
The Effectiveness of Dialectical Behavior Therapy in Developing
Emotion Regulation Skill for Adolescent with Intellectual Disability
Shahnaz Safitri, Rose Mini Agoes Salim, and Pratiwi Widyasari
Faculty of Psychology, Universitas Indonesia, UI Campus, Depok, Indonesia
Keywords: Dialectical Behavior Therapy; Emotion Regulation; Intellectual Disability.
Abstract: Intellectual disability is characterized by significant limitations in intellectual functioning and adaptive
behaviour that appears before the age of 18 years old. The prominent impacts of intellectual disability in
adolescent are failure to establish interpersonal relationships as socially expected and lower academic
achievement. Meanwhile, it is known that emotion regulation skill has a role in supporting the functioning
of individual, either by nourishing the development of social skill as well as by facilitating the process of
learning and adaptation in school. This study aims to look for the effectiveness of Dialectical Behaviour
Therapy (DBT) in developing emotion regulation skill for adolescent with intellectual disability. DBT’s
special consideration toward clients’ social environment and their biological condition is foreseen to be the
key for developing emotion regulation capacity in adolescent client with intellectual disability. Through
observations on client’s behaviour, conducted before and after the completion of DBT intervention program,
it was found that there is an improvement in client’s knowledge and attitude related to the mastery of
emotion regulation skills. In addition, client’s consistency to actually practice emotion regulation techniques
over time is largely influenced by the support received from the client’s social circle.
1 INTRODUCTION
Adolescence is a transitional period of development
starting from the age of 10 into adulthood. The
distinctive feature of adolescents is that their
emotional state is rapidly fluctuated over time in
response to their environment. It is said that this
state of emotional fluctuation makes them
vulnerable to anger and aggressive behaviour when
facing unpleasant situations (Papalia, Olds, and
Feldman, 2010). Furthermore, adolescents also tend
to be more reactive to their surrounding and more
often feel negative emotions. Such condition
becomes a potential for them to engage in a
relational conflict, be it with parents, peers, and
other social circles (Gross, 2012).
Mastering social skill supports the adolescents
on their adaptation to everyday social situations
(Gross, 2012). The need to adapt adequately is of
particular concern for adolescent with intellectual
disabilities. Intellectual disability is a condition
marked by significant limitation in intellectual
function and adaptive behaviour which emerging
before the age of 18 years old (Hallahan and
Kaufman, 2006). Commonly found in adolescents
with intellectual disability is a typical growth of
physical development, in which it is in accordance to
the chronological age. However, their cognition and
social emotional aspects are underdeveloped
compare to their peers. It is stated that this
developmental discrepancy has occurred since the
early onset of development and continues into
adulthood (Barbosa, 2007; Pereira and Faria, 2015).
Because of their developmental discrepancy,
adolescents with intellectual disability often receive
unrealistic social expectations in their everyday life.
They are often seen by others as high functioning
individuals who are capable of an adequate social
interaction, given that their physical appearance is
just like a typical person of their age. As no surprise,
adolescents with intellectual disability tend to be
unable to meet the expectations in their conduct of
social interaction (Marinho, 2000; Pereira and Faria,
2015). The combination of delayed development in
both cognitive and social emotional aspect leads to
their failure of building interpersonal relationship as
expected. This failure leads to an isolation and
rejection by peers, which is the main cause of stress
and negative self-concept in adolescents with
Safitri, S., Salim, R. and Widyasari, P.
The Effectiveness of Dialectical Behavior Therapy in Developing Emotion Regulation Skill for Adolescent with Intellectual Disability.
DOI: 10.5220/0008589303510359
In Proceedings of the 3rd International Conference on Psychology in Health, Educational, Social, and Organizational Settings (ICP-HESOS 2018) - Improving Mental Health and Harmony in
Global Community, pages 351-359
ISBN: 978-989-758-435-0
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
351

intellectual disability (Blackwell, 1979, Hauser-
Cram and Krauss, 2004).
Another study by Wiltz (2005) suggests that the
majority of individuals with intellectual disability
often have a limited number of friends. Furthermore,
their friendship tends to be full of conflict and
unstable. It is mentioned that this friendship is
difficult to maintain due to their difficulty in social
skill, such as translating social signals of facial
expression. This makes individuals with intellectual
disability become vulnerable to loneliness, and in
the extreme case they can suffer from depression
(Heiman, 2000 in Wiltz, 2005).
