
Comparison the Unit Cost of Hemodialysis Service with Dialysis
Service’s Tariff in INA CBGs Universal Health Coverage Programe
(JKN): Case Study Hemodialysis Clinic in Depok
Supriadi
Vocational Education Programme, Universitas Indonesia, Hospital Administration Department,
Keywords: Activity-based Costing, INA Cbgs, Hemodialysis.
Abstract: Comparing the hemodialysis service unit costs calculated by activity-based costing method with INA CBG
tariff for dialysis service in the National Health Insurance Program (JKN). Data was taken from a
hemodialysis clinic that was the provider of the JKN program in the Depok area. Calculation of the unit cost
of hemodialysis services uses the activity-based costing method. This method was started by tracking all
hemodialysis service activities. T The direct and indirect costs of each service activity were traced. The data
used are primary data obtained from interviews with leaders and clinical finance officers, and secondary data
obtained from clinical, operational records, both financial and non-financial records. The results of unit cost
calculations will be compared with the tariff dialysis service in INA CBGs. The results showed that the unit
cost of hemodialysis services using the activity-based costing method was lower than the tariff of dialysis
service in INA CBGs. The results of this study it is used to trace costs and make efficiency in order to reduce
service costs so that real profits can be increased from hemodialysis services
1 INTRODUCTION
The Universal Health Coverage Programme (JKN)
organised by the Health Insurance Administration
Agency (BPJS) began to be implemented on January
1, 2014. The goal of the JKN program is to fulfil the
proper public health needs and are given to everyone
who is registered and has paid contribution, or the
contributions are paid by the government (PMKRI
28, 2014; Noviatri LW, 2016).
In the JKN Program, BPJS Kesehatan
collaborates with first-rate and advanced health
services both government and private. Payment
system for JKN organisers’ health services using two
ways; by capitation and INA CBGs. Capitation
payment is for the primary health services, while
payment by INA CBGs is for the advanced health
services (PMRK 28, 2014).
NA CBGs is a system for determining health care
rates that use the case-mix system is a grouping of
diagnoses and procedures by referring to
similar/similar clinical features and similar/similar
use of resources/ maintenance costs. The grouping is
done using grouper software. The amount of INA
CBG tariff is influenced by the class of hospital or
health service and regionalisation, which is where the
location of the health service is located (PMKRI 27,
2014).
The problem that arises is that INA CBG tariff is
sometimes not in accordance with the real costs
incurred in the services provided. This happens a lot
in hospital services such as in surgical and non-
surgical cases, besides that it is also influenced by the
use of drugs, consumables and medical equipment as
well as treatment classes (Sari RP, 2014;
RayahuningrumIO, Tantomo D, Suryono A 2016).
Hemodialysis services are health services
included in the payment system using INA CBGs.
This service can be done in a hospital and at a special
hemodialysis clinic. Febriani (2016) in his study
found that the real costs incurred for hemodialysis
services at the Medika Stania Hospital in Bangka
were higher than the rates of INA CBGs paid. This is
mainly because the overhead costs are still high and
there are not enough hemodialysis patients (Febriani,
2016).
Hemodialysis services not only in hospitals, there
are now many hemodialysis clinics that serve JKN
patients with the INA CBGs payment system. To find
out the ratio of costs incurred with the INA CBGs
130
Supriadi, .
Comparison the Unit Cost of Hemodialysis Service with Dialysis Service’s Tariff in INA CBGs Universal Health Coverage Programe (JKN): Case Study Hemodialysis Clinic in Depok.
DOI: 10.5220/0010168900002967
In Proceedings of the 4th International Conference of Vocational Higher Education (ICVHE 2019) - Empowering Human Capital Towards Sustainable 4.0 Industry, pages 130-134
ISBN: 978-989-758-530-2; ISSN: 2184-9870
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
tariff for hemodialysis services in the clinic, so the
real unit cost calculation is carried out with the tariff
of INA CBGs in a hemodialysis (HD) clinic in the
Depok area. Real unit cost calculation uses the
Activity Based Costing (ABC) method, where this
method is an ABC cost calculation focusing on
activities carried out to produce a product or service.
