
The Complexity of Sharia and the Implementation of Islamic Ethics
in Establishing Sharia Standards for Hospital
Muhammad Maksum
1
, Siti Hanna
2
, M. Asrorunniam Sholeh
2
and Afidah Wahyuni
2
1
Departement of Islamic Economic Law, Syarif Hidayatullah State Islamic University, Ciputat, South Tangerang, Indonesia
2
Department of Comparative Law, Syarif Hidayatullah State Islamic University, Ciputat, South Tangerang, Indonesia
Keywords: Sharia, Islamic law, Hospital, standard, contract.
Abstract: Sharia standards have been implemented in many fields such as finance, tourism, hospital, and financial
technology. In the economic sense, the standards generally refer to the establishment of contract (akad) and
the involved party. However in reality, the implementation of Sharia standards for hospital is more complex
than that of economic sense. Aside from the contract, the standards also refer to the personnel, services,
medicine and food, and fund allocation and budgeting. The response for this system has been positive, marked
by the high demands for Sharia certification. This paper will contest the implementation of Sharia standards
for hospital against the standards implemented in banking system which has already been implemented. In
addition, it will also observe the support and direction of the regulation between the hospital and the banking
system in Indonesia. This comparison is crucial for the ongoing dynamics within the Muslim society to
implement the Sharia way of life in their everyday’s life.
1 INTRODUCTION
The development of Sharia-based industries and
companies continues to increase. If it previously took
place in the financial sector, it has lately penetrated
other industries and services such as tourism industry
and health services. In terms of Sharia-based health
services or Sharia hospitals, Indonesia is the first
country to initiate their standardization. For the first
time, the Sharia standard for the hospital was
launched by the Indonesian Islamic Health Effort
Council (Majelis Upaya Kesehatan Islam Seluruh
Indonesia/MUKISI) by the end of 2017. The National
Sharia Council (Dewan Syariah Nasional/DSN) of
the Indonesian Ulema Council even issued a fatwa
regulating the criteria that must be met by the
hospital. It’s Fatwa Number 107/DSN-MU/IX/2016
regarding the implementation guidelines for hospitals
based on the Sharia principles which were ratified on
1 October, 2016.
Besides MUKISI, several institutions
accommodating hospitals are also formed. At the
international level, for example, 2 institutions have
supervised Islamic hospitals. The institutions are the
Federation Islamic Medical Association (FIMA) and
the Islamic Hospital Consortium (IHC) meeting.
Although they supervise Islamic hospitals, it does not
mean that the Islamic hospitals implement the Sharia
certification. Practically, Islamic hospitals and Sharia
certified hospitals have differences. Countries that are
members of FIMA include America, Europe,
Pakistan and Malaysia. (Mukisi, 2018)
The first hospital to obtain Sharia certification is
Sultan Agung Hospital, a type B private hospital in
2017. The hospital is located in Semarang, Central
Java. Until August, 2018, the number of hospitals that
have received Sharia certification has been about 10
hospitals. This number will continue to grow,
considering there have currently been 24 hospitals
submitting the certification process. Further,
MUKISI has targeted 50 hospitals to certify by the
end of this year. (Mukisi, 2018) To support the
certification effort, the certification assessors is being
prepared through assessor training. The number of
assessors who have been certified as assessors is 15
people and 22 people will soon add up, which means
the total number of the assessors becomes 37 people.
(Mukisi, 2018)
Sharia hospitals must provide services that are
different from conventional hospitals. The religious
atmosphere, according to Samsudin Salim, is
considered to have a role to increase endurance and
accelerate hospitalization as hospitals combine
140
Maksum, M., Hanna, S., Sholeh, M. and Wahyuni, A.
The Complexity of Sharia and the Implementation of Islamic Ethics in Establishing Sharia Standards for Hospital.
DOI: 10.5220/0009919801400147
In Proceedings of the 1st International Conference on Recent Innovations (ICRI 2018), pages 140-147
ISBN: 978-989-758-458-9
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

medical and spiritual services. Here, the spiritual
service is free of charge and Non-Muslim patients are
entitled to get services in accordance with their
respective religion. (Mukisi, 2018) If compared to
Muslim minorities in non-Muslim areas, according to
Robert M. Marsh, minority communities will adapt to
the majority values especially if socialization is made
available to them. (Marsh, 2012)
There are two main aspects a hospital must
consider, quality improvement and patient safety.
Islam itself emphasizes the importance of these two
aspects, so that a doctor in Islam must be responsible
for his/her work. He/she is not negligent in carrying
out his/her duties. (al-Syafi’i, 1325H) In other words,
these two aspects must be the basis and indicators of
Sharia hospitals.
2 ISLAMIC HOSPITAL AND
SHARIA HOSPITAL
A hospital is a health service institution that organizes
individual health services in a comprehensive manner
and provides inpatient, outpatient and emergency
services. Here, hospitals that serve patients from all
backgrounds are called public hospitals. In the
meantime, the hospitals serving one field or one type
of disease are called special hospitals. The hospital
can be established by government, local government,
and private sectors.
