
Coaching Improving Self-efficacy to Perform Salat (Muslim Prayer)
Among Muslim Patients in Hospital
Hamdan Hariawan
1
, Oedojo Soedirham
2
and Abu Bakar
1
1
Faculty of Nursing, Universitas Airlangga, Kampus C Jl. Mulyorejo Surabaya, Indonesia
2
Faculty of Public Health, Universitas Airlangga, Surabaya, Indonesia
Keywords: Coaching, Self-efficacy, Salat (muslim prayer).
Abstract: Background: Hospitalization and weakness, attached medical equipment and lack of konowledge can
decrease patients self efficacy to perform salat (muslim prayer) as spiritual needs. The purpose of this study
was to determine the effect of individual coaching in improving self effecacy to perform salat among
muslims patient in hospital. Methods: This study was used quasy experiment method. The samples were 36
hospitalized muslim patients. Data were collected by self-constructed questionnaire based on Prayer-based
self eficacy scale. Data were analysed using Independent t-test with α ≤ 0.05. Results: Before giving the
intervention, the means of pretest self-efficacy score in both groups were 24,72+2,67 and 25,06+2,34. There
is no significant difference of self efficacy scores between two groups before intervention (P=0,693). After
giving intervention, these scores have changed to 28,11+2,93 and 24,94+1,83, and there is higher
significance of self efficacy scores after giving intervention (P=0,000). Conclusions: Coaching is suitable
methode to increase patients ability and self efficacy to perform salat. It was recommended to nurses in
hospital to do coaching as nursing intervention to increase patients self efficacy to perform salat as spiritual
needs of muslim patients.
1 BACKGROUND
Hospitalized patients tend to have an unstable
psychic condition and feel unmet spiritual needs
during the treatment. Since 1998, psychic and
spiritual needs are in the second place in the
National Inpatient Priority Index (Gallison et al.
2013). One of patient’s spiritual needs is how they
are able to carry out religious practice (Kurniawati
2017). Salat is an obligatory worship for every
Muslim. Salat (muslim prayer) must be performed
five times every days in both sick and healthy
conditions (Mohamed et al. 2015).
Salat is a religious practice which is performed
by moving certain limbs. Movements in salat is
certain movements in accordance with the guidelines
for Muslims. Before performing salat, a Muslim
should perform ablution first. Ablution is washing
parts of particular body with water. In addition to
obtain a valid salat, the body and clothing as well as
the place of salat should be clean and sacred (Akgül
and Karadaǧ 2016).
Patient in a poor conditions and attached medical
devices lead to doubts and inability to perform salat
(Al-Obaidi et al., 2012; Akgül and Karadaǧ, 2016).
In addition, patients sense in an unholy condition so
they unable to perform salat can be a lesser form of
self-efficacy. Hospitalized patients with physical
weakness will experience a decrease in self-efficacy,
such as the physical weakness after surgery. Patients
who have low self-efficacy levels cause themselves
to consider they are not able to do something useful
or feel less productive due to illness. The failure of
self-efficacy has been shown to influence an
individual's decision to conduct self-care behavior.
A change of behavior will only occur if there is a
change in the individual's self-efficacy (D’Souza et
al. 2017).
According to Aris et al., (2017) research, there
are more than half patients (53.6%) had low
knowledge about how to perform salat in hospital
during illness. Low knowledge can also be the cause
of lack of self-efficacy. Provision of education as a
form of verbal persuasion by explaining how to pray
during illness can be a solution of self-efficacy
improvement. Salat has a specific way to be
performed in a certain conditions called rukhsoh,
such as salat by sitting if unable to stand or lie down
442
Hariawan, H., Soedirham, O. and Bakar, A.
Coaching Improving Self-efficacy to Perform Salat (Muslim Prayer) Among Muslim Patients in Hospital.
DOI: 10.5220/0008326504420445
In Proceedings of the 9th International Nursing Conference (INC 2018), pages 442-445
ISBN: 978-989-758-336-0
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
if unable to sit. The movement in salat can be
performed according to the patient's ability and can
be performed in certain unavoidable conditions such
as the place of salat is not clean (Hafiz J et al. 2016).