The ABC method provides information about the
activities and resources needed to carry out these
activities (Rumumpuk MS, 2013). The ABC method
was developed to accommodate various
shortcomings of traditional calculation methods,
where the ABC method can be to allocate a suitable
cost driver for any activity, and to calculate the cost
price according to the activity (Javid M, Hadian M,
Ghaderi H, Gaffari S, Salehi M
, 2106). This method
will get a summary of the costs of the organisation of
activities by providing more detailed cost information
about health service activities so that it is seen which
activities require large costs and are considered for
efficiency measures (Kazemi Z, Zadeh AH, 2015).
2 METHOD
This research is a descriptive study in which the cost
calculation uses the Activity Based Costing method.
This calculation begins by tracing the activities that
occur in hemodilysis services from start to finish.
After the activity is obtained, the time for each
activity is calculated. Percentage of time each of these
activities will be the cost driver of overhead costs or
indirect costs. For direct costs traced directly for each
time service hemodialysis.
This study use data from January to December
2018 including financial data and non-financial
transactions. Direct cost data is the cost of medicines
and consumables used for each hemodialysis
procedure and doctor’s fee for each patient
consultation. While indirect costs are overhead costs,
including investment depreciation costs, employee
salaries, consumables, utilisation costs, maintenance
costs and others. Charging depreciation of the
building for 5 years, while electronic equipment and
furniture are depreciated for 5 years. Calculation of
depreciation costs using the straight-line method.
The total clinical overhead costs for a year will be
charged to each activity using the percentage cost
driver for each activity. Then the activity costs will be
divided by the number of hemodialysis actions
carried out during 2018 so the overhead or indirect
costs of activity is measured. Finally, this cost is
added to the direct cost of hemodialysis measures,
such as the cost of drugs and medical supplies and the
of a doctor’s services fee. This sum of indirect costs
and direct costs results in unit costs for hemodialysis
services.
Interviews were conducted with clinic managers
to find out operational policies at this clinic, such as
investment depreciation policies, provisions on the
use of hemodialysis tools and others.
3 RESULT AND DISCUSSION
3.1 The Activity of Hemodialysis (HD)
Based on interviews with managers of clinic HD and
observations of HD service actions starting from the
beginning to completion there are several activities
and the time needed for each activity as follows:
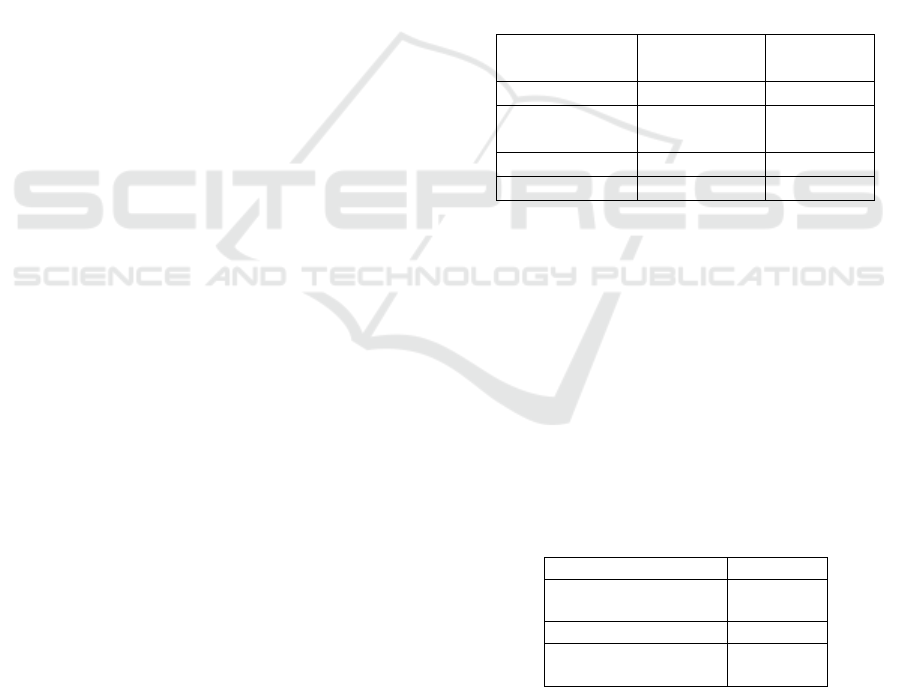
Table 1: HD Service Activity in 2018.