Islamic hospitals have long been established. The
name of an Islamic hospital is not the same as a Sharia
hospital. The Islamic hospital, for example, refers to
ownership of the hospital and its affiliates. Islamic
labels are usually pinned or entitled to hospitals in
which the owners are Muslim or Islamic
organizations. It is also possible that the Islamic label
affiliates the hospitals to certain religious
organizations. Basically, the Islamic label does not
require certain requirements as it can be pinned by the
owner of the hospitals.
The Sharia label in a hospital is an award for
meeting certain standards. The hospital must go
through a certification process raging from
registration, the fulfillment of standards, observing
the fulfillment of assessment elements, and
certification decision by assessors. If all the stages are
completed by the hospital and the auditing assessors
finds it has met all standards, it will eventually be
granted Sharia certification. Thus, Islamic hospitals
are not necessarily Sharia hospitals and likewise.
3 THE STANDARDS OF SHARIA
HOSPITAL PLUS
Hospitals that will apply for Sharia certification must
first obtain accreditation from the Hospital
Accreditation Committee (Komite Akreditasi Rumah
Sakit/KARS). Accreditation here is also a
requirement for any hospitals that will open BPJS
services, submit operational permits and class
assignments and fulfill hospital obligations to avoid
lawsuits and improve quality and customer
satisfaction (patient safety). Article 40 of the Hospital
Law mentions “in an effort to improve the quality of
hospital services, accreditation must be carried out
periodically for at least once in 3 (three) years. That
means the hospitals have met the standards set by the
government. In other words, the Sharia hospital
certification is an additional standard. In practice, the
Sharia hospitals resemble accredited plus Sharia
certified hospitals, which indicates they meet the
accreditation and Sharia standards.
The accreditation standards are set in 15 chapters
of KARS accreditation and the Sharia standards
consist of 5 chapters. This means that Sharia hospitals
must meet 20 chapters of accreditation. To this end,
they have added values in service, management and
organization aspects. The latest hospital accreditation
standards have been in force since January 1, 2018.
These standards include five groups of assessment,
patient-oriented services, management, patient
safety, national programs, and integration of health
education in services. Each group includes several
accreditation targets. Service standards, for instance,
targets the access to hospitals and continuity of
services, patient and family rights, patient
assessments, patient care, anesthesia and surgical
services, pharmaceutical services and drug use, and
communication and education management. In
meantime, the management standards aims at
improving patient quality and safety, infection
prevention and control, hospital governance, facility
and safety management, staff competency and
authority, and information and medical record
management. Further, the target of patient safety
standards is to identify patients correctly, maintain
effective communication, and improve the safety of
drugs that must be alerted (high alert medications). In
addition, the standards ensure the correct surgical
location and procedures, conduct surgery for the right
patient, reduce risk infections related to health
services, and reduce the risk of patient injury due to
falling. The objectives of the national program
include reducing maternal and infant mortality,
reducing HIV/AIDS morbidity, decreasing TB
The Complexity of Sharia and the Implementation of Islamic Ethics in Establishing Sharia Standards for Hospital
141
efficacy rates, controlling antimicrobial resistance
and providing geriatric services. Overall, the total
standards for hospital accreditation from the five
groups of assessment are equal to 338 standards. Each
standard is assigned to several assessment elements.
These assessment elements are included in the sixteen
criteria. At last, the total number of assessment
elements is about 1353 assessment elements.
The standards for hospital accreditation from the
five assessment groups totaled 338 standards. Each
standard is derived in several assessment elements.
These assessment elements are included in sixteen
criteria. The total number of assessment elements is
1353 elements. The sixteen criteria are:
1. Patient safety target with 10 standards and 36
assessment elements.
2. Access to hospitals and service continuity with
23 standards and 100 elements.
3. Patient and family rights numbered 27 standards
with 100 assessment elements.
4. Patient assessment includes 39 standards and
163 assessment elements.
5. Patient care and service with 21 standards and
81 elements.
6. Anesthesia and surgery services cover 20
standards with 71 assessment elements.
7. Pharmaceutical and drug use services with 21
standards and 80 assessment elements.
8. Communication and education management
with 13 standards and 49 elements.
9. Quality improvement and patient safety with 19
standards and 80 assessment elements.
10. Infection prevention and control with standard
28 pieces and 107 elements.
11. Hospital governance with 28 standards and 127
assessment elements.
12. Facility and safety management with 24
standards and 105 assessment elements.
13. Staff competency and authority which includes
26 standards and 96 assessment elements.
14. Information management and medical records
with 21 standards and 77 elements.
15. The national program includes 12 standards
with 58 assessment elements.
16. Integration of health education in hospital
services with 6 standards and 23 assessment
elements.
If mapped out based on the functional groups, the
accreditation standards are categorized into
management, medical, and nursing targets. The
management targets, for example, consist of 118
standards, while the medical targets include 121
standards. In the meantime, the nursing targets cover
99 standards. The following is the complete data on
the number of standards and assessment elements for
each target.