One form of education that can be given is
coaching. Coaching not only exposes the material,
but also teaches and do practices so the patient can
immediately practice the prayer movement in their
ability. The results of the study on the use of
coaching in some previous researches may address
existing clinical and community problems by
improving patient self-efficacy, affecting adherence,
increasing knowledge of health and self care
behavior, and improving quality of life (Bennett et
al., 2009; Vanacker et al., 2017; Wagner et al.,
2017). The purpose of this study was to determine
the effect of individual coaching in improving self
efficacy to perform salat among muslims patient in
hospital.
2 METHODS
This study was used quasy experiment method with
pre-post with control group design. The samples
were 36 hospitalized muslim patients and sample is
selected and divided in intervention and control
groups by simple random sampling. The size of both
groups are same. The independent variable was
individual coaching, while the dependent variable
was self efficacy. Coaching in this research consists
of 5 stages. The first, fourth and fifth stages
including assessmant, personal support and
evaluation are given by nurse, while the second and
third stage are provision of education and practice of
performing salat during illness are given by the
hospital's guidance counselor.
Data were collected by self-developed
questionnaire. The questionnaire was developed
based on prayer-based self efficacy which is
consisting preparation for salat, performance of
ablution, and performance of salat. The reliability of
this questionnaire was calculated using Cronbach
Alpha value of 0,557. Data were analysed by using
Independent t test with α ≤ 0.05. This study was
approved by Rumah Sakit Umum Daerah Provinsi
NTB Ethical Committee number 070/01/KEP/2018.
3 RESULTS
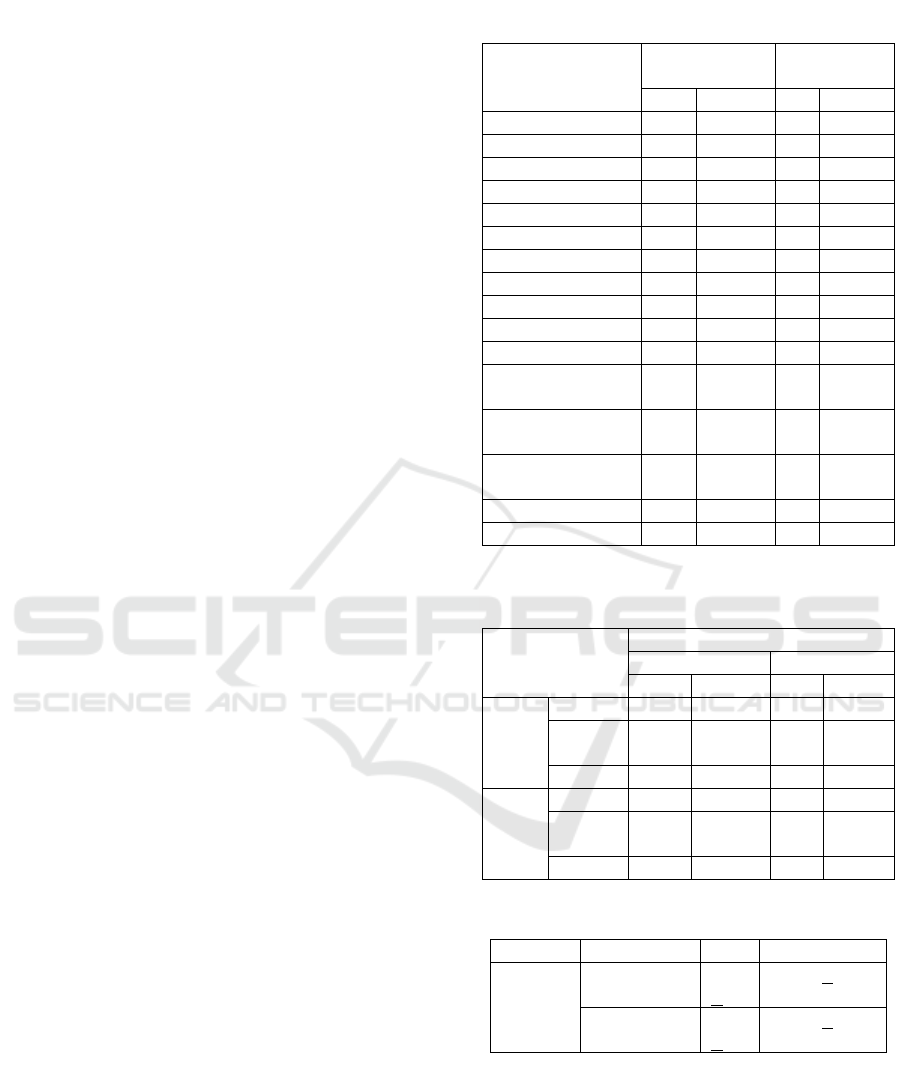
Table 1 shows that both groups have more male
respondents than female. The ages of respondents
are varies, but most respondents are 36-45 years old.