In general, as adolescent grow with increasing
age, followed by development in cognitive abilities,
they are gradually be more able to regulate their
emotions in order to fit themselves in daily social
and moral norms (Papalia, Olds, and Feldman,
2010). Unlike adolescent in general, the chronic
developmental discrepancy in adolescents with
intellectual disability becomes a major factor for
their difficulty in developing another skill, one of
them is on regulating emotion. Furthermore, it is
known that the difficulty in regulating emotions is
the reason for their inadequate social interaction
(Baurain and Grosbois, 2012). This dynamic shows
that emotion regulation skill is important for
adolescents with intellectual disability to adapt to
social environment (Gross, 2012).
Emotional regulation is defined as an individual
process for actively adjusting their emotional
experiences by considering the type of emotions, the
time of and for experiencing emotions, and how
those emotions are channelled (Gross and Thomson,
2007). It is said that emotion regulation is part of the
overall individual adjustment to his/her external
environment (Baurain and Grosbois, 2012).
Furthermore, emotion regulation is also part of a
general self-regulation, a process that allows
individuals to flexibly respond to changing
environmental context but still in line to their pursuit
of goals (Mennin and Fresco, 2014).
The emotion regulation skill promotes the
development of individual social skills. It is known
that mastering emotion regulation contributes to the
formation of social competencies in adolescents,
both for short-term and long-term period
(Einsenberg, 1997 in Gumora and Arsenio, 2002).
Especially in adolescents with intellectual disability,
emotion regulation skill is needed to develop their
underdeveloped social skills in order to blend in
with society and avoid social isolation, bullying, and
victimization. In addition, the mastery of social
skills supports the individual not to display an
aggressive and violent behaviour, which is also
commonly found in individuals with intellectual
disability (Hauser-Cram and Krauss, 2004; O'clare,
Waasdorp, Pas, and Bradshaw, 2015).
In accordance with developing social
competence, a well-developed emotion regulation
skill is also known to facilitate the creation of a
positive relationship between students and teachers.
This then becomes a contributing factor in enabling
students to smoothly learn from the teachers and
build their achievement motivation (Graziano,
Reavis, Keane, and Calkins, 2007). The lack of
cognitive ability in adolescent with intellectual
disability makes learning difficult for them and
brings out negative emotions (Gumora and Arsenio,
2002). Therefore, their capacity to regulate those
negative emotions foster them to survive the
learning process regardless their cognitive
constraints (Denham, Basset, Mincic, Kalb, Way,
Wyatt, and Segal, 2012). Without emotion
regulation, their learning achievement and academic
adjustment tend to be low. In fact, school adjustment
is known as a predictor for their life adjustment in
the long run (Eisenhower, Baker, and Blacher,
2007).
All these description shows that there is a need
for adolescent with intellectual disabilities to
improve emotion regulation skill. By definition,
emotion regulation involves the process of
individual actively adjusting his/her experience by
considering the type of emotion, the time of
experience, and how the emotion is channelled
(Gross and Thomson, 2007). Thus, the basis of
emotion regulation skill is the ability to distinguish
the types of emotion (Linehan, 1993 in McWilliams,
deTerte, Leathem, Malcolm, and Watson, 2014).
The ability to differentiate emotion is also a part of
an important social skill, since it facilitates
individual to behave appropriately regardless the
current emotional state. Individual who is more
aware of his/her emotional state tends to be easier to
regulate the emotion experienced (Gross, 2006).
Research by Baurain and Grosbois (2012)
suggests that individual with intellectual disability
have a delayed emotion regulation skill development
compare to the peers. This delay explains their lesser
frequency and quality of social behaviour, in which
it continues throughout adulthood. On the other
hand, this study provides an insight that that the
ability to regulate emotion in individual with
intellectual disability improves gradually as they get
older. Thus, a program to enhance the emotion
regulation skill in individual with intellectual
ICP-HESOS 2018 - International Conference on Psychology in Health, Educational, Social, and Organizational Settings
352

disabilities is applicable to optimize their
capabilities.
There are numbers of therapy that specifically
aim to develop emotion regulation skill, such as
Emotion Regulation Therapy (ERT), Attention
Modification, Affect Regulation Training (AFT),
Mindfulness Training (MT), and Dialectical
Behaviour Therapy (DBT). All of these therapies
focus on empowering the individual's ability to
master emotion regulatory skill using cognitive and
behavioural strategies (Gross, 2014). Nevertheless,
Attention Modification, AFT, and MT require
clients to possess an adequate cognitive function to
concentrate to the environmental stimulus; so that
they can manage the emotions associated with the
stimulus (Berking and Schwarz, 2014; MacLeod and
Grafton, 2014; Farb, Anderson, Irving and Segal,
2014). Furthermore, the ERT technique demands a
lot of higher order thinking to know one’s own value
in the process of regulating emotions (Mennin and
Fresco, 2014). Meanwhile, individual with
intellectual disability has limitation in their cognitive
function (Hallahan and Kaufman, 2006).