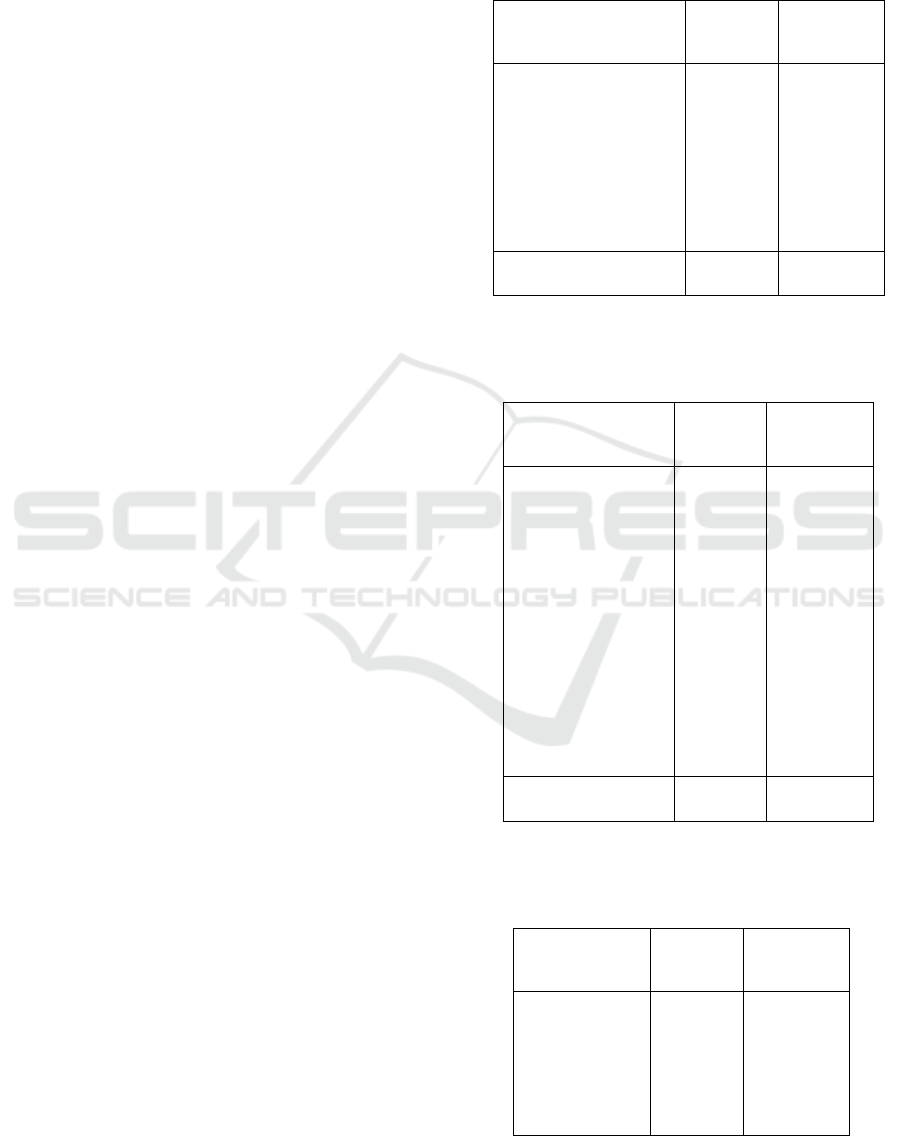
Table 1: Management standards.
Indicators No
Standards
No
Assessment
Element
Pharmaceutical and
drug use services
Quality improvement
and patient safety
Hospital governance
Facility and safety
management
Staff competency and
authority
21
19
28
24
26
80
80
127
105
96
Total 118 488
Source: Masyhudi, 2018.
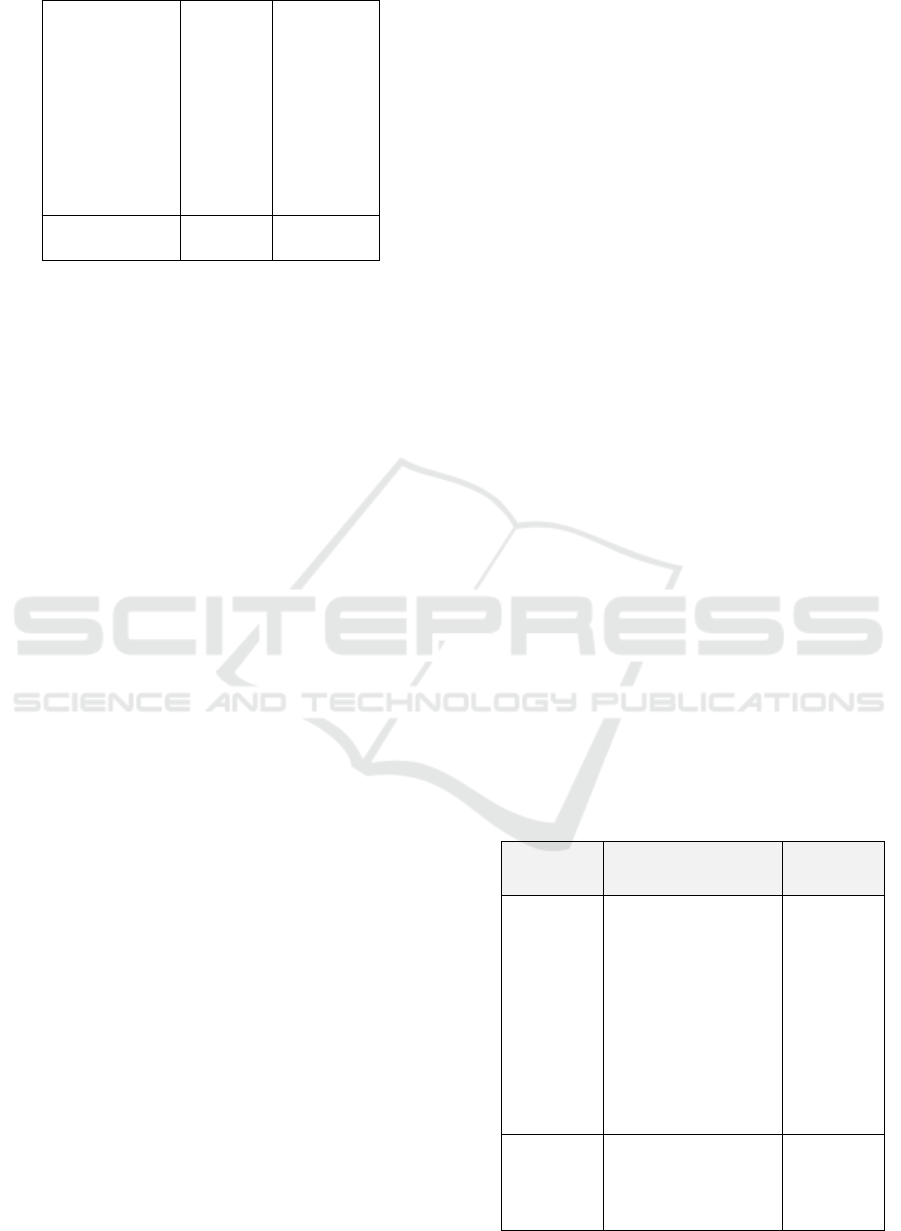
Table 2: Medical standards.
Indicators No
Standards
No
Assessment
Element
Access to hospitals
and service
continuity
Patient assessment
Patient care and
service
Anesthesia and
surgery services
The national
program
Integration of health
education in hospital
services
23
39
21
20
12
6
100
163
80
71
58
23
Total 121 496
Source: Masyhudi, 2018.
Table 3: Nursing Standards
Indicators No
Standards
No
Assessment
Element
Patient and
family rights
Communication
and education
management
27
13
28
10
100
49
107
36
ICRI 2018 - International Conference Recent Innovation
142
Infection
prevention and
control
Patient safety
target
Information
management
and medical
records
21 77
Total 121 496
Through some provisions in Islamic criminal law,
Islam itself seeks to protect the society from the
dangers of free sexual relationship or without
marriage bond considering it can lead to HIV/AIDS.
(Deuraseh, 2008) The Sharia standard for this type of
hospital attempts to combine substantive and
legalistic approaches. These two approaches,
according to Hegazy, are socio-economic and legal
approaches to see the development of Islamic finance.
(Hegazy, 2007) If it is associated with a hospital, the
combination of the two seeks to combine service and
legal aspects in the hospital.
4 FROM MAQÂSHID
AL-SYARÎ’AH TO STANDARDS
The Sharia hospital certification standards are derived
from the objectives of Sharia (maqâshid al-syarî'ah)
which become the goals of the Sharia existence and
lead to the interest for primary needs (dharuriyyat),