Last education of respondents also varies.
Based on Table 2, there are 94,44% respondents
in intervention group had strong self efficacy and
5,56% had very strong self efficacy, all respondents
in control group had strong self efficacy before
intervention given to them. After respondents being
given coaching, self efficacy in intervention group
Table 1: Distribution of respondents.
Characteristics
Intervention
Group
Control
Group
%
%
Gender
Male
14
77,8
12
66,7
Female
4
22,2
6
33,3
Total
18
100
18
100
Age
26-35 years old
4
22,2
1
5,6
36-45 years old
8
44,4
8
44,4
46-55 years old
1
5,6
6
33,3
55-65 years old
5
27,8
3
16,7
Total
18
100
18
100
Last Education
Elementary
School
5
27,8
7
38,9
Junior High
School
6
33,3
6
33,3
Senior High
School
6
33,3
4
22,2
Bachelor
1
5,6
1
5,6
Total
18
100
18
100
Table 2: Self-efficacy before and after
intervention.
Self efficacy
Groups
Intervention
Control
%
%
Pre
test
Strong
17
94,44
18
100
Very
strong
1
5,56
-
-
Total
18
100
18
100
Post
test
Strong
15
83,33
18
100
Very
strong
3
16,67
-
-
Total
18
100
18
100
Table 3: Score of Self-efficacy in both groups.
Variable
Groups
Pre
Post
Self
Efficacy
Intervention
24,7
+2,6
28,11+2,93
Control
25,1
+2,3
24,95+1,83
Coaching Improving Self-efficacy to Perform Salat (Muslim Prayer) Among Muslim Patients in Hospital
443

became strong by 83,33% and 16,67% were in very
strong self efficacy, there is no change in control
group.
Table 3 shows the average score of self efficacy
in both groups. Before get intervention, control
group had higher mean (24,7) of self efficacy score
than intervention group (25,1). After get
intervention, the mean score of self efficacy higher
(28,11) than before (24,7), and also higher (28,11)
than control group (24,95).
Results of statistical tests using independent t-
test in both groups before giving intervention was
p=0,693, and after giving intervention was p=0,000.
Based on test result after giving intervention, there
was difference of self-efficacy in both groups. The
defference indicated that coaching affecting self-
efficacy to perform salat.
4 DISCUSSION
In this research, self-efficacy score based on gender
and age on each respondent are varies. This is not in
line with the theory of Bandura (1997) which states
that olders tend to have more time and experience in
overcoming something that happens when compared
with younger individuals. It can be caused by last
education of respondents. In this study the most last
education of respondents are high schools and the
average category of respondent’s self-efficacy are in
a strong category. Self-efficacy can be formed
through the learning process and formal education is
one of ways in learning process. The individual has
a high self-efficacy according their length in
learning.