In contrast to other therapies, DBT views the
difficulty for regulating emotion as an implication of
various biological and non-supportive environmental
factors (Lew, Matta, Trip-Tebbo, and Watts, 2006).
Thus, DBT is particularly concerned about how
environmental and individual histories play a role in
his/her ability to regulate emotion (Gross, 2014).
Biological factors include cognitive capacity; while
environmental factors, among others, are the lack of
opportunity and feedback from the social
environment for individual to exercise emotion
regulation (Njardvik, Matson, and Cherry, 1999).
DBT's special consideration to personal factors
makes this therapy an appropriate alternative to be
delivered to individual with intellectual disability. In
DBT, the therapeutic emphasis is placed on the
positive and non-judgmental climate. Furthermore,
DBT focuses on preparing clients to be able to stand
for themselves using the skills taught, while
ensuring the availability of coaches that clients can
rely on in times of crisis (Lew, Matta, Trip-Tebbo,
and Watts, 2006). This is in line with the spirit of
education for individual with intellectual disability,
which is to develop their independence while
considering their magnitude of disability. It is
known a more severe disability require more
intensive assistance (Mangunsong, 2009). This
concept is in accordance with the characteristic of
adolescents with intellectual disability who still
require guidance when necessary.
Furthermore, DBT is also taking into account the
environmental factors that shape individual's life
history related to the opportunity to exercise emotion
regulation skill (Lew, Matta, Trip-Tebbo, and Watts,
2006). It is said that individual with intellectual
disability are often live a condition of over-
protective family, so that they have no experience
for decision making. Furthermore, individual
surrounding is often unresponsive to emotional
expression except for negative emotional display.
Thus, the individual gets reinforcement for this
negative emotion expression. DBT through one of
its several modes of intervention - structuring client's
environment - responds this environmental challenge
in relation to developing emotion regulation skill
(Lew, Matta, Trip-Tebbo, and Watts, 2006). This is
done by involving family members in training, as
well as re-arranging clients’ room with several tools,
such as journal of daily emotional state. These
practices are also in line with the principle of
education in individual with intellectual disability, in
which modification of space is sometimes needed
for the learning process (Mangunsong, 2009).
This paper describes the process of conducting
DBT in special population of adolescent with
intellectual disability. It is known that DBT has five
modes of intervention, which are individual therapy,
skills training, coaching in crisis, structuring the
environment, and consultation team. However, it is
said that skill training is the most essential element
of DBT among all other modes (Soler, et.al, 2009).
Another study by Sakdalan, Shaw, and Collier
(2010) found that skill training is the only mode of
all DBT intervention that can be delivered solely
without other modes. Based on the information
gathered, we aim to test the DBT's skill training
effectiveness for improving emotion regulation skill
in adolescent with intellectual disability. As far as
we concern, this is the first study to seek out the skill
training effectiveness in the context of client with
the mentioned characteristic.
2 METHOD
2.1 Research Question and Hypothesis
This study aims to answer if Dialectical Behavior
Therapy technique can be used to improve emotion
regulation skill in adolescent with intellectual
disability. We propose a hypothesis that Dialectical
Behavior Therapy technique is effective to improve
emotion regulation skill in adolescents with
intellectual disability.
The Effectiveness of Dialectical Behavior Therapy in Developing Emotion Regulation Skill for Adolescent with Intellectual Disability
353

2.2 Research Design
We use single subject design in which the
measurement to answer the research question is
conducted to one subject. In a single subject design,
the researcher focuses on the behaviour the subject
raises before the program is given and after the
program is completed. (Gravetter and Forzano,
2009). Therefore, there is period of baseline
observation being conducted prior to the delivery of
intervention program. This is done to get an accurate
portrait of subject’s behaviour in daily life in respect
to the his/her capacity to regulate emotion.
2.3 Participant
The subject is adolescent with intellectual disability
with difficulty in emotion regulation skill. By
definition, the characteristic is applied to those in
age of 10 years old to early twenties (Papalia, Olds,
and Feldman, 2010). In addition, they possess an
intellectual disability in which there is significant
limitation of intellectual function and adaptive
behaviour manifested through conceptual, social,
and practical adaptive abilities (Hallahan and
Kaufman, 2006). A girl aged 16 years old with
intellectual disability is referred to the researcher
with characteristic of having difficulty in social
interaction due to the inability to regulate emotion.
2.4 Overview of Intervention Program
In providing DBT to individual with intellectual
disability, there are number of challenges to be faced
(Lew, Tripp-Tebo, and Watts, 2006). Those
challenges are as follow:
1. The standard DBT practice is constrained by
the clients' language capacity, in which they
tend to communicate in a much simpler
vocabulary.