secondary needs (hâjiyat), or tertiary needs
(tahsîniyyat). (Ibn ‘Ashur, 2012) In details, the
objectives of Sharia focus on the five main objectives
(kulliyyat al-khams) including protection of religion
(hifzhu al-din), protection of soul (hifzhu al-nafs),
protection of offspring (hifzh al-nasl), protection of
wealth (hifzh al-mal), and protection of mind (hifzh
al-‘aql). Preserving and protecting religion, for
example, is done by fulfilling the five principles
(ijâbiyyah) and avoiding any acts that are contrary to
the five principles (‘adamiyyah). (al-Syatibi, 2006)
Therefore, a doctor who will be assigned must fulfill
three conditions; having patient approval, obtaining a
medical license from the authorized party, and
following the applicable provisions and code of
conducts. (Kassim)
Hifzh al-din (protection of religion) occupies the
highest and most important positions compared to
others considering it is the pillar of the life of society
and individuals in the world and the hereafter. (al-
Syatibi, 2006) Meanwhile, hifzh al-nafs aims at
nurturing the human soul in order to maintain their
existence on earth and create ease and comfort in their
life. (al-Zuhaili, 1998) Hifzh al-‘aql is intended to
protect the mind because human beings are noble
compared to other beings due to the existence of their
mind. Further, Hifzh al-nasl is to protect offspring
and therefore marriage is highly recommended and
adultery is forbidden. Lastly, Hifzh al-mal which
means protecting wealth is carried out by the
existence of a contract in the form of buying and
selling and ijarah. (al-Zuhaili, 1998) Some scholars,
such as Imam al-Qarafi, add one more type of
protection, hifz al-‘ird, which is the protection of self-
esteem. One more important thing to include in the
kulliyat al-khams is the protection of environment
(Hifzh al-Biah). This latter protection is essentially an
inherent obligation in human identity as the caliphs
on earth.