HD Activity Time Percentage
Re
g
istration 5 minutes 2 %
Doctor
Anamnesa
5 minutes 2 %
HD service 240 minutes 96%
Total 250 minute 100%
The percentage of HD service time that will be used
as a cost driver to share indirect cost of the HD
service.
3.2 Direct Cost of HD Services
Direct costs are costs incurred due to the occurrence
of the service, otherwise if there is no service, then
these costs do not arise. In the case of HD service, for
1 time HD service uses a fixed amount of a package
of drugs and medical supplies. In addition, there is a
fee for the doctor who performs the examination and
supervision during HD service. The direct costs are:
Table 2: Direct Cost for Each HD Service in 2018.
Direct Cost Rp
Package of drugs &
medical supplies
335,828,-
Doctor fee 55,000,-
Total Cost 390,828,-
Based on the table above, direct costs for 1 time
HD action amounting to Rp 390,828, - which consists
of the cost of the package of drugs and medical
supplies . The size of the drug package and the cost
of consumables are greatly affected by the number of
times the dialyser is reused. The more frequently used
Comparison the Unit Cost of Hemodialysis Service with Dialysis Service’s Tariff in INA CBGs Universal Health Coverage Programe
(JKN): Case Study Hemodialysis Clinic in Depok
131
again, the smaller direct costs will be. In medical
supplies there is a disposible tool called a dialyser.
This tool can be reused several times. The more
frequently used again, the lower the cost of medical
supplies. For the amount of drug packages and
medical supplies above is for the use of dialysers 5
times.
3.3 Indirect Cost of HD Services
According to the manager of clinic HD that the
building used is not its own, but is rented for 5 years
and will be extended after 5 years. Thera are 7 units
Hemodialysis instrument in this clinic and all of them
is loaned with an Operational Cooperation
Agreement (OCA), while other equipment such as
medical equipment, furniture and electronics are
investment.