2. Some clients with intellectual disability tend to
be unready for a group activity.
Charlton and Dykstra (2011) describes that the
adaptation of DBT is a must. One of the ways is by
conveying information during intervention using
various modalities. In this study we use various
materials and activities, which are ranging from
working on coloured worksheet, watching cartoon
videos, and doing physical movement. In addition, a
simple language is required to teach the client during
intervention, so that it is easier for them to
understand what is taught by the therapist. We use a
simple vocabulary to speak, and switch the word in
worksheet with a relevant image to serve as a
symbol for the client to understand the meaning. The
use of symbol is due to the client's inability to read.
Furthermore, it is said that the materials
containing information for client need to be tailored
to attract the attention and facilitate understanding
(Charlton and Dykstra, 2011). This is done by
containing the images of the client's idol in every
material given to maximize her excitement to learn.
Bailie and Slater (2014) adds that the content of the
intervention needs to be conveyed by linking to what
client has already known. The content must also be
in line with what is faced by clients in their daily
life, so that they can apply the skill directly in daily
affair. Therefore, we observe the subject and
interview her family to gain a deeper understanding
of her daily life before the intervention is conducted.
Intervention also needs to be implemented in a
simple therapeutic structure using concrete
activities. A clear rule is also needed during client's
participation throughout the intervention process.
The therapist also needs to be more active and
directive to the client compare to teaching client
without disability. Throughout the intervention
process, repetition of the material taught becomes
important and is part of the overall intervention
structure. Therefore, there is a need for a special
time allocation to review the lessons and various
situations to apply the emotion regulation skill being
taught, in order to facilitate client in making
generalization of the knowledge and skills (Charlton
and Tallant, 2003 in Charlton and Dykstra, 2011).
Another DBT adaptation is that the therapist
should involve client's family members, teachers, or
other caregivers into the intervention process. This is
done to ensure that caregivers can practice the same
skills as learned by the client. It is beneficial for
clients if their caregivers gain these same knowledge
and skills to further act as their coaches and facilitate
mentorship in everyday life (Charlton and Dykstra,
2011). Therefore, a special session is held to teach
the client's mother and teachers all the programs
activities and objectives. They are also given a
responsibility to ensure the client do her homework
and fill the journal designed by the researcher to
observe the client's progress in home and in schools.
2.5 The Program Objective
In the standard DBT's skills training, there are 10
objectives to be reached. The mastery of the first 6
objective of the training is a prerequisite to be
further able in mastering a more advanced emotion
regulation skill (McKay, Wood, and Brantley,
2007). Therefore, this study focuses on targeting the
ICP-HESOS 2018 - International Conference on Psychology in Health, Educational, Social, and Organizational Settings
354

first 6 objectives to be adopted as the program's
goal. The details are as follows:
1. Subject is able to recognize various types of
basic emotions.
2. Subject is able to recognize their own
emotions.
3. Subject understands the process of emotion
formation.
4. Subject is able to manage negative emotions.
5. Subject knows how to increase the emergence
of positive emotions.
6. Subject knows the factors that affect the
emotion regulation process.
2.6 Program's Targeted Behaviour
In general, the program is considered successful if
there is an increase in the emotion regulation skill
shown by the subject. It is indicated by several
indicators:
1. Subject can identify the types of basic
emotions
The subject is said to be able to identify the
types of basic emotions when she can name all
the 6 different basic emotion as shown is the 6
coloured emotion cards. Otherwise, subject
need also to be able to choose the right emotion
card according to type of emotion mentioned
by researcher.
2. Subject can identify the emotions they feel in
real situations.
The subject is said to be able to identify the
emotions she feels when she can tell her
emotional experience according to the emotion
card given by researcher. This applies to all six
basic emotions.
3. Subject understands the process of emotion
formation, by identifying the situation that
cause emotion, the background thoughts, the
emotion emerged, and the action to respond to
situations.
Subject is said to be able to understand the
process of emotion formation when she can
accurately arrange a series of display card that
contain image/symbol associated with the four
stage of emotion formation. Furthermore,
subject also needs to tell a story of six basic
emotions emergence by matching the story
card to the relevant emotional sequence card
arranged first. The story is both gathered from
the subject experience and also from 6 cartoon
videos containing different emotional display.
4. Subject can manage the negative emotions
experience
The subject is said to be able to manage
negative emotions if she can demonstrate the
correct "stop-think-relax" technique in the
proper sequence as taught in the program.
5. Subject knows how to improve his/her positive
emotions
The subject is said to know how to improve her
positive emotion when she can mention all
different activities taught in generating positive
emotions. She needs to remember the activities
without any clue given.