Basically, the standards and elements of hospital
assessment are derived from the objectives of the
sharia (maqâshid al-syarî'ah). In details, the
objectives of protecting religion (hifzh al-din) include
33 standards and 119 elements of assessment, the
objectives of protecting soul (hifzh al-nafs) contain 6
standards and 20 elements of assessment, and the
objectives of protecting mind (hifzh al-‘aql) cover 6
standards and 7 elements of assessment. In the
meantime, the objectives of protecting offspring
consist of 2 standards and 7 elements of assessment
and the assessment of protecting wealth (hifzh al-mal)
cover 4 standards and 14 elements of assessment. If
the sharia goals is correlated with the target of
management standards, then the results are as
follows:
Table 4 Sharia target and management standards.
Target Management
Standards
Indicators
protection
of religion
(hifz al-
din)
organizational
management
human capital
management
financial
management
marketing
management
facility management
quality management
28
14
5
8
8
7
protection
of soul
(hifz al-
nafs)
facility management 4
The Complexity of Sharia and the Implementation of Islamic Ethics in Establishing Sharia Standards for Hospital
143
Target Management
Standards
Indicators
protection
of mind
(hifz al-
‘aql)
human capital
management
6
protection
of
offspring
(hifz al-
nasl)
- -
protection
of wealth
(hifz al-
mal)
financial
management
12
Total 92
Source: Masyhudi, 2018
If the sharia goals is correlated with the target of
management standards, then the results are as
follows:
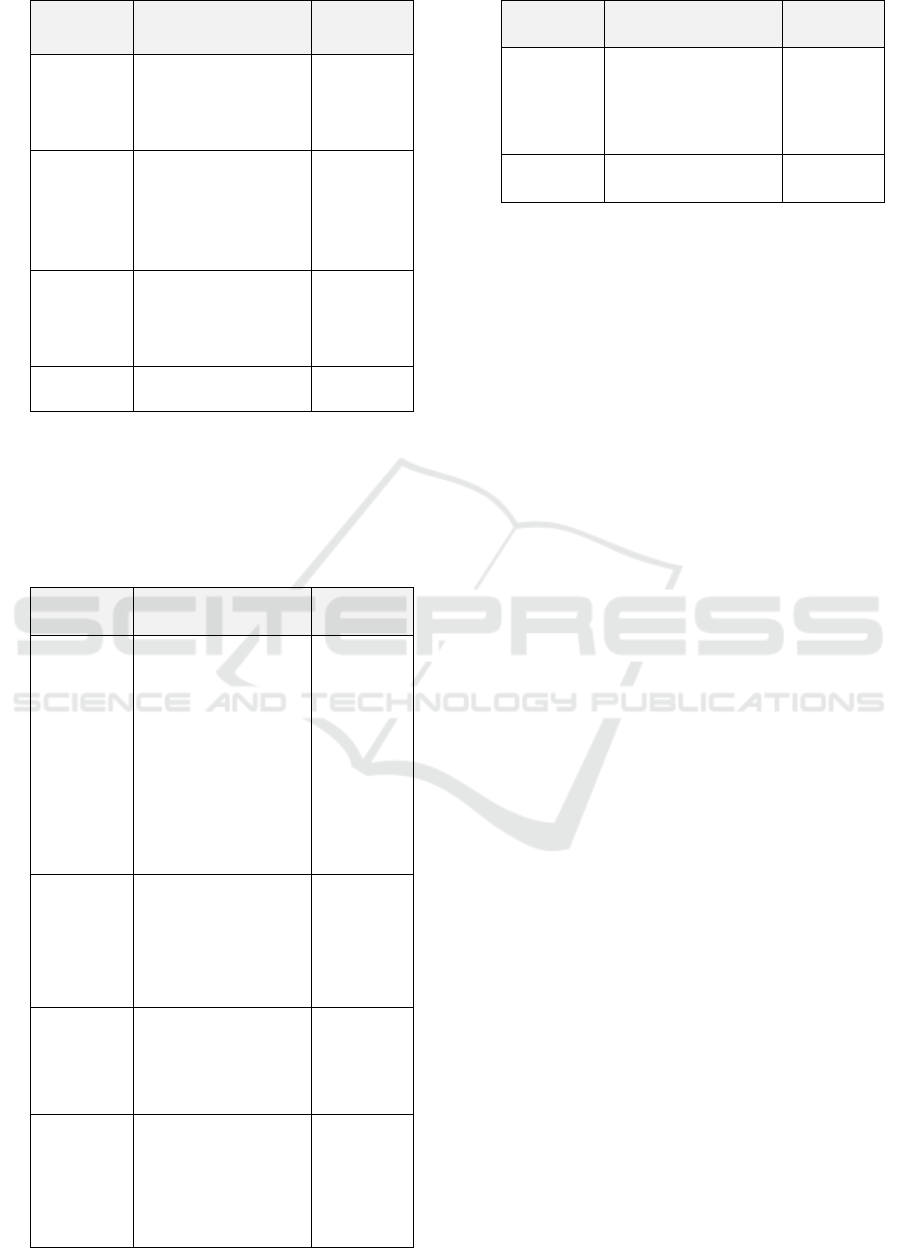
Table 5 Sharia target and service standards
Target Services Standards Indicators
protection
of
religion
(hifz al-
din)
service access and
continuity
patient assessment
patient services
medicine services
spiritual guidance
and services
patient and family
education
6
3
19
9
8
4
protection
of soul
(hifz al-
nafs)
infection
prevention and
control
spiritual guidance
and services
2
10
protection
of mind
(hifz al-
‘aql)
patient assessment
patient and family
education
3
8
protection
of
offspring
(hifz al-
nasl)
patient services 7
Target Services Standards Indicators
protection
of wealth
(hifz al-
mal)
patient services 2
Total 83
Source: Masyhudi, 2018
The Sharia standards for hospitals are actually
divided into thirteen (13) groups of standards. These
groups of standards are categorized into management
and service standards. Six (6) standards are included
in the management standard and seven (7) standards
are in the service standard. Here, the group of Sharia
management standards covers organizational
management, human capital management, financial
management, marketing management, facility
management, and quality management. Further, the
group of Sharia Service standards include service
access and continuity, patient assessment, patient
services, Sharia medicine services, spiritual guidance
and services, patient and family education, and
infection prevention and control.