In addition to investment depreciation costs, costs
which are indirect costs are electronic depreciation
costs, medical device depreciation and 5-year,
depreciation of the meubeler, employee salary costs,
utilisation costs, maintenance costs and other
consumable costs. All costs calculated are
transactions that occurred in 2018. Details of indirect
costs can be seen in the following table:
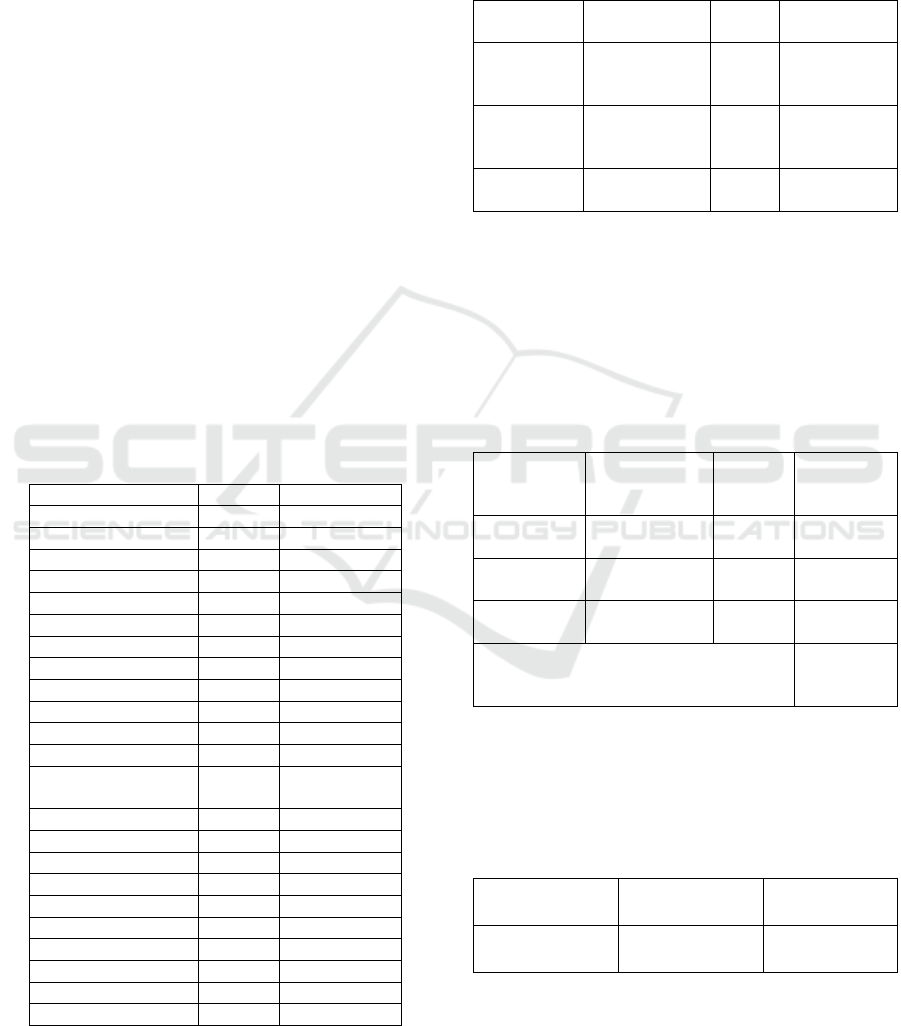
Table 3: Indirect Cost for HD Service in 2018.
Cost Numbe
r
Rp
Depresiasi Inv.
- Clinic Buildin
g
1 unit 25,704,500,-
- AC S
p
lit 5 unit 1,070,000,-
-Medical Instrument total 9,534,000,-
- Meubele
r
total 2,587,600,-
- Computer+Printe
r
3 set 2,480,000,-
- LCD TV 50” 1 unit 1,960,000,-
Salaries
- Manage
r
1 prs 79,625,000,-
- Nurse 4 prs 213,200,000,-
- Marketing Office
r
1 prs 46,150,000,-
- Registration
Office
r
1 prs 37,050,000,-
- Nurse Ai
d
1 prs 27,300,000,-
- Cleaning Service 1 prs 20,410,000,-
Other Cost
Electricit
y
45,102,864,-
- Internet 6,000,000
- Consumables 4,476,000,-
- Food and Beverage 6,300,000,-
- Office Stationer
y
3,042,000,-
- Maintenance 4,227,720,-
Total Cost 561,219,684,-
The indirect costs incurred by HD clinics during
2018 are Rp. 561,219,684. This cost will be allocated
to each HD service activity using the percentage of
time for each activity. The total indirect costs for each
activity for a year are as follows:
Table 3: Indirect Cost Allocated to HD Activity.
HD
Activit
y
Indirect Cost Cost
Drive
r
Cost/year
Registration Rp
561,219,684,-
2 % Rp
11,224,394
Doctor
Anamnesa
Rp
561,219,684,-
2 % Rp
11,224,394
HD Service Rp
561,219,684,-
96% Rp
538,770,896
Table 4 shows the amount of indirect cost for each
activity during 2018. To get the indirect cost of one
time the HD service, must be divided by the number
of HD service in 2018. Based on HD service records
in 2018, the number of HD service are 2,072 services,
so that the indirect cost for one time HD service is as
follows:
Table 5: Indirect Cost Allocated to Each HD Activity.