6. Subject knows the vulnerability factor in the
process of emotion regulation
The subject is said to know the factors affected
emotion regulation when she can mention the
meaning of the symbolic images, given as a
work-sheet, that refer to these factors.
2.7 Program Implementation
The intervention is conducted by having one session
a day to make the learning conducive to the client's
capacity to learn. The program details are listed in
the Table 1.
In practice, we found that the session 2 of the
intervention needed repetition, since the subject
cannot answer the review questions asked on the
following day. In addition, the post-test 2 of the
study was failed to be delivered on schedule due to
the client's health condition. Therefore, the aim to
seek out if the subject's attainment of program
indicator is still intact was done by relying on the
observational worksheet filled out by the client's
mother at home. In conclusion, the intervention was
executed as an 8 days intervention as planned but
with different sequences.
2.8 Data Analysis
As in standard DBT's skill training, this research use
observation as a method to measure the completion
of program's goal and test the intervention
effectiveness. Observation takes place before and
after intervention is held, focusing on achievement
of behavior indicator. The score is given to the
subject for every successful attainment on program's
objectives. The percentage of achievement score
before and after intervention is then compared to
grab the picture of program effectiveness in
improving subject's emotion regulation skill. The
additional data analysis is done using a behavioral
checklist filled out by the mother and teacher of the
clients.
The Effectiveness of Dialectical Behavior Therapy in Developing Emotion Regulation Skill for Adolescent with Intellectual Disability
355
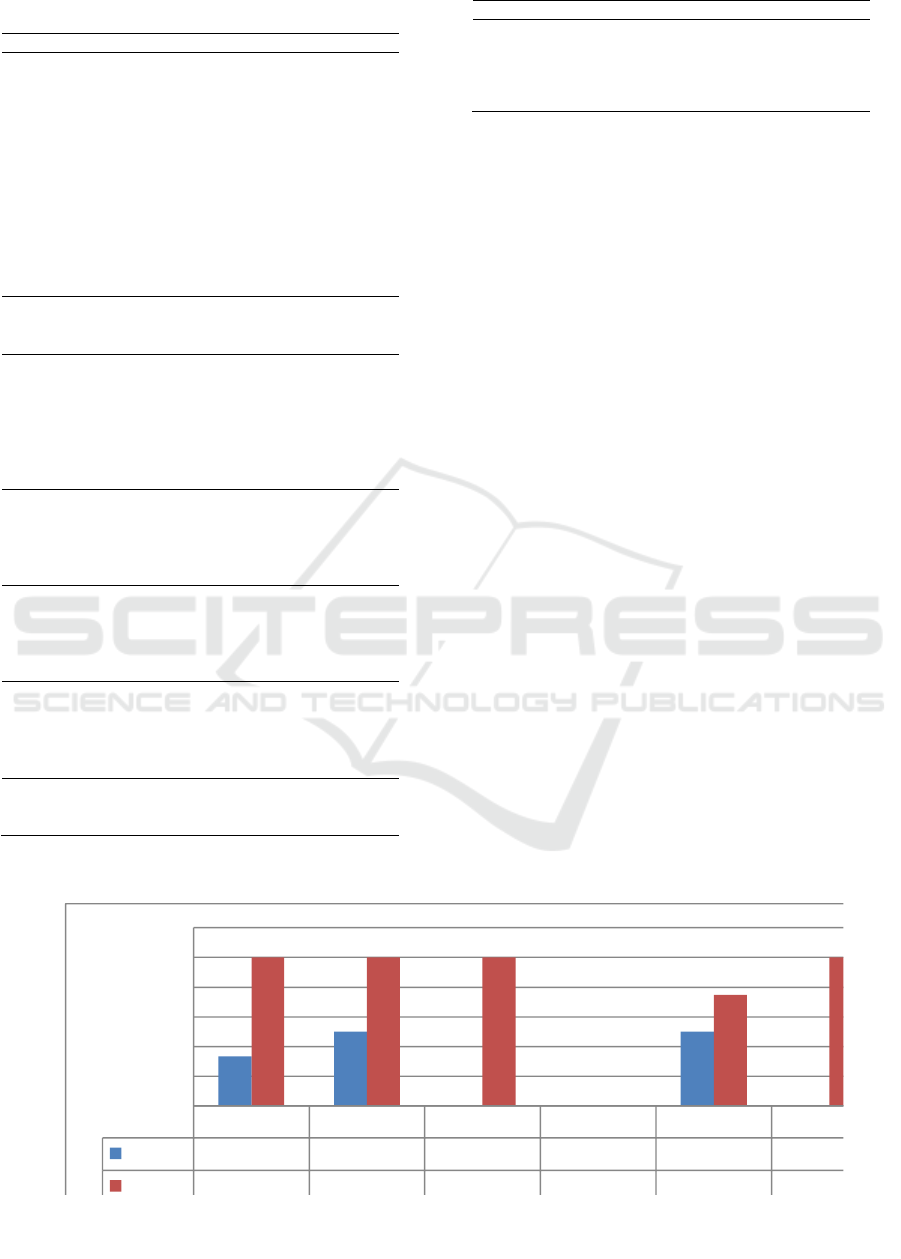
Table 1: Program Session(s) & Objective(s)
Session
Objective
Pre-test &
Program
Orientation
The gather subject's baseline level of
emotion regulation skill in respect to
behavior indicator.