Each group of the above standards has standard
details that differ from one to another. In the same
way, the elements of assessment for each standard are
also different. The total number of Sharia standards is
51 standards and the number of elements of
assessment is 173 elements. See the following table
for the details.
The standard shows the complexity of indicators
that must be met by hospitals. If, for example, Islamic
finance focuses on the prohibition of usury, obscurity
(jahalah), uncertainty (gharar), and prevents the
prohibited, then all Islamic provisions are applied in
Sharia hospitals, including other standards. If Foster
calls Islamic financial law an urgent need, the Sharia
hospitals also require more complex Sharia
provisions. (Foster, 2007) It cannot be solely included
in the classification of Islamic financial law, but there
has to be a separate classification.
5 THE TRANSFORMATION OF
FATWA TO SHARIA
STANDARDS FOR HOSPITAL
The standards set by MUKISI have extended from the
Sharia provisions stipulated in the DSN-MUI fatwa.
The Fatwa Number 107/DSN-MUI/X/2016 on the
ICRI 2018 - International Conference Recent Innovation
144

Implementation Guidelines for Sharia Hospital
stipulates four provisions that must be complied by
Sharia hospitals; first, the provision associated with
contract and personnel/institution in and outside the
hospital; second, the provision related to services;
third, the provision related to the Use of Medicines,
Food, Beverages, Cosmetics, and Goods; and fourth,
the provision associated with Hospital Allocation,
Use and Development Fund. Here, the fatwa has
become a legal source to determine the Sharia
hospital standards. (Amin, 2014) This condition also
shows the position of fatwa (including the position of
Muslim scholars) which play contribution in
responding to the needs of the society although such
contribution is not really significant compared to
Malaysia, considering the Malaysian legislation
places the position of scholars and fatwas in a strong
position. (Saat, 2012)
One of the Sharia principles emphasized in
hospital services is a contract or work relationship
between the parties involved in the management and
service of the hospital. As a result, the character of
Sharia in various muamalah activities centers on the
compliance of Sharia contracts stipulated by fatwas
that have a tendency to legal aspects although, in the
context of sharia hospitals, the contract does not
become the dominant standard. (El-Gamal, 2006)
The contracts applied in hospitals include buying
and selling and ijarah contracts. Buying and selling
contract, for instance, is used between hospitals and
pharmaceutical companies to purchase medicines. In
addition, it is also used to purchase nutritious food
ingredients by hospitals from the food service
providers. In the meantime, the ijarah contract can be
applied in many places and agreements; work
agreement between hospitals and permanent doctors,
permanent employees, and temporary employees.
Other employees involved in the hospitals can also be
involved in ijarah contract such as laboratory service
officers and supporting officers such as cleaning
staffs and security officers. Similarly, the ijarah
contract can also be used for cooperation between
hospitals and medical device providers for leasing
medical devices. Here, a contract on mobile oxygen
refilling is considered as ijarah contract between
hospitals and oxygen provider companies. (Lathif,
2018)
The contract regulated in the fatwa involves the
cooperation between hospitals and medical
personnel, patients, Medical Device Suppliers and
Laboratory Equipment Suppliers, and Drug
Suppliers. The contract applied between hospitals and
medical personnel and patients is a lease contract (al-
ijarah). In the meantime, the contract between the
hospitals and medical device suppliers is considered
as a lease contract (al-ijarah) and a lease with a
purchase option (al-ijarah al-muntahiya bi al-tamlik),
a sale and purchase contract (al-bay’), and a contract
with musyarakah mutanaqishah or mudharabah
agreement. (DSN, 2018) Hospitals and individuals in
the hospitals can become legal subjects with natural
and legal personality principles. (Zahraa,) In Islam,
the position of the parties determines their rights and
obligations. In the case of doctors, Islam requires a
doctor who practices to have expertise in his/her field.
If he/she is negligent due to his/her
unprofessionalism, he/she will be responsible for the
loss suffered by the patient and the patient’s family.
(Ibn Qayyim, 1397H)
The standard of the contract is stated only in one
standard, standard number 1.1.9 with five elements of
assessment. Four assessments are stated in the DSN
fatwa and one more element of assessment is added
by MUKISI. This additional element is a contract
between hospitals and financial, insurance, education,
and social institutions and other institutions. (Mukisi,
2017)
Regarding the provisions associated with hospital
financial management, the DSN fatwa sets several
rules. First, the hospital is obliged to cooperate with
Islamic Financial Institutions, such as banks,
insurance, financing institutions, guarantee
institutions, and pension fund; second, the
management of the fund portfolio and other types of
assets is carried out based on the Sharia principles;
third, the prohibition of working with institutions or
business activities contradicting to Sharia principles;
and fourth, the guidelines to manage zakat fund,
infaq, alms and endowments.
