
The Relationship between Nutritional Status and Central Obesity with
Low Density Lipoprotein (Ldl) Cholesterol Level in Coronary Heart
Disease Patients at Rsudza Banda Aceh
Egi Atika Handayani
1
, Husnah
2*
, Muhammad Ridwan
3
1)
M
edical
F
aculty, Universitas Syiah Kuala, Banda Aceh, Indonesia
2) Department of Nutrition, Medical Faculty, Universitas Syiah Kuala, Banda Aceh, Indonesia
3) Department of Cardiovascular, Medical Faculty, Universitas Syiah Kuala-dr.Zainoel Abidin Hospital,
Banda Aceh, Indonesia
Keywords: CHD, Nutritional Status, Abdominal Obesity, LDL Cholesterol
Abstract: Coronary Heart Disease (CHD) is one of the chronic diseases mainly causing death in developing countries.
Obesity is one of the factors predisposing an increase in LDL cholesterol level. General obesity is assessed
using body mass index (BMI), while abdominal obesity by waist circumference (WC). This study aims to
assess whether nutritional status and abdominal obesity was associated with LDL cholesterol level in
patients with CHD at RSUDZA Banda Aceh. This is an analytic observational study with cross-sectional
design using quota sampling design of non-probability sampling method. Data collected start from October
16 to October 26, 2017. There were 140 patients that meets the inclusion criteria which have been measured
body weight, height, waist circumference, and the LDL cholesterol level obtained from the laboratory
results. The respondents consisting of 77 males and 63 females. 57 respondents (89.1 %) of 64 respondents
with Obese Class 1 (≥25-<30 kg/m
2
) and 120 respondents (88.9%) of 135 respondents with abdominal
obesity have high LDL cholesterol level. Using Spearman test, the result of this study reveals a significant
association between nutritional status and LDL cholesterol level in CHD patients with p value = 0,000
(p<0,05) and moderate positive relationship (r = 0.29) and between abdominal obesity and LDL cholesterol
level in CHD patients with p value = 0.000 (p<0,05) and moderate positive relationship (r = 0.31).
Nutritional status and abdominal obesity are associated with the LDL cholesterol level in CHD patients at
RSUDZA Banda Aceh.
1 INTRODUCTION
Coronary Heart Disease (CHD) is one of the leading
causes of death and one of the chronic diseases in
developing countries
(Amani R. 2010). According to
World Health Organization (WHO), cardiovascular
disease is a disease with worldwide death and
disability, and each year is estimated at 17.3 million
people die from cardiovascular disease where a total
of 7.3 million people occurred due to heart disease
and 6.2 million people due to stroke (WHO 2011).
Coronary heart disease is a non-
communicable disease with impaired heart function
because of blood deficiency to the heart muscle due
to the constriction of coronary artery. Based on the
Basic Health Research Indonesia (RISKESDAS)
2013, the prevalence of CHD in Indonesia is the
seventh of 12 diseases. The prevalence of coronary
heart disease based on a doctor's diagnosis is 0.5
percent and based on symptoms is 1.5 percent.
Coronary heart disease increases with age
(RISKESDAS 2013). The prevalence of coronary
heart disease in Aceh Province based on doctor’s
diagnosis is 0.7 percent and based on symptom is 2.3
percent (Balitbangkes 2013).
Coronary heart disease is characterized by
abnormal accumulation of lipids or fatty and fibrous
tissue in the walls of blood vessels. High-fat foods
(cholesterol) can raise cholesterol in the blood.
Cholesterol and other fatty elements are not soluble
in the blood, but bind to proteins to form soluble
compounds called lipoproteins. The cholesterol
contained in the body slightly binds to lipoproteins
132
Handayani, E., Husnah, . and Ridwan, M.
The Relationship between Nutritional Status and Central Obesity with Low Density Lipoprotein (Ldl) Cholesterol Level in Coronary Heart Disease Patients at Rsudza Banda Aceh.
DOI: 10.5220/0008789701320137
In Proceedings of the 2nd Syiah Kuala International Conference on Medicine and Health Sciences (SKIC-MHS 2018), pages 132-137
ISBN: 978-989-758-438-1
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All r ights reser ved
are Low Density Lipoprotein (LDL) (AlMatsier S
2007).