To familiarize subject with the
intervention setting, signing contract
containing rules to be respected by
the client
To teach the mother and teacher
about the program, including
objectives, activities, and materials.
The behavioral checklist is also
explained to be further filled by
them.
Session 1
To review the rules of learning
To identify the types of basic
emotions
Session 2
To review the previous session
material
To review the homework given
To identify the emotions participant
feel in real situation
To understand the process of
emotion formation
Session 3
To review the previous session
material
To review the homework given
To manage the negative emotions
experience
Session 4
To review the previous session
material
To review the homework given
To know how to improve positive
emotions
Session 5
To review the previous session
material
To review the homework given
To know the vulnerability factor in
the process of emotion regulation
Post-test 1
The gather subject's attainment of
emotion regulation skill in respect to
behavior indicator.
Session
Objective
Post-test 2
The seek out if the subject's
attainment of emotion regulation
skill in respect to behaviour indicator
is intact
3 RESULTS
The Figure 1 is that summarizes the differences of
client's percentage on achievement score before and
after the intervention related to the behaviour
indicator.
From the graph, we can see that there are
differences in subject's achievement percentage
score of emotional regulation skill before and after
intervention conducted. Prior to the intervention,
subject obtains a total score of 9 out of 27 with the
resulting percentage of 33.33%. While in post-test,
subject gets the score of 24 which mean that she gets
a percentage of 88.89%. Therefore, there is an
increase in the percentage score by 55.56%, which
indicate that there is an increase in subject level of
emotion regulation skill. The data obtained shows
that the increase occurs on five out of six program
objectives.
4 DISCUSSION
Charlton and Dykstra (2011) revealed that language
adaptation in the implementation of the DBT is a
must so that subject with intellectual disability can
easily understand the learning lesson and then apply
the knowledge. In this study, language adaptation
becomes one of the keys in enabling the subject to
capture the information provided by researcher.
Indicator 1
Indicator 2
Indicator 3
Indicator 4
Indicator 5
Indicator 6
Pretest
33.33
50
0
0
50
0
Postest
100
100
100
0
75
100
0
20
40
60
80
100
120
Percentage
Figure 1: Comparison of Client Percentage Score Before and After the Intervention
ICP-HESOS 2018 - International Conference on Psychology in Health, Educational, Social, and Organizational Settings
356

Some examples of language adaptation are
"emotions" as "feelings," "emotional regulation," as
"regulating feelings," "actions" as "what to do," and
so on. The selected word is chosen from the
preliminary observation of client's vocabulary
repertoire. Thus, the creativity of the researcher in
determining the right vocabulary to convey the
lesson in accordance with the material is crucial.
Charlton and Dykstra (2011) argues that content
in the program should be as relevant as possible to
the daily life of the clients to facilitate their
application of the skill taught. Bailie and Slater
(2014) added that the intervention program should
relate the new information provided to what was
previously known by the client. In this program, the
overall content reviewed is specifically tailored to
the subject's daily life. For example, a case study of
a person being scolded by parents, ridiculed by
friends, and travelling to Bali are given; where they
are all known as situations that cause the subject to
experience certain emotional reaction. For that
purpose, collecting baseline data before the delivery
of program becomes important to determine which
case should be raised in the program. The suitability
between the case raised and the subject previous
experiences makes it easy to draw the subject's
attention to the material and to gain understanding.
Lew, Tripp-Tebo, and Watts (2006) mentioned
that materials in the intervention program need to be
tailored to attract the attention of clients. Given the
condition of the client is not able to read yet, the
material in then given by using images with various
colours. The use of image builds the impression of a
fun learning process to the client, and makes it easy
for her to identify and associate the images with
explanations given by the researcher about the
meaning. Furthermore, the attractiveness is enforced
through the inclusion of self and family portraits in
the instrument. It becomes easier for subject to
recognize the image and she can immediately
associate between what she knows based on her
experience with the material provided. In addition,
the use of self and family portrait makes the subject's
learning process in line with the individual approach
which is advisable in the educational process for
individuals with special needs (Mangunsong, 2009).
