Kampen, M., Verlvoesem, N., Dieltjens,
E., Vos, L., De Vrieze, T., Christiaens, M. R., Neven,
P., Geraerts, I., & Devoogdt, N. 2017. Effect of
myofascial techniques for treatment of upper limb
dysfunctions in breast cancer survivors: a randomized
controlled trial. Supportive care in cancer: official
journal of the Multinational Association of Supportive
Care in Cancer, 25(7), 2119–2127.
https://doi.org/10.1007/s00520-017-3616-9
Doley M., Warikoo D., Arunmozhi R. 2013. Effect of
Positional Release Therapy and Depp Transverse
Friction Massage of Gluteus Medius Trigger Point-A
Comparative Study. Journal of Exercise Science and
Physiotherapy. Vol. 9, No. 1, 40-45.
Gutierrez, M. I., Lopez-Haro, S. A., Vera, A., & Leija, L.
2016. Experimental Verification of Modeled Thermal
Distribution Produced by a Piston Source in
Physiotherapy Ultrasound. BioMed research
international, 2016, 5484735.
https://doi.org/10.1155/2016/5484735
Hassan, S., Hafez, A., Seif, H. and Kachanathu, S. 2016.
The Effect of Deep Friction Massage versus Stretching
of Wrist Extensor Muscles in the Treatment of Patients
with Tennis Elbow. Open Journal of Therapy and
Rehabilitation, 4, 48-54.
DOI: 10.4236/ojtr.2016.41004.
Hari Haran, R., & Singh, A. 2013. Effect of High Power
Pain Threshold Static Ultrasound Combined with
Transverse Friction Massage and Stretching on Upper
Trapezius Myofascial Trigger Point. Indian Journal Of
Physiotherapy & Occupational Therapy-An
International Journal, 7(3), 113-117. Retrieved
from http://www.i-
scholar.in/index.php/ijpot/article/view/42652.
Joshi, S., Metgud, S., & Ebenezer, C., 2013. Comparing the
effects of Manipulation of Wrist and Ultrasound,
Friction Massage and Exercises on Lateral
Myofascial Release and Ultrasound, versus Deep Friction Treatment: Which is the Best for Patients with Tennis Elbow Injuries?
347

Epicondylitis: A Randomized Clinical Study. Indian
Journal of Physiotherapy and Occupational Therapy -
An International Journal. DOI Number:
10.5958/j.0973-5674.7.3.093
Kamali, F., Mohamadi, M., Fakheri, L., &
Mohammadnejad, F. 2019. Dry needling versus friction
massage to treat tension-type headache: A randomized
clinical trial. Journal of bodywork and movement
therapies, 23(1), 89–93.
https://doi.org/10.1016/j.jbmt.2018.01.009
Magri, L. V., Carvalho, V. A., Rodrigues, F. C., Bataglion,
C., & Leite-Panisse, C. R. 2017. Effectiveness of low-
level laser therapy on pain intensity, pressure pain
threshold, and SF-MPQ indexes of women with
myofascial pain. Lasers in medical science, 32(2), 419–
428. https://doi.org/10.1007/s10103-016-2138-x
Mohamadi, M., Piroozi, S., Rashidi, I., & Hosseinifard, S.
2017. Friction massage versus kinesiotaping for short-
term management of latent trigger points in the upper
trapezius: a randomized controlled trial. Chiropractic
& manual therapies, 25, 25.
https://doi.org/10.1186/s12998-017-0156-9
Patra, P., & Nayana, D.N. 2013. Effect of 3-d torque and
muscle splay Techniques on subjects with Posterior
tibial tendon dysfunction: A comparative study.
International Journal of Pharmaceutical and
Biological Research (IJPBR) 4(4).
Santiago, V., & Raphael, K.G., 2018. Perceived helpfulness
of treatments for myofascial TMD as a function of
widespread comorbid pain. Clinical Oral
Investigations, 23, 2929-2939.
https://doi.org/10.1007/s00784-018-02797-6
Vieira, W., Aguiar, K., Silva, K., Canela, P., Silva, F., &
Abreu, B. 2012. Overview of ultrasound usage trends in
orthopaedic and sports physiotherapy. Critical
ultrasound journal. 4. 11. 10.1186/2036-7902-4-11.
ICVHE 2019 - The International Conference of Vocational Higher Education (ICVHE) “Empowering Human Capital Towards Sustainable
4.0 Industry”
348