Cholesterol is transported to the blood in the
form of lipoproteins, 75% LDL cholesterol and 20%
HDL cholesterol. Low LDL cholesterol levels have
a good role in CHD, but excessive LDL cholesterol
will accumulate in the arteries. Cholesterol deposits
in the arteries over time cause narrowing and
stiffening of the arteries, usually called
atherosclerosis, which is a major problem in
coronary heart disease (Joewono S 2013).
Based on Ali Cem's research in 2017, there is
a relationship between body mass index and waist
circumference on coronary heart disease in
Uzunköprü State Hospital, Turkey. The relationship
between abdominal circumference and coronary
heart disease has a stronger correlation. From 292
people with an abdominal circumference > 90 cm,
66 people experienced coronary heart disease. Body
mass index, abdominal circumference and
dyslipidemia are parameters for pathogenesis of
coronary heart disease (Yekdeş 2017).
Research by Karunia in 2015 reveals that
there is a relationship between nutritional status with
HDL and LDL cholesterol levels. There were 50%
of overweight subjects had high serum LDL / HDL
levels. The increasing of LDL cholesterol is
associated with body fat that resides in the adipose
tissue. The adipose tissue will release high levels of
free fatty acids into the portal circulation, thus
disrupting the liver metabolism and stimulating the
liver to produce Very Low Density Lipoprotein
(VLDL), then VLDL particles will be converted into
LDL particles and affect the LDL / HDL ratio
(Agustin K 2015).
Based on research by Medika in 2015, there
is a relationship between abdominal circumference
with LDL cholesterol. As many as 20 people
(54.1%) with abnormal abdominal circumference
have high LDL levels. People with abnormal
abdominal circumference has a 2.64 chance of
having LDL levels (Prasetya M 2015) .The main
cause of elevated LDL cholesterol in the blood is
high saturated fat intake and obesity. Visceral fat
(central obesity) is strongly associated with
metabolic syndrome disorders than total body fat
(general obesity) (Ayu IG 2017).
Obesity has an increased risk of cardiovascular
disease and metabolic diseases such as coronary
heart disease, atherosclerosis, hypertension,
dyslipidemia, diabetes and heart failure (Wilson P
2002). According to the American Heart Association
(AHA), obesity is a major modifying risk factor for
coronary heart disease (Krauss R 2012). Obesity is a
state of increasing total body fat both or in certain
body parts. Obesity can be measured by
anthropometric measurements such as Body Mass
Index (IMT) and abdominal circumference. The
negative effects of excess body weight on blood
cholesterol contribute about 45% in increasing the
risk of CHD(Wilson P 2002). (Widyastuti 2006).
2 METHOD
The study was observational analytic with cross-
sectional design in Polyclinic of Cardiology at
RSUDZA Banda Aceh in October 2017. The
population was all patients with Coronary Heart
Disease diagnosis in Polyclinic of Cardiology at
General Hospital dr. Zainoel Abidin Banda Aceh
2017, the sample was taken by quota sampling and
met the inclusion criteria. The sample was chosen by
non probability sampling method. The primary data
collected by measuring body weight, height and
abdominal circumference, and secondary data
obtained from laboratory results of LDL cholesterol
levels of CHD patients. Statistical analysis with
univariate analysis was used for frequency
distribution and Correlation Spearman Test for
bivariate analysis.