Repetition of material to subject with intellectual
disabilities is important and also forms the structure
of the overall implementation of intervention
(Charlton and Tallant, 2003 in Charlton and Dykstra,
2011). Furthermore, repetition is also one of the
main principles in teaching individual with
intellectual disabilities (Hallahan and Kaufman,
2006) related to their characteristic of memory
deficiency. Throughout the program, the repetition
of the material that has been learned is done in each
session. On the other hand, the subject complained
several times that she was bored with the repetition
because she already knew about the material. In this
case, we see that the process of review of the
material needs to be done with a variety of
activities/methods to foster the motivation of the
client in order to avoid boredom.
Limitation of this study lies in the physical
condition of the subject who had shown the
symptoms of sickness in the final session of the
program. In respect to the failure of practicing the
act of managing negative emotion (using stop-think-
relax method), the main constraint lies in the nature
of the stop-think-relax technique. This technique
requires optimal physical condition for the
individual who practice it. During the program,
subject finds it difficult to practice relax techniques-
in which she needs to inhale and exhale deeply –
since she has cold. Therefore, attention to the
physical condition of the subject for program
implementation becomes crucial. In addition,
considering another type of negative emotion
regulating techniques is advisable. As a note, the
technique should be concrete enough and easily
implemented by the individual in respect to their
disability (Mangunsong, 2009).
5 CONCLUSIONS
This study aims to test the effectiveness of
Dialectical Behaviour Therapy in improving the
emotion regulation skill in adolescents with
intellectual disability. Based on the result obtained,
we see that the program is effective to improve the
client's emotion regulation skill based on the
behaviour indicator. Through observation made on
the subject's behaviour after the program, it was
found that the program succeeded in providing new
knowledge to the subject about the benefits of
excelling in emotion regulation skill, the types of
emotions, the process of emotion emergence, the
procedure for managing negative emotions, the
activities to induce positive emotions, and factors
affecting emotion regulation. Furthermore, the
program also succeeds in changing the views or
attitudes of the subject regarding the importance of
managing emotions in everyday life, especially in
terms of changing bad habits that foster vulnerability
for experiencing negative emotions. Nevertheless,
further tracking is required to seek out if the
program is successful in altering the actual
The Effectiveness of Dialectical Behavior Therapy in Developing Emotion Regulation Skill for Adolescent with Intellectual Disability
357

behaviour of the subject to regulate the negative
emotion using the techniques taught.
ACKNOWLEDGEMENTS
This study cannot be successfully done without the
support of Sekolah Luar Biasa Ulaka Penca for
giving the required time and place to conduct the
intervention to the client. Cooperation displayed by
the subject's family member is also the main factor
for the subject's successful completion of the
program. To further clarify, this research received
no specific grant from any funding agency,
commercial or not-for-profit sectors.
REFERENCES
Baillie, A. and Slater, S., 2014. Community dialectical
behaviour therapy for emotionally dysregulated
adults with intellectual disabilities. Advances in
mental health and intellectual disabilities, 8(3),
pp.165-173.
Barnicot, K., Gonzalez, R., McCabe, R. and Priebe, S.,
2016. Skills use and common treatment processes
in dialectical behaviour therapy for borderline
personality disorder. Journal of behavior therapy
and experimental psychiatry, 52, pp.147-156.
Baurain, C. and Nader-Grosbois, N., 2012. Socio-
emotional regulation in children with intellectual
disability and typically developing children in
interactive contexts. ALTER-European Journal of
Disability Research/Revue Européenne de
Recherche sur le Handicap, 6(2), pp.75-93.
Berking, M. and Schwarz, J., 2014. Affect regulation
training. Handbook of emotion regulation, 2.
Blackwell, M.W. 1979. Care of the Mentally Retarded.
Little, Brown, and Company. USA.
Charlton, M. and Dykstra, E.J., 2011. Dialectical
behaviour therapy for special populations:
Treatment with adolescents and their caregivers.
Advances in mental health and intellectual
Disabilities, 5(5), pp.6-14.
Denham, S.A., Bassett, H., Mincic, M., Kalb, S., Way, E.,
Wyatt, T. and Segal, Y., 2012. Social–emotional
learning profiles of preschoolers' early school
success: A person-centered approach. Learning
and individual differences, 22(2), pp.178-189.
Eisenhower, A.S., Baker, B.L. and Blacher, J., 2007. Early
student–teacher relationships of children with and
without intellectual disability: Contributions of
behavioral, social, and self-regulatory competence.
Journal of school psychology, 45(4), pp.363-383.
Espelage, D.L., Rose, C.A. and Polanin, J.R., 2015.
Social-emotional learning program to reduce
bullying, fighting, and victimization among middle
school students with disabilities. Remedial and
special education, 36(5), pp.299-311.