HD Activity Indirect Cost HD
Service
in 2018
Indirect
Cost/ Serv
Registration Rp
11,224,394
2,072 Rp 5,417,-
Doctor
Anamnesa
Rp
11,224,394
2,072 Rp 5,417,-
HD
Service
Rp
538,770,896
2,072 Rp
260,025,-
Total Indirect Cost Each HD Service Rp
270,859,-
The unit cost calculation of HD services using the
ABC method is to add up the direct costs incurred in
the activities and indirect costs for one HD action as
obtained above. The HD services unit costs can be
seen in the following table:
Table 6: Unit Cost HD Service with ABC Method.
Direct Cost + Indirect
Cos
t
= Unit Cost
Rp 390,828,- + Rp
270,859,-
= Rp
661,687,-
Table 6 shows that for 1 time the HD service
requires direct costs and indirect costs of Rp. 661,687.
Based on interviews with HD clinic managers that the
ICVHE 2019 - The International Conference of Vocational Higher Education (ICVHE) “Empowering Human Capital Towards Sustainable
4.0 Industry”
132

HD clinics are in the category of primary referral
clinics at the level of type D hospitals and are in
regional 1 according to Permenkes RI RI no 64 2016.
For this reason, payments received by these HD
clinics use INA CBGs tariff code is N-3.15.0
(Dialysis Procedure) and the tariff is Rp. 737,700, -
for 1 time HD service (PMKRI 64, 2016).
Compared to the unit cost calculated using the
ABC method on HD services at the HD clinic, it was
obtained at Rp 661,687, with the INA CBGs rate
applicable to this clinic at Rp 737,700, - The profit of
Rp 76,013 was still obtained for each time HD.
Whereas the profit during 2018 was 2,072 HD
services multiplied by Rp 76,013, - equal to Rp
157,498,936.
There are the differ results from Febriani (2016)
for hemodialysis services in the Medika Stania
Hospital in Bangka where real costs were higher than
the INA CBGs tariff paid. This is mainly because
overhead costs are still high and the number of
hemodialysis patients has not been large (Febriani,
2016). Kalhor et al (2016) find that unit costs
calculated using the ABC method in the radiology
department at a hospital in Iran are higher than the
rates determined by the ministry of health11. Noer
(2016) in his research at Charitas Hospital Palembang
found that cost inefficiencies occur in employee
salary costs and maintenance costs. This causes the
high cost of HD services at the hospital (Rusli NT).
According to Febriani (2016) that in addition to
fairly high employee costs, the thing that causes unit
costs to be high is the selection of Operational
Cooperation for HD devices with certain more
expensive brands. This is because the obligation to
purchase medical consumables used in HD services
has been determined by the Operational Cooperation
Agreement (OCA). The use of disposable dialysers is
also the factor that causes the high cost of HD services
in Medika Stania Hospital, Bangka. The results of
interviews with HD clinic managers that OCA is done
not with expensive companies brand, so that the cost
of medical supplies is not too high. On the other hand
the use of dialysers 5 times is also enough to reduce
the cost of HD services at the clinic, so the unit costs
are lower than the INA CBGs tariff for HD services.
4 CONCLUSION
Calculation of HD service unit costs in HD clinics in
Depok area using the ABC method found that the unit
cost was Rp. 661,687, -. This result is lower than the
INA CBGs tariff for HD services received by the
clinic of Rp. 737,700. When compared to other
services which turned out to be a higher unit cost than
JKN tariffs, this was due to, among other things,
Operational Cooperation Agreement with not an
ordinary brand companies so the price of consumable
medical materials that had a lower price compared to
xpensive brands. The use of dialysers 5 times can
reduce costs so that the direct costs are lower than the
INA CBG rates for HD services.