3. RESULTS AND DISCUSSION
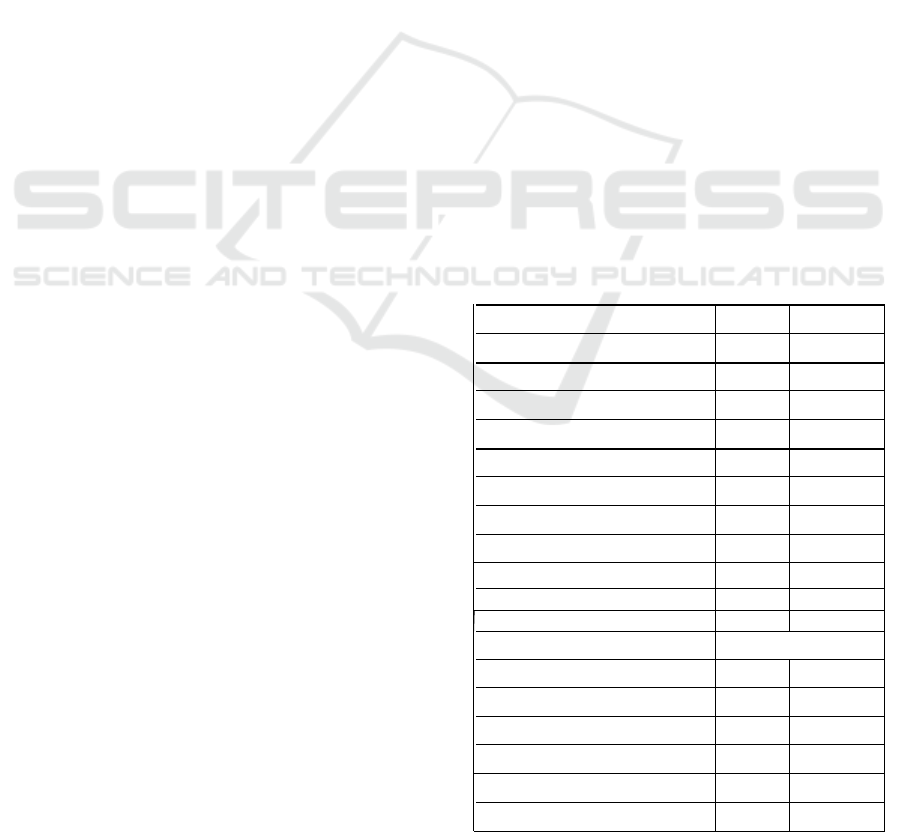
Table 1 General Characteristics of CHD Patients
General
n=140
(
%
)
Characteristics
Sex
Men
77 55,0
Women
63 45,0
Age (years)
17-25
2 1,4
26-35
7 5,0
36-45
19 13,6
46-55
42 30,0
56-65
56 40,0
>65
14 10,0
Educational level
No school
1
0,7
Elementary school
15
10,7
Junior Hi
g
h School
25
17,9
Senior Hi
g
h School
47
33,6
Bachelo
r
51
36,4
Ma
g
iste
r
1
0,7
The Relationship between Nutritional Status and Central Obesity with Low Density Lipoprotein (Ldl) Cholesterol Level in Coronary Heart
Disease Patients at Rsudza Banda Aceh
133
Occu
p
ational
Unem
p
lo
y
ment
1 0,7
Housewife
44 31,4
Entre
p
reneu
r
48 34,3
Teacher/Lecture
r
5 3,6
Employee
34 24,3
Retirement
7 5
College student
1 0,7
Based on Table 1 the CHD patients was dominantly
men were 77 people (55,0%). Group of age 55-65
years were 56 people (40%). Bachelor, dominantly
in educational level, were 51 people (36,4%).
Entrepeneur was themost patients’ occupation, were
48 people (34,3%).
