
Anxiety Level Differences on Light Smokers and Heavy Smokers in
Tegal Sari Mandala II and III Villages
Nanda Sari Nuralita
1*
Cut Mourisa
1
1
Department of Psychiatry, Faculty of Medicine, University of Muhammadiyah Sumatera Utara, Medan, Indonesia
Keywords: Anxiety level, Smokers.
Abstract: Smoking is one cause of death in the United States. Almost a quarter of the population smokes, and this
habit has been associated with about 430,000 deaths per year. Psychiatric disorders are 2-3 times more
common among smokers than non-smokers or ex-smokers. The prevalence of smoking in patients with
anxiety is 17% to 55%. By behavior, the stimulant effect of nicotine results in increased attention, time to
react, learning and problem-solving skills. The aim of this study is to examine the relationship between light
and heavy smoking habit and anxiety level with citizens in Tegal Sari Mandala II and III village, Medan.
This study is categorical analytic study with cross sectional method to see the relation between smoker and
anxiety level to citizen in Tegal Sari Mandala 2 and 3 village with 180 subjects in this study and will be
analyze by Chi-Square. The level of smoking habit will be asked during interviews and the anxiety level
will be examined by Hamilton Anxiety Rating Scale (HARS). In this study it was found that the greatest
possible level of anxiety/anxiety in both light smokers and heavy smokers was the same, i.e. moderate
anxiety but it can be ascertained that in heavy smokers it is less likely to experience mild anxiety (p <0.001).
1 INTRODUCTION
Smoking is one cause of death in the United States.
Almost a quarter of the population smokes, and this
habit has been associated with about 430,000 deaths
per year. Smoking is associated with asthma, chronic
bronchitis, lung cancer, coronary heart disease, and
emphysema. Although about 35% of smokers try to
quit smoking each year, less than 5% are successful.
The majority of researchers agree that one of the
major obstacles to success in quitting smoking is the
nicotine withdrawal syndrome (Morrell HE, 2006).
According to Morissette et al., 2007, the
prevalence of smoking in patients with anxiety is
17% to 55%. Hughes et al., 1986 found that 47% of
psychiatric patients treated with anxiety disorders
had a smoking habit. Himle et al., 1988 went on to
study Hughes, also observed smoking comorbidities
against more specific anxiety disorders. They
encountered simple phobias, 47%; social phobia,
27%; agoraphobia, 57%; panic disorder, 47%;
general anxiety, 29%, and obsessive compulsive
disorder, 9% who smoked. Himle also suggests that
smoking levels may differ between types of anxiety
disorders. Studies conducted by Johnson et al., 2000
show that heavy smokers (more than 20 cigarettes /
day) are associated with increased risk of anxiety
disorders, panic disorders, and agoraphobia
disorders during adulthood. The invention is also
consistent with previous findings that smoking
increases the risk of anxiety disorders.
Smoking prevalence, particularly nicotine
dependence is 2-3 times among patients with
anxiety, attention-deficit, mood, substance use, and
other psychiatric disorders. Psychiatric disorders are
2-3 times more common among smokers than non-
smokers or ex-smokers. By behavior, the stimulant
effect of nicotine results in increased attention, time
to react, learning and problem-solving skills.
Nuralita, N. and Mourisa, C.
Anxiety Level Differences on Light Smokers and Heavy Smokers in Tegal Sari Mandala II and III Villages.
DOI: 10.5220/0008791802710275
In Proceedings of the 2nd Syiah Kuala International Conference on Medicine and Health Sciences (SKIC-MHS 2018), pages 271-275
ISBN: 978-989-758-438-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
271

Tobacco users also report that smoking can reduce
depressive feelings, elevate mood and reduce tension
(Huges JR, 2009 and Sadock BJ, 2007). Nicotine has
a complex structure. The effects of nicotine on the
central nervous system are also widespread. The
central nervous system associated with nicotine will
result in changes in the neuronal receptor nicotinic
acetylcholine (nAChRs). These receptors can be
found throughout the brain area and when there is
stimulation, there are releases of neurotransmitters
such as dopamine, norepinephrine, vasopressin,
glutamate, serotonin, gamma aminobutyric acid
(GABA), and other neurotransmitters. Increased
concentrations of nAChRs receptors are found in the
mesolimbic system of dopamine and locus ceruleus
(Kamluddin A, 2011).