REFERENCES
Febriani, Analisis Perhitungan Unit Cost Pelayanan
Hemodialisi Terhadap Penetapan Tarif INA-CBGs dan
Tarif Rumah Sakit Medika Stannia Kabupaten Bangka.
Tesis. Program Studi Manajemen Rumah Sakit
Program Pascasarjana Universitas Muhammadiyah
Yogyakarta; 2016.
Javid M, Hadian M, Ghaderi H, Gaffari S, Salehi M.
Application of the Activity-Based Costing Method for
Unit-Cost Calculation in a Hospital. Global Journal of
Health Science; Vol. 8, No. 1.;2016.
Kalhor R, Amini S, Majid E, Etall. Comparison of the
Ministry of Health’s tariffs with the cost of radiology
services using the activity-based costing method.
Electronic Physician, Volume, 8;February 2016.
Kazemi Z, Zadeh AH . Activity based Costing: A Practical
Model for Cost Price Calculation in Hospitals. Indian
Journal of Science and Technology, Volume 27; 2015.
Noviatri LW. Sugeng; Analisis Faktor Penyebab
Keterlambatan Penyerahan Klaim BPJS di RS Panti
Nugroho, Jurnal Kesehatan Vokasional, Volume 1,
Nomor 1 ;Oktober 2016.
Peraturan Menteri Kesehatan Republik Indonesia (PMKRI)
no 27 Tahun 2014 Tentang Petunjuk Teknis Sistem
Indonesian Case Base Groups (INA-CBGs)
Peraturan Menteri Kesehatan Republik Indonesia (PMKRI)
no 28 Tahun 2014 Tentang Pedoman Pelaksanaan
Program Jaminan Kesehatan Nasional.
Peraturan Menteri Kesehatan Republik Indonesia (PMKRI)
no 64 Tahun 2016 Tentang Perubahan Atas Peraturan
Menteri Kesehatan Nomor 52 Tahun 2016 Tentang
Standar Tarif Pelayanan Kesehatan Dalam
Penyelenggaraan Program Jaminan Kesehatan.
Rahayuningrum IO, Tantomo D, Suryono A; Comparison
Between Hospital Inpatient Cost and INA-CBGs Tariff
of Inpatient Care in the National Health Insurance
Scheme in Solo, Boyolali and Karanganyar Districts,
Central Java. Journal of Health Policy and Management
1;2016.
Rumampuk MS, Perbandingan Perhitungan Harga Pokok
Produk Menggunakan Metode Activity Based Costing
dan Metode Konvensional Pada Usaha Peternakan
Ayam CV. Kharis di Kota Bitung, Jurnal EMBA 637
Vol.1 No.4; 2013.
Rusli NT, Analisis Biaya dan Faktor-Faktor Penentu
Inefisiensi Layanan Hemodialisis pada Pasien Gagal
Comparison the Unit Cost of Hemodialysis Service with Dialysis Service’s Tariff in INA CBGs Universal Health Coverage Programe
(JKN): Case Study Hemodialysis Clinic in Depok
133

Ginjal Kronik Rumah Sakit Rk Charitas Palembang
Tahun 2016. Jurnal ARSI;Juni 2017.
Sari RP, Perbandingan Biaya Riil dengan Tarif Paket INA-
CBGs dan Analisis Faktor yang Mempengaruhi Biaya
Rill pada Pasien Diabetes Melitus Rawat Inap
Jamkesmas di RSUP Dr Sardjito Yogyakarta, Jurnal
SPREAD, Volume 4 Nomor 1;April 2014.
ICVHE 2019 - The International Conference of Vocational Higher Education (ICVHE) “Empowering Human Capital Towards Sustainable
4.0 Industry”
134