Farb, N.A., Anderson, A.K., Irving, J.A. and Segal, Z.V.,
2014. Mindfulness interventions and emotion
regulation. Handbook of emotion regulation,
pp.548-567.
Gravetter, F.J. and Forzano, L.A.B., 2018. Research
methods for the behavioral sciences. Cengage
Learning.
Graziano, P.A., Reavis, R.D., Keane, S.P. and Calkins,
S.D., 2007. The role of emotion regulation in
children's early academic success. Journal of
school psychology, 45(1), pp.3-19.
Gross, J.J. 2014. Handbook of emotion regulation. The
Guilford Press.
Gross, J.J and Thomson, R.A. 2007. Emotion regulation:
Conceptual foundations. Handbook of Emotion
Regulation . The Guilford Press.
Gumora, G. and Arsenio, W.F., 2002. Emotionality,
emotion regulation, and school performance in
middle school children. Journal of school
psychology, 40(5), pp.395-413.
Hallahan, D.P. and Kaufman, J.P. 2006. The exceptional
learner: Introduction to special education.
Pearson Education.
Hauser-Cram, P., Krauss, M.W. and Kersh, J., 2004.
Adolescents with developmental disabilities and
their families. Handbook of adolescent
psychology, 1, pp.589-617.
Lew, M., Matta, C., Tripp-Tebo, C. and Watts, D., 2006.
Dialectical behavior therapy (DBT) for individuals
with intellectual disabilities: A program
description. Mental health aspects of
developmental disabilities, 9(1), p.1.
Linehan, M. M. 1993. Cognitive-behavioral treatment of
borderline personality disorder. Guilford Press.
Mangunsong, Frieda. 2009. Psikologi dan pendidikan
anak berkebutuhan khusus. LPSP3.
MacLeod, C. and Grafton, B. 2014. Affect regulation
training. Handbook of emotion regulation. The
Guilford Press.
McKay, M., Wood, J.C. and Brantley, J., 2010. The
dialectical behavior therapy skills workbook:
Practical DBT exercises for learning mindfulness,
interpersonal effectiveness, emotion regulation
and distress tolerance. New Harbinger
Publications.
McWilliams, J., de Terte, I., Leathem, J., Malcolm, S. and
Watson, J., 2014. Transformers: a programme for
people with an intellectual disability and emotion
regulation difficulties. Journal of intellectual
disabilities and offending behaviour, 5(4), pp.178-
188.
Mennin, D.S. and Fresco, D.M. 2014. Emotion regulation
therapy. Handbook of emotion regulation. The
Guilford Press.
Njardvik, U., Matson, J.L. and Cherry, K.E., 1999. A
comparison of social skills in adults with autistic
disorder, pervasive developmental disorder not
otherwise specified, and mental retardation.
ICP-HESOS 2018 - International Conference on Psychology in Health, Educational, Social, and Organizational Settings
358

Journal of autism and developmental disorders,
29(4), pp.287-295.
O’Brennan, L.M., Waasdorp, T.E., Pas, E.T. and
Bradshaw, C.P., 2015. Peer victimization and
social-emotional functioning: a longitudinal
comparison of students in general and special
education. Remedial and special education, 36(5),
pp.275-285.
Papalia, D.E., Olds, S.W., and Feldman, R.D. 2010.
Human development. The McGraw-Hill
Companies
Pereira, C.M.G. and de Matos Faria, S.M., 2015. Do you
feel what I feel? Emotional development in
children with ID. Procedia-Social and behavioral
sciences, 165, pp.52-61.
Saarni, C., Campos, Camras, J., and Withering, D. 2006.
Emotional development: Action communication
and understanding. Handbook of Child
Psychology. Wiley. N
Sakdalan, J.A., Shaw, J. and Collier, V., 2010. Staying in
the here‐and‐now: A pilot study on the use of
dialectical behaviour therapy group skills training
for forensic clients with intellectual disability.
Journal of intellectual disability research, 54(6),
pp.568-572.
Soler, J., Pascual, J.C., Tiana, T., Cebrià, A., Barrachina,
J., Campins, M.J., Gich, I., Alvarez, E. and Pérez,
V., 2009. Dialectical behaviour therapy skills
training compared to standard group therapy in
borderline personality disorder: a 3-month
randomised controlled clinical trial. Behaviour
research and therapy, 47(5), pp.353-358.
Wiltz, J.P., 2005. Identifying factors associated with
friendship in individuals with mental retardation
(Doctoral dissertation, The Ohio State University).
The Effectiveness of Dialectical Behavior Therapy in Developing Emotion Regulation Skill for Adolescent with Intellectual Disability
359