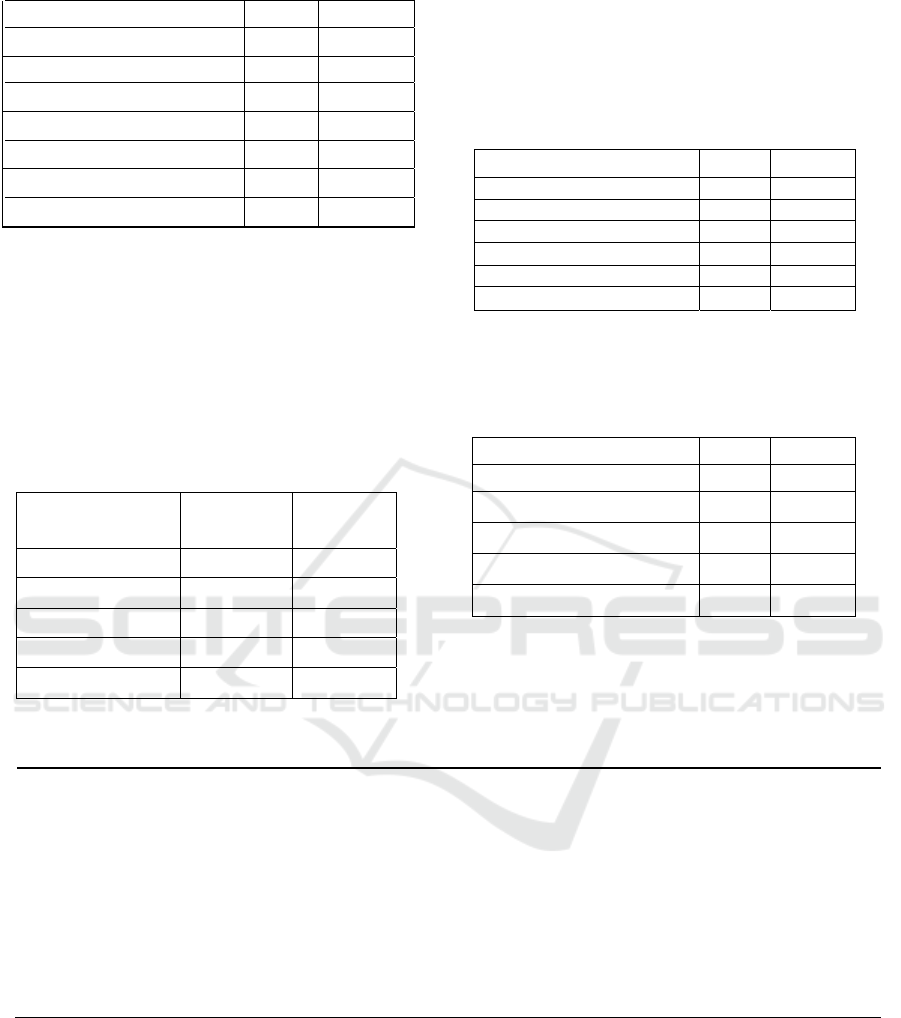
Table 2 The distribution of nutritional status of CHD
patients
Nutritional status (n=14
0)
(%)
Underweight
1
0,7
Normal
35 25,0
Overweight
37 26,4
Obesity I
64 45,7
Obesity II
3 2,1
Table 2 indicates CHD patients were dominantly
have obesity grade 1, were 64 people (45,7%),
subject with underweight were 1 people (0,7%).
Table 3 The distribution of Central Obesity of
CHD patients
Abdominal Circumference
n=140
(%)
Normal
Men
2 1,4
Women
3 2,1
Abnormal
Men
75 53,6
Women
60 42,9
Table 3 reveals that the highest central obesity is
found in men, were 75 people (53.6%).
Table 4 Laboratory results of CHD patients, were
obtained LDL cholesterol levels.
LDL cholesterol level
n=140
(%)
Near optimal
0 0
Optimal
0 0
Borderline high
5 3,6
High
124 88,6
Very high
11 7,9
Table 4 reveals that 124 respondents (88,6%) have
high LDL cholesterol.
Table 5 The relationship between nutritional status and LDL cholesterol level of CHD Patients
Nutritional
Status
LDL Cholesterol Level
Borderline high High Very high Total
P-Value
r
n
%
n
%
n
%
n
%
Underweight 1
100 00 0
0
0 1 100
Normal 4
11,4 228 80
3
8,6 35 100
Overweight 0
0 337 100
0
0 37 100
0,000 0,29
Obesity I
0
0 557 89,1
7
10,9 64 100
Obesity II
0
0 22 66,7
1
33,3 3 100
Based on table 5, indicates form 35 respondents with normal nutritionl status,there were 28 people (80%) had
high LDL cholesterol level, from 37 people (100%) had high LDL cholesterol level, from 64 respondents with
obesity I, there were 57 people (89.1%) had high LDL cholesterol levels and from 3 respondents with obesity
II, 2 people (66,7%) had high LDL cholesterol level. The result revealed p value=0.000(p<0,05), there is
coreelation between nutritional status and LDL cholesterol level of CHD patients in polyclinic of cardiology
in RSUDZA Banda Aceh, and correlation coefficient value (r=0,291) means the strength of relation both
variable is enough.