Before the intervention, the average score of
intervention group was 24.72 with 17 respondents
had strong self-efficacy and 1 respondent had very
strong self-efficacy. This can be seen from the
average of answers “confident” and “very confident”
of respondents to their ability to perform salat in a
sitting or lying position, and there are some still
confident the obligation to perform salat during
illness. Some respondents also answer “confident”
that family can help them in performing salat. This
can be influenced by the information gained on how
to perform salat during illness that obtained from
religious studies or religious community. It can also
be obtained from the experience of others and the
support of family members during hospitalization.
After the intervention, the average score of the
intervention group was 28.11 with 15 respondents
had a strong self-efficacy and 3 respondents had
very strong self-efficacy. Increased self-efficacy can
occur due to increased confidence in the obligation
to perform salat in every condition and increased
confidence in the ability to perform salat as their
ability. While in the control group, there was no
increase in self-efficacy. All control groups had an
average self-efficacy score was 24.72 with a strong
self-efficacy.
Based on the statistical test, it can be stated that
the provision of coaching can improve self-efficacy
significantly. Coaching in this research consists of 5
stages. The second and third stage are provision of
education and practice of performing salat during
illness are given by the hospital's guidance
counselor. the results of this study are in line with
several other studies such as the study of health
coaching on self efficacy and the study of wellness
coaching in improving self efficacy (Eom and Lee
2017; Dejesus et al. 2018)
The research of the effect of health coaching
program on self-efficacy, health behavior and
quality of life in hypertensive people in poverty
resulted in a significant effect on improving self-
efficacy. Eom and Lee (2017) stated in his research
that health coaching is the right strategy to improve
patient’s self-efficacy to continue maintaining their
health behavior. The results of this study are also in
line with research conducted by Dejesus et al.
(2018) that wellness coaching can improve self-
efficacy. Self-efficacy can be improved because
coaching enhances positive motivation and patient
beliefs about their abilities. In addition, coaching
also makes patients and coaches have regular
schedule to meet and provide materials and training
that can improve the motivation and ability of
patients.
See et al. (2014) in his research stated that
education which is provided personally to
hospitalized patients with the right material can
improve the patient’s self-efficacy to be able to
recognize and report symptoms of adverse
conditions that can be experienced by patients.
Education is part of health coaching that can meet
the verbal persuasion in order to improve self-
efficacy. Bandura (1997) states that the individuals
can gain influence or suggestion so they are able to
overcome the problems they faced. Verbal
persuasion can be given by influential people such
as family and experts such in this research is the
religious leaders so that patients will be more
confident about salat. A person who is always given
the belief and drive to succeed, then will show the
behavior to achieve that success. The focus of
coaching includes factors that influence motivation,
overcome obstacles, limit the disability of the
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
444

patient, influence patients to not limit themselves,
produce solutions, support, build self-efficacy, and
how patients become more involved in decision
making (Macadam 2013).
Increased self-efficacy after given intervention
can occur due to increased patients confidence in the
obligation to perform prayers and increased patients
confidence in their ability to perform prayers even in
sick condition. This can be achieved due by
individual coaching, because coaching which was
given including providing information, training
patients to perform prayers during hospitalization,
helping patients to overcome barriers in performing
salat, and motivating patients.
5 CONCLUSIONS
There was an improvement of self-efficacy to
perform salat in illness condition after given
individual coaching. Coaching not only emphasizes
the cognitive aspects of the patient, but also on the
affective and psychomotor aspects and it is suitable
methode to increase their ability and self-efficacy to
perform salat. It was recommended to nurses in
hospital to do coaching as nursing intervention to
increase patients self-efficacy to perform salat as
spiritual needs of muslim patients
REFERENCES
Akgül, Betül, and Ayişe Karadaǧ. 2016. “The Effect of
Colostomy and Ileostomy on Acts of Worship in the
Islamic Faith.” Journal of Wound, Ostomy and
Continence Nursing 43(4): 392–97.
Al-Obaidi, Saud, James C. Wall, Madhuri S. Mulekar, and
Rebecca Al-Mutairie. 2012. “The Reliability of
Prayer-Based Self-Efficacy Scale to Assess Self-
Confidence of Muslims with Low Back Pain.”