Nicotinic receptors in cognitive function,
are strongly associated with pleasure and reward
systems. Nicotine work on nAChRs will modulate
the amount of stress hormones, monoaminergic
transmission and neurotransmitters in the brain that
will improve memory and affect the level of anxiety
and depression in the normal brain. In addition to
nicotine, cigarette smoke contains monoamine
oxidase inhibitors (MAOI); an antidepressant, so
that the destruction of some neurotransmitters such
as dopamine, norepinephrine and serotonin will be
reduced. The release of serotonin, corticosteroids
and endorphins due to nicotine, can reduce fatigue
and improve the efficiency of the brain's cognitive
processes.
Because of these effects, nicotine has a
sedative effect that decreases anxiety (Kamluddin A,
2011). The aim of this study is to examine the
relationship between light and heavy smoking habit
with anxiety. The hypothesis of this study is there is
a relationship between light and heaving smoking
habit with anxiety in Tegal Sari Mandala II and III
Village Medan.
2 METHOD
This study is categorical analytic study with cross
sectional method to see the relationship between
smoker and anxiety level to citizen in Tegal Sari
Mandala 2 and 3 village. Population Study: residents
in Tegal Sari Mandala 2 and 3 villages.
Inclusion criteria: citizens registered in Tegal Sari
Mandala 2 and 3 , have a smoking history for 1 year,
men aged 20-40 years, Cooperative and willing to
participate in study. Exclusion criteria: have a
history of substance abuse other than nicotine, have
a history of general medical disorders, have a history
of psychiatric disorders.
The sample size is measured using the formula:
n1= n2= Z∝ 2PQ + Z𝛽 P1Q1 + P2Q2
2
P1 – P2
Using the formula above we get the sample of 90
people for each group. The total sample size is 180
people. This study activity is carried out in several
stages of preparation phase, implementation and
preparation of study result report. The step that has
been passed in this study is preparation and early
stage of study implementation. At the preparatory
stage, the activity is a literature study of theories that
support the study (study journal). Furthermore, the
management and permission application to conduct
study from the Medical Ethics and Study Committee
(KEPK) Faculty of Medicine, University of
Muhammadiyah Sumatera Utara.
Approval is obtained after 2 weeks submission.
The outcome of the preparatory phase is the draft
study work plan. After getting approval, the study is
continued to the stage of study implementation.
Activities undertaken by conducting study according
to draft work that has been prepared together by the
study team from the previous stage. Implementation
of the study begins with requesting permission in
advance with the Village Heads in Tegal Sari
Mandala II and III to collect the residents and ask
questions to fill out the questionnaire after first
getting information about the study and the purpose
of the study.
The residents of Tegal Sari Mandala II and III
Urban Villages meeting the inclusion criteria are
given explanation of the study and for the willing
citizens who will be the subjects of the study, are
required to complete the consent form. After
completing the consent form, the subject is
requested to sign the consent form. Then given the
form data, and given an explanation of its usefulness
SKIC-MHS 2018 - The 2nd Syiah Kuala International Conference on Medicine and Health Sciences
272
and how to fill it. After that the subject in the
interview for charging of Hamilton Anxiety Rating
Scale (HARS). After filling HARS done total sum of
HARS score, and performed data processing.
Implementation phase of the study until now
completed at the stage of data collection, while the
results of the study will be analyze by Chi-Square.
3 RESULT
Table 1: Distribution of sample demographic data
Demographic
data
n
%
Gender
Men
180
100.0
Smoking level
Mild
90
50.0
Severe
90
50.0
Age
20-29 years
40
22.2
30-39 years
63
35.0
≤40 years
77
42.8
Education
Elementary
18
10.0
Junior high
47
26.1
High school
60
33.3
University
55
30.6
Occupation
Employed
133
73.9
Unemployed
47
26.1
The table above shows that there were 180 male
samples, with light smokers as many as 90 people
(50.0%) and heavy smokers as many as 90 people
(50.0%), age range 20-29 years as many as 40
people (22.2 %), sample with age range 30-39 year
counted 63 people (35,0), and 40 ≤ year counted 77
person (42,8%). Based on the level of education, the
sample with the level of primary education found as
many as 18 people (10.0%), junior high school
education level of 47 people (26.1%), high school
education level of 60 people (33.3%), and college
level as many as 55 people (30.6%). Based on work,
the sample worked more with the number of 133
people (73.9%) and the non-working 47 people
(26.1%).