SKIC-MHS 2018 - The 2nd Syiah Kuala International Conference on Medicine and Health Sciences
134

Tabel 6 The relationship between central obesity and LDL cholesterol level of CHD patients
Central
Obesity
LDL Cholesterol Level Total
p
-value
Borderline
hi
g
h
High Very high
n % n % n % n %
Normal 1
20.0
4
80.0
0
0.0 5 100.0
Abnormal 4
3.0 120
88.9
11
8.1 135 100.0
0,000 0,31
Based on Table 6, indicates that of 135 central obesity respondents, 120 people (88.9%) had high LDL cholesterol and
11 people (8.1%) had very high cholesterol levels. The result of p value = 0.000 (p
<0,05) shows that there is correlation between central obesity and LDL cholesterol level of CHD patients in
Polyclinic of Cardiology in RSUDZA Banda Aceh,
correlation coefficient value (r = 0,31) means the strength of relation both variables is enough.
4. CONCLUSION
The study results obtained 64 people (45.7%) with obesity
I and 3 people with obesity II (2.1%). This study coincides
with study by Mohammad Ifard 2013 in Iran on 12,416
respondents of CHD patients average on BMI 25.6 kg/m
2
have obesity status.(Mohammadifard N 2013). Obesity is
a major modifying risk factor for CHD disease. (Krauss
R 2012).
The negative effects of excess weight on blood
pressure and blood cholesterol contribute about 45% in
increasing the risk of CHD and there is an independent
increase of significant risk of the factor. Study by
Iskandar 2017 also find that although there is a slight
increase in body weight above normal, it can increase the
risk of CHD (Hadil A 2017).
The study results of the study found that 135
people (96.5%) of CHD patients had central obesity.
Central obesity is an indicator of cardiovascular
diseases(Sugondo 2009). This The relationship between
nutritional status and LDL cholesterol level of CHD
patients study is in line with research by Ratih 2015,
Women with abdominal circumferences >80 cm will
have 1.5 times risk affected by CHD compared to women
whose abdominal
circumference <80 cm(
Oemiati R 2015).
Obesity central is
influenced by unbalanced energy intake
and lack of physical activity so fat accumulation is more
prevalent in the abdomen because fat cells in the abdomen
are larger. Excess fat is stored in the form of triglycerides
in
fatty
tissue,
in
addition, lifestyle modernization, high
caloric intake, low physical activity is also a result of
increased central obesity which is a risk factor of
CHD (Dewi A 2013).
The study results obtained 124 people (88.6%)
with high LDL cholesterol levels. study coincides
Ma'rufi
2014, the percentage of patients with
LDL> 130 mg / dL
in the CHD group was 65.6% (Ma’rufi 2014). If foods
containing saturated fats consumed in excess amounts can
cause an increase of blood cholesterol, usually called
hypercholesterolaemia
(Dewi A 2013).
Increased levels
of
LDL cholesterol is one of the risk factors for coronary
heart disease. The high levels of LDL cholesterol that
accumulate on the
subendothelial
layer,
LDL cholesterol
is atherogenic which can lead to atherosclerosis (Ma’rufi
2014).
The Spearman Correlation test results obtained p
value = 0.000 (p <0.05) with correlation coefficient value
(r = 0.29). This suggests that there is a relationship
between nutritional status and LDL cholesterol levels in
CHD patients with the strength of relation is enough.
From 64 respondents who have obesity I, there were 57
people (89.1%) had high LDL cholesterol levels. It
signifies that the increasing of nutritional status in a
person tends to affect the increasing of LDL cholesterol
levels. This result is in line with the research of Ali Cem
2017 conducted in Turkey, there were 66 respondents who
experienced CHD had high cholesterol levels with obesity
nutritional status (p-value = 0,049 (Yekdeş 2017).
Obesity is a state of increased total body fat or in
certain body parts. Overweight and obesity have a
relationship with other risk factors in CHD, one of them is
dyslipidemia. LDL cholesterol will be carried to the
tissues including arteries that over time will lead to the
accumulation of fatty plaque in the arteries. If the fatty
plaques accumulate in coronary artery, often called
atherosclerosis, which is the initial cause of coronary heart
disease(Blu DI 2012).