Physiotherapy Research International 17(2): 110–20.
Aris, Muhammad Shamsir Mohd et al. 2017. “Knowledge,
Attitude, and Practice of Performing Prayers (Salat)
among Muslim Patients in Hospital Langkawi, Kedah:
Roles of Muslim Healthcare Providers.” Advanced
Science Letters 23(5): 4955–59.
Bandura, Albert. 1997. Self-Efficacy. New York: Freeman.
Bennett, Heather et al. 2009. “The Effectiveness of Health
Coaching, Home Blood Pressure Monitoring, and
Home-Titration in Controlling Hypertension among
Low-Income Patients: Protocol for a Randomized
Controlled Trial.” BMC Public Health 9(1): 456.
http://bmcpublichealth.biomedcentral.com/articles/10.
1186/1471-2458-9-456.
D’Souza, Melba Sheila et al. 2017. “Self-Efficacy and
Self-Care Behaviours among Adults with Type 2
Diabetes.” Applied Nursing Research 36: 25–32.
http://dx.doi.org/10.1016/j.apnr.2017.05.004.
Dejesus, Ramona S et al. 2018. “Impact of a 12-Week
Wellness Coaching on Self-Care Behaviors among
Primary Care Adult Patients with Prediabetes.”
Preventive Medicine Reports:
https://doi.org/10.1016/j.pmedr.2018.02.012.
Eom, Sun Ok, and Insook Lee. 2017. “The Effect of
Health Coaching Programs on Self-Efficacy , Health
Behaviors , and Quality of Life in.” J Korean Acad
Nurs 47(3): 380–91.
Gallison, Barry S., Yan Xu, Corrine Y. Jurgens, and
Suzanne M. Boyle. 2013. “Acute Care Nurses
Spiritual Care Practices.” Journal of Holistic Nursing
31(2): 95–103.
Hafiz J, Dzulkhairi, Shamsir MA, and Abu NA. 2016.
“Knowledge , Attitude and Practice towards Religious
Obligations among Healthcare Workers in Hospital.”
The International Medical Journal Malaysia 15(2): 3–
6.
Kurniawati, Ninuk Dian. 2017. “Mind-Body-Spiritual
Nursing Care in Intensive Care Unit.” Advances in
Health Sciences Research 3(Inc): 223–28.
Macadam, Catherine. 2013. “Health Coaching – a
Powerful Approach to Support Self-Care.”
http://www.selfcareforum.org/wp-
content/uploads/2014/08/Health-Coaching-how-it-can-
support-Self-Care.pdf.
Mohamed, Che Rabiaah, Katherine Nelson, Pamela Wood,
and Cheryle Moss. 2015. “Issues Post-Stroke for
Muslim People in Maintaining the Practice of Salat (
Prayer ): A Qualitative Study.” Collegian 22(3): 243–
49. http://dx.doi.org/10.1016/j.colegn.2014.01.001
See, Min Ting Alicia et al. 2014. “Effectiveness of a
Patient Education Intervention in Enhancing the Self-
Efficacy of Hospitalized Patients to Recognize and
Report Acute Deteriorating Conditions.” Patient
Education and Counseling 97(1): 122–27.
http://dx.doi.org/10.1016/j.pec.2014.07.003.
Vanacker, P. et al. 2017. “An Individualized Coaching
Program for Patients with Acute Ischemic Stroke:
Feasibility Study.” Clinical Neurology and
Neurosurgery 154: 89–93.
Wagner, Kelly A. et al. 2017. “Dietary Intervention for
Glucose Tolerance In Teens (DIG IT): Protocol of a
Randomized Controlled Trial Using Health Coaching
to Prevent Youth-Onset Type 2 Diabetes.”
Contemporary Clinical Trials 53: 171–77.
http://dx.doi.org/10.1016/j.cct.2016.12.018.
Coaching Improving Self-efficacy to Perform Salat (Muslim Prayer) Among Muslim Patients in Hospital
445