All provisions in the fatwa are adopted in the
standards for Sharia hospitals set by MUKISI. Here,
the Sharia standard even provides additional
standards, financial governance based on Sharia
accounting, the obligation to pay zakat for hospital
institutions and employees, policies and management
mechanisms for patients who cannot afford to pay,
and guidelines for billing calculations. (Mukisi, 2017)
Three important aspects of the expansion of
Sharia standards include the application of Sharia
accounting, tendency for patients who can’t afford to
pay, and billing errors. The Sharia accounting
standards set by DESAS, for example, are different
from the ones in conventional accounting.
Nevertheless, there is no specific Sharia accounting
standard for hospitals. The current accounting
standards applied to Islamic finance and socio-
religious finance is waqf and zakat. Further, the
Sharia standards related to patients who can’t afford
The Complexity of Sharia and the Implementation of Islamic Ethics in Establishing Sharia Standards for Hospital
145

to pay is an Islamic standard. This is very crucial to
give assistance and lenience to people who are unable
to complete the payment. In the case of debt, people
who are clearly unable to pay shall be released from
their debt. A hadith narrated by Ibn Abbas mentions.
When the Prophet asked to expel the Banu Nadhir,
several of them came and said: “O Prophet, you have
asked to expel us while we owe some money and we
haven’t paid yet". He then replied: “Give remission
and bill it faster". As for the billing errors, the Sharia
principle emphasizes the importance of earning
money in a lawful and correct way. The billing errors
result in unauthorized payments and bring bad assets.
In addition, they can also harm the hospital or patient.
In practice, if the billing is greater than what the
patient has to pay, then the excess billing is the
patient’s right and must be returned to him/her. If the
billing is less than what is supposed to be paid by the
patient, then the hospital has the right to collect the
shortage from the patient or to explain it. Such action
is based on the principles of fiqh, ibra’, which is to
release rights.
Other provisions regulated in the fatwas are
associated with drugs. Medicines, food, drinks,
cosmetics, and goods that will be used in hospitals
must be halal and obtain halal certification from the
Indonesian Ulema Council (MUI). If, for example, a
halal certified-drug is not found, then using drugs that
do not contain prohibited elements is an option. Here,
the drugs that contain unclean elements can only be
used in an emergency and informed consent
procedures have been carried out. (DSN, 2016) The
drug service standard set by MUKISI do not regulate
the stages of drug use in details, from halal
certification, absence from illicit goods, and the use
of drugs containing illicit ingredients in an emergency
situation. The standard only contains the commitment
of the hospital to provide drug formulas that do not
contain haram elements. However, it extends the
criteria related to Islamic messages written on labels
or drug packages given to patients and the religious
messages when giving the drugs to the patients.
(Mukisi, 2017)
Regarding the service standard, when the fatwa
and Sharia criteria set by the MUKISI are compared,
the MUKISI’s sharia standard undergoes a very deep
expansion. The terms of service in the fatwa include
the obligation of the parties to complete their rights
and obligations, services based on the standard
Clinical Practice Guideline, clinical pathways and/or
applicable service standards, prioritizing
humanitarian aspects regardless of race, ethnicity,
and religion, committed to trustworthy, polite and
friendly, transparent and qualified. In addition, the
terms also cover the application of the principles of
justice, and fairness in costing, providing spiritual
services and consultations, the obligation of patients
and the person in charge of the patients to obey the
rules and have good character, avoid immoral acts,
risywah, zhulm and any acts that contradict to the
Sharia, and always conform the Sharia provisions
stipulated by the MUI. At last, the guidelines for
Islamic worship procedures and hygiene standards
are also made available. (DSN, 2016) All provisions
in the fatwa have been accommodated in the sharia
standards for hospital services. Such provisions are
found in the Sharia standards of patient assessment,
spiritual service and guidance standard, and patient
and family education standard. In the sameway, the
Sharia service standard also adds transportation
standard which is equipped with Islamic audio or
video, standard of aurat supervision and patient
service by gender and regulation to separate men and
women who are not muhrim (an unmarriageable kin
with whom marriage or sexual intercourse would be
considered haram). Rukyah service, reproductive and
child health according to sharia, service for patient
who pass away, waste management, and the
procurement of water in accordance with the
provisions of Sharia are also provided. In addition,
the hospital must provide a library that contains
Islamic literatures and education and give Islamic
health advice to visitors. (Mukisi, 2017) In Islam,
professionalism is also regulated. An incompetent
doctor must be responsible for the health measures
he/she conducts. However, if the doctor is competent
and carries out his/her duties properly and does not
contradict the Sharia, then he/she, for example,
causes something for the patient, he does not have to
be responsible. (Kassim, 2007)
The transformation of the fatwa in the Sharia
standard proves the existence of a development in the
Islamic legal system. Fatwa, referring to the term
used by Wael B. Hallaq, has acted as a legal discourse
and social instrument. (Hallaq, 1994) This standard
also emphasizes that the fatwa is a product which is
relevant to the needs of society and it is not a legal
speculation from the legal experts (muftis). (Hallaq,
1994)
6 CONCLUSION
The Sharia standards for hospitals are related to
patient and safety services instead of contract. Many
standards and elements of assessment that must be
met by Sharia hospitals affect the complexity of
implementing these standards. Here, the hospitals
ICRI 2018 - International Conference Recent Innovation
146

undergo a transformation and expansion for the
standards as set in the fatwa of the National Sharia
Council of the Indonesian Ulema Council. Basically,
the Sharia standards are derived from the objectives
of Sharia (maqâshid al-syarî'ah) which include
protection of religion, protection of soul, protection
of offspring, protection of wealth, and protection of
mind. At last, hospitals that have obtained Sharia
certification are in turn entitled to hospitals plus as
they are accredited according to the law and are also
certified based on the Sharia principles.