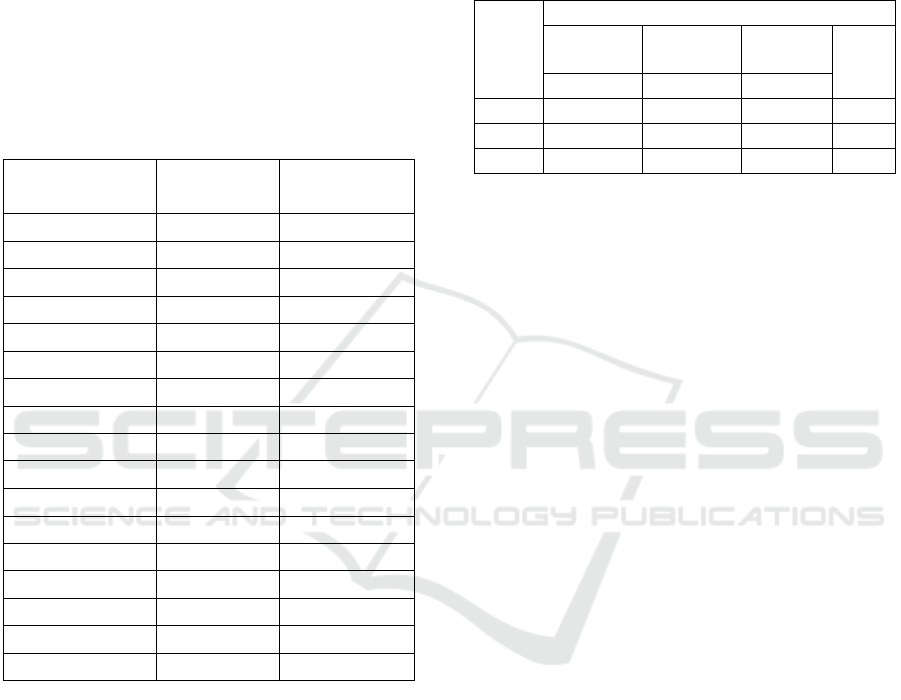
Table 2: Relationship of Smoking Behavior with
Anxiety Level with villagers on Tegal Sari Mandala
II and III.
Smokin
g habit
level
Anxiety level
Mild
anxiety
Moderate
anxiety
Severe
anxiety
P
value
n %
n %
n %
Light
60 66.7
20 22.2
10 11.7
0.001
Heavy
0 0
55 61.1
35 38.9
Total
60 33.3
75 41.7
45 25.0
The table above shows that there are 60 people
(66,7%) of light smoker with mild anxiety. There are
20 people (22,2%), heavy anxiety is 10 people
(11,1%). In the subject of heavy smokers
experiencing anxiety was found as many as 55
people (61.1%) and as many as 35 people who
experienced severe anxiety (38.9%). The p value
shows 0.001 (p<0.05) which means there is a
significant correlation between smoking behavior
and anxiety level with villagers on Tegal Sari
Mandala II and III.
4 DISCUSSION
The study of "anxiety level differences in
light smokers and heavy smokers" is an unpaired
categorical analytical study with cross sectional
methods. The purpose of this study was to determine
the difference of anxiety level in light smokers and
heavy smokers in Tegal Sari Mandala 2 and 3
villages. In this study it was found that the greatest
possible level of anxiety/anxiety in both light
smokers and heavy smokers was the same, i.e.
moderate anxiety but it can be ascertained that in
heavy smokers it is less likely to experience mild
anxiety (p <0.001).
This study is in accordance with a study conducted
Byeon in 2015 in South Korea that smoking has a
significant relationship with anxiety. Smokers have
an anxiety tendency of 1.5 times (OR = 1.49, 95%
CI [1,14-1,96]) greater than non-smokers (p <0.05)
and adolescents who smoke more than 5 cigarettes
Anxiety Level Differences on Light Smokers and Heavy Smokers in Tegal Sari Mandala II and III Villages
273

day 1.5 times (OR = 1.49, 95% CI [1.07-2.08]) are
more likely to have anxiety (p <0.05).
This study, however, does not match the
study by Khademalhosseini in 2015 in Iran against
1020 high school adolescents where there is no
significant relationship between smokers and
anxiety. In addition, the findings of Lee et al in 2017
in the United States with interesting findings suggest
that mild smokers (less than 1-5 cigarettes a day) but
very depressed/depressed have a 5.8 times greater
risk of having anxiety disorders Thorough compared
to individuals who do not smoke and have mild
symptoms of depression. Also, multiple stroke but
highly depressed smokers have a 3.8 times greater
risk for having an overall anxiety disorder,
compared to people who smoked less than half a
pack a day and had low symptoms of depression.
Symptoms of depression seem to have a stronger
relationship with a complete anxiety disorder than
smoking.