This research is not in line with Tracey's research
2012 at BLU / RSUP. Prof. Dr. R.D.Kandao Manado,
from 62 cases with normal BMI, there were 5 people
normal without CHD (29,4%), and experienced CHD
were 12 people (70,6%). Patients with obesity I, There
were is 2 people normal without CHD (8.7%) and
suffering CHD were 21 people (91.3%). The study
showed p value = 0,135 which means p> 0,05), there is no
relationship between obesity and coronary heart disease.
The absence of a significant association in this study may
be there was the number of other risk factors for
unrecoverable CHDs such as heredity or genetics, age and
sex factors, as well as other factors related to behaviors
such as smoking, alcohol consumption and other history
of diseases such as diabetes melitus, hypertension,
improper diets or infectious diseases that strike attack the
blood and blood vessels (Blood NHL 2011)
.
The
relationship between central obesity and LDL cholesterol
level of CHD patients.
The study results in Polyclinic of Cardiology in
RSUDZA found that there is the relationship between
central obesity with LDL cholesterol levels of CHD
patients. From 135 respondents who had central obesity,
there were 120 people (88.9%) had high LDL cholesterol
The Relationship between Nutritional Status and Central Obesity with Low Density Lipoprotein (Ldl) Cholesterol Level in Coronary Heart
Disease Patients at Rsudza Banda Aceh
135

levels. The Spearman Correlation test results obtained p =
0,000 (α <0.05) with correlation coefficient value (r =
0.31). The result is in line with research by Medika 2015
in Dr. M. Djamil Padang Hospital. It was obtained there
were 20 people (54,1%) with abnormal abdominal
circumference and high LDL level (p = 0,02) which mean
there is difference of proportion of high LDL level
between abnormal abdominal abdominal respondent with
high LDL level with OR = 2, 64, meaning people with
abnormal abdominal circumference has a 2.64 chance of
having high LDL levels compared to respondents with
normal abdominal circumference (Prasetya M 2015).
The direct effects of excessive fat in the abdomen,
causing a person to have central obesity (Ayu IG 2007).
High intake of saturated fat diet also increase plasma
cholesterol levels with an increase about 15% -25%. This
is because there is a fat deposit in the liver which then
causing the increase of acetyl-koA in the liver to produce
cholesterol (Guyton A 2007). The high levels of LDL
cholesterol in the blood can cause the lack of antioxidants
in the blood vessels so that endothelias are more
susceptible to have endothelial injury that can cause
atherosclerosis in CHD patients (Sudoyo A 2009).
5. SUGESTION
The Nutritional status of CHD patients in the Polyclinic of
Cardiology in RSUDZA Banda Aceh are more
predominantly patients with obese I (45.7%). CHD
patients in Polyclinic of Cardiology in RSUDZA Banda
Aceh are more dominant had central obesity (96.5%).
LDL cholesterol levels of CHD patients were more
dominantly high (88.6%). There is a relationship between
nutritional status and central obesity with LDL cholesterol
levels in CHD patients in Polyclinic of Cardiology in
RSUDZA Banda Aceh.
For related institutions, better to always measuring
abdominal circumference to patients on a regular basis in
order to evaluate LDL cholesterol levels of CHD patients.
For other researchers, it is expected to conduct further
research on other factors that affect LDL cholesterol levels
that also have a high risk for CHD and aggravate CHD
with a larger number of respondents.
REFERENCES
Amani R, Noorizadeh M, Rahmanian S, Afzali N,
Haghighizadeh MH. Nutritional related cardiovascular
risk factors in patients with coronary artery disease in
IRAN: A case-control study. 2010;1–6.
AlMatsier S. Penuntun Diet. Jakarta: Gramedia Pustaka
Utama; 2007.
Agustin K. Hubungan Indeks Massa Tubuh dan Asam
Lemak Jenuh dengan Serum Rasio LDL / HDL
Lansia. 2015;
Ayu IG, Rasdini A. Hubungan Lingkar Pinggang dengan
Kadar Kolesterol LDL Pasien Penyakit Jantung
Koroner di Ruang ICCU RSUP Sanglah Denpasar.