REFERENCES
Admin Mukisi, “Mukisi Siap Berbagi Cerita tentang
Rumah Sakit Syariah di Forum Internasional »,
accessed on August 12, 2018 from
https://mukisi.com/898/mukisi-siap-berbagi-cerita-
tentang-rs-syariah-di-forum-internasional/.
Admin Mukisi, “Latih Asesor, Mukisi Yakin Lahirkan 50
Rumah Sakit Tersertifikasi Syariah”, accessed on
August 12, 2018 from https://mukisi.com/886/latih-
asesor-untuk-lahirkan-50-rs-tersertifikasi-syariah-di-
2018/.
Admin Mukisi, “Latih Asesor, Mukisi Yakin Lahirkan 50
Rumah Sakit Tersertifikasi Syariah”, accessed on
August 12, 2018 from https://mukisi.com/886/latih-
asesor-untuk-lahirkan-50-rs-tersertifikasi-syariah-di-
2018/.
Admin Mukisi, “Seperti Ini Suasana Religius di Rumah
Sakit Syariah », accessed on August 12, 2018 from
https://mukisi.com/906/seperti-ini-suasana-religius-di-
rs-syariah/.
Al-Alim, Yusuf Hamid. al-Maqâshid al-‘Ammah li al-
Syarî’ah al-Islâmiyyah.
Al-Syatibi, 2006. al-Muwâfaqat fi Ushûl al-Ahkâm, Dar al-
Hadits. Cairo.
Al-Zuhaili, Wahbah, 1998. Ushûl al-Fiqh al-Islâmy, Dar al-
Fikr. Damaskus, series 2.
Amin, Ma’ruf, 2014. “Perkembangan Fatwa dan Peraturan
Perundang-undangan di Bidang Hukum Ekonomi di
Indonesia”, a paper presented in UIN National Seminar
on September 9, 2014.
Deuraseh, Nurdeen, 2008. “Protection against STDs: An
Islamic Criminal Law Approach”, Arab Law Quarterly
22.
El-Gamal, Mahmod A., 2006. Islamic Finance, Law,
Economics, and Practice, Cambridge University Press.
Cambridge.
Fatwa Number NO: 107/DSN-MUI/IX/2016 regarding the
implementation guidelines for hospitals based on the
Sharia principles which were ratified on 1 October,
2016.
Foster, Nicholas H. D., 2007. “Islamic Finance Law as an
Emergent Legal System”, Arab Law Quarterly 21.
Hallaq, Wael B, 1994. “From Fatwas to Furu’: Growth and
Change in Islamic Substantive Law”, Journal of Islamic
Law dan Society, Leiden.
Hegazy, Walid S., 2007. “Contemporary Islamic Finance:
From Socioeconomic Idealism to Pure Legalism”,
Chicago Journal of International Law, Vol. 7, 2.
Ibnu ‘Ashur, 2012. Maqâsid al-Syarî’ah al-Islâmiyyah, Dar
al-Salam. Cairo.
Ibn Qayyim, 1397H. a’lam al-Muwaqqi’in, Dar al-Fikr,
Beirut.
Imam al-Syâfi’i, 1325H. Kitâb al-Umm, Matba’ah al-
Kubra, Cairo, 6
th
edition.
Kassim, Puteri Nemie Jahn, 2007. “Medical Negligence In
Islamic Law”, Arab Law Quarterly 20, 4.
Lathif, Ah. Azharuddin, 2018. “Akad-akad Syariah dan
Implementasinya di Rumah Sakit”, dalam Modul
Pelatihan Asesor Sertifikasi Rumah Sakit Syariah, DSN
Institut, Jakarta.
Marsh, Robert M., 2012. “Muslim Values in Islamic and
Non-Islamic Societies”, Comparative Sociology 11.
Masyhudi, 2018. “Pengantar Manajemen Rumah Sakit”, in
Modul Pelatihan Asesor Sertifikasi Rumah Sakit
Syariah, DSN Institut. Jakarta.
Mukisi, 2017. Standar Rumah Sakit Syariah, Mukisi.
Jakarta.
Saat, Norshahril, 2012. “Islamising Malayness: Ulama
discourse and authority in contemporary Malaysia”,
Contemporary Islam, 6.
Zahraa, Mahdi. “Legal Personality in Islamic Law”, Arab
Law Quarterly.
The Complexity of Sharia and the Implementation of Islamic Ethics in Establishing Sharia Standards for Hospital
147