Recent conclusions in terms of cigarette linkage
with anxiety can be seen from a literature study by
Fluharty et al in 2017 in the UK where from 148
studies categorized as: onset of smoking, smoking
status, heavy smoking, tobacco dependence and
smoking trajectory. The results for each category
vary substantially, with positive associative evidence
in both directions (smoking with later mental health
effects and mental health leads to later smoking
behavior). Overall, nearly half of the studies
reported that baseline anxiety was associated with
several types of smoking behavior, while more than
one-third found evidence that smoking exposure was
associated with anxiety that would subsequently
emerge. However, there are several studies that
directly support the two-way model of smoking and
anxiety can occur mutually. While this incidence
could be explained by the fact that the impact given
to smokers has the effect of being given
psychostimulants. Acute nicotine exposure, whether
obtained by smoking or intravenous infusion of
nicotine, has an effect on elevating the amount of
cortisol in the human body and animals. Long-term
smoking can cause persistent dysregulation of
hormonal regulation. Hypertensive patients also
experience increased sympathetic tone, where can
increase the intensity of anxiety symptoms in
patients.
REFERENCES
Aditama TY. Final Report Global Youth Tobacco
Survey Jakarta- Bekasi- Medan-Indonesia. 2003-
2004: 17- 18.
Badan penelitian dan Pengembangan Kesehatan
Kementrian Kesehatan RI. Penggunaan
Tembakau. Riset Kesehatan Dasar (Riskesdas).
2010; 399.
Baron, J. A., Comi, R. J., Cryns, V., Brinck-Johnsen,
T., & Mercer, N. G. 2017. The effect of cigarette
smoking on adrenal cortical hormones. Journal
of Pharmacology and Experimental
Therapeutics, 272, 151–155
Caggiula, A. R., Epstein, L. H., Antelman, S. M.,
Saylor, S. S., Perkins, K. A., et al. 2016.
Conditioned tolerance to the anorectic and
corticosterone-elevating effects of nicotine.
Pharmacology, Biochemistry and Behavior, 40,
53–59.
Hughes JR. Tobacco withdrawal in self-quitters.
Journal of Consulting and Clinical Psychology.
1992; 60(5): 689–697.
Hughes JR. Pharmacotherapy for smoking cessation:
Unvalidated assumptions, anomalies, and
suggestions for future study. Journal of
Consulting and Clinical Psychology. 1993;
61(5): 751–760.
Hughes JR, Hatsukami DK, Mitchell JE, &
Dahlgren LA. Prevalence of smoking among
psychiatric outpatients. American Journal of
Psychiatry. 1986; 143: 993–997.
Johnson JG. Associaion cigarette smoking and
anxiety disorders during andolescense and early
adulthood. The Journal American Medical
Association. 2000; 284: 2348-2351.
Kamaludin A. Pemantauan dopamin transporter
sebagai biomarker dalam keberhasilan berhenti
merokok. Jakarta: Indonesian Psychiatric
Quarterly 2011, no. 4: p. 77- 89.
McDowell I. Measuring Health A Guide to Rating
Scales and Questionnaires 3rd ed. New York:
Oxford University Press. 2006, p. 273- 93.
SKIC-MHS 2018 - The 2nd Syiah Kuala International Conference on Medicine and Health Sciences
274

Morisette SB, Tull MT, Gulliver SB, Kamholz BW,
Zimering RT. Anxiety, anxiety disorder, tobacco
use, and nicotine: a critical review of
interrelationship. Psychological Bulletin. 2007;
133 (2): 245-272.
Morrell HE, Cohen LM. Cigarette Smoking,
Anxiety, and Depression. Journal of
Psychopathology and Behavioral Assessment,.
2006; 28 (4): 283-296
Moylan S, Jacka FN, Pasco JA, Berk M. How
cigarette smoking may increase the risk of
anxiety symptoms and anxiety disorders: a
critical review of biological pathways. Brain and
Behavior. 2013; 3(3): 302–326.
Sadock BJ, Sadock VA. Kaplan & Sadock’s
Synopsis of Psychiatry Behavioral Sciences/
Clinical Psychiatry. 10th ed. Philadelphia:
Lippincott Williams & Wilkins; 2007.
Senol Y, Donmez L, Turkay M, Aktekin M. The
incidence of smoking and risk factors for
smoking initiation in medical faculty students:
cohort study. BMC Public Health. 2006; 6:128.
Sitepoe M. Kekhususan rokok Indonesia. Jakarta:
PT. Gramedia Widiasarana Indonesia; 2000: p.
5- 22.
World Health Organization. Tobacco: deadly in any
form or disguise. 2006: p. 7- 31.
Anxiety Level Differences on Light Smokers and Heavy Smokers in Tegal Sari Mandala II and III Villages
275