2007;
Sudoyo A. Buku Ajar Ilmu Penyakit Dalam. 5th ed.
Setiyohadi B, Alwi I, editors Jakarta: Interna
Publishing; 2009. 1937-41 p
Badan Penelitian dan Pengembangan Kesehatan. Riset
Kesehatan Dasar (RISKESDAS) 2013. Lap Nas 2013.
2013;91–3.
Balitbangkes. Riset Kesehatan Dasar 2013 Berdasarkan
Provinsi Aceh [Internet]. Vol. 7. 2013. 17-26 p
Available from: terbitan.litbangkes.depkes.go.id
Blu Di, prof R, Manado RDK, Rampas CCW, Rampengan
SH. Penyakit Jantung Koroner Pada Pasien.
2012;(November):1–6.
Blood NHL and, Institute. Coronary Heart Disease Risk
Factors [Internet]. 2011. Availablefrom:
http://www.nhlbi.nih.gov/health/health-
topics/topics/hd/atrisk.html
Dewi A. Obesitas Sentral dan Kadar Kolesterol Darah.
2013;9(1):37–43.
Hadil A, Hadi A. Risk factors of coronary heart disease in
Meuraxa hospital of Banda Aceh 2017;2(July
2015):32–42
Joewono S. Ilmu Penyakit Jantung. Surabaya: Airlangga
University Press; 2013.
Krauss R, Winston M. Obesity Impact on Cardiovascular
Disease. Am Hear Assoc Inc [Internet]. 2012;
Available
from: http://circ.ahajournals.org/ content/98/14/1472
Mohammadifard N. Body Mass Index, Waist-
circumference and Cardiovascular Disease Risk
Factors in Iranian Adults : Isfahan Healthy Heart
Program. 2013;31(3):388–97.
Ma’rufi. Hubungan Dislipidemia dan Kejadian Penyakit
Jantung Koroner 2014;6(1):1–7
Oemiati R. FAKTOR RISIKO PENYAKIT JANTUNG
KORONER ( PJK ) PADA PEREMPUAN ( Baseline
Studi Kohor Faktor Risiko PTM ) ( Risk Factors for
Coronary Heart Disease ( CHD ) in Women ( Baseline
Cohort Study of Risk Factors for Non Communicable
Disease). 2015;5:47– 55.
Prasetya M, Oenzil F, Karani Y. Hubungan Indeks Masa
Tubuh dan Lingkar Perut dengan Low Density
Lipoprotein Pada Pasien Penyakit Jantung Koroner di
Poliklinik Jantung RSUP Dr. M. Djamil Padang. J
Kesehat Andalas [Internet]. 2015;4(3):737–42.
Sugondo. Obesitas. IV. Sudoyo, editor. Jakarta: Pusat
Penerbitan IPD FKUI; 2009. 1919-1923 p
Wilson P, D’Agostino R, Sullivan L,Parise H, Kannel
W. Overweight andObesity as Determinants of
Cardiovascular Risk: The FraminghamExperience.
Arch Intern Med. 2002;(162):1867–
WHO. Cardiovascular Diseases. NMH Fact Sheet,
2011:1-
SKIC-MHS 2018 - The 2nd Syiah Kuala International Conference on Medicine and Health Sciences
136

Widyastuti, Nurmasari, Subagio HW. Hubungan Beberapa
Indikator Obesitas dan Hipertensi Pada Perempuan.
Media Med Indones. 2006;1(41)
Guyton A, Hall J. Buku Ajar Fisiologi Kedokteran. 11th
ed. Irawati editor. Jakarta: EGC; 2007.8882-94 p.
Yekdeş AC. Indian Journal of Medical Research and
Pharmaceutical Sciences With Metabolic Syndrome
Indian Journal of Medical Research and
Pharmaceutical Sciences. 2017;4(June):1–9.
The Relationship between Nutritional Status and Central Obesity with Low Density Lipoprotein (Ldl) Cholesterol Level in Coronary Heart
Disease Patients at Rsudza Banda Aceh
137
