
The Correlation between Self-efficacy and Quality of Life in Elderly
Who are Living with Hypertension
Maria Manungkalit and Linda Juwita
Faculty of Nursing, Widya Mandala Catholic University, Jl. Raya Kalisari Selatan 1, Pakuwon City, Surabaya, Indonesia
Keywords: Elderly, Hypertension, Quality of life, Self-efficacy.
Abstract: The prevalence of hypertension was found to be high in the elderly globally. Self-efficacy plays an
important role in the initiation and maintenance of health behavior, thus has an impact in determining
quality of life (QOL). This study aimed to analyze the correlation between self-efficacy and QOL in elderly
who are living with hypertension. This was a correlational study by using cross-sectional design approach.
The population was all elderly with hypertension live in nursing home of St. Yosef Surabaya, amounting to
70 people. Sample size was 45 selected by purposive sampling technique. The independent variable was
self-efficacy measured by General Perceived Self-Efficacy instrument (α=.785, r=.447-.745). Dependent
variable was QOL measured by WHOQOL-BREF instrument (α=.700, r=.419-.798). Data analysis used
Spearman Rank correlation test (α=.05). Result showed that majority was female (57.78%), 75-90 years old
(55.56%), primary school graduated (40%), and had a family history of hypertension (82.22%). Most
respondent had sufficient self-efficacy (82.22%) with no low self-efficacy was found, and had sufficient
QOL (73.33%) with no high QOL was found. Self-efficacy was not correlated with QOL in elderly who are
living with hypertension (p=.456). Various factors influenced the elderly’s QOL, such as independency
level, family support, socio-economic status, living standard, and culture.
1 BACKGROUND
Every individual will experience and face the aging
process in the course of his life and this is a natural
process that cannot be avoided. Being elderly is a
process that takes place in life means someone has
gone through the stages of life, namely neonatal,
toddler, pre-school, school, adolescent, adult, and
the elderly. This different stage of life begins both
biologically and psychologically (Padila, 2013).
Gradually, the elderly will experience changes in the
ability of various organs, functions, and body
systems that are natural / physiological. With many
changes that occur in the elderly, elderly faces many
problems, one of that is the increase of blood
pressure (hypertension). Epidemiological
investigations have shown that the occurrence of
hypertension is closely related to morbidity and
mortality of cardiovascular disease (Mutaqqin,
2009). Some studies concluded that age is also one
factor in the occurrence of hypertension because the
increased age of a person will increase the risk of
hypertension. Hypertension is an increase in systolic
blood pressure of at least 140 mmHg or diastolic
pressure of at least 90 mmHg (Price & Wilson,
2006).
According to the data of Ministry of Health
(MOH), Republic of Indonesia (RI) in 2014, there
was an increase in number of elderly who had
hypertension about 50%. The incidence of
hypertension in East Java in 2013 was 26.2%.
According to data of the Health Departement of
Surabaya, number of hypertension cases in 2014 as
much as 19.56% (Basic Health Research, 2013).
The incidence of elderly with hypertension is
caused by many factors that are closely related to the
natural aging process. In elderly, structural and
functional changes occur in the peripheral vessel
system resulted in changes in blood pressure. These
changes include atherosclerosis, loss of elasticity of
connective tissue, and a decrease in relaxation of
smooth muscle of blood vessels which in turn
decreases the ability of distention and tensile
strength of blood vessels (Brunner & Suddarth,
2002). Complications will also occur in people with
hypertension, such as coronary heart disease, heart
failure, brain blood vessel damage, and kidney
failure (Corwin, 2009).
Manungkalit, M. and Juwita, L.
The Correlation between Self-efficacy and Quality of Life in Elderly Who are Living with Hypertension.
DOI: 10.5220/0008326004130417
In Proceedings of the 9th International Nursing Conference (INC 2018), pages 413-417
ISBN: 978-989-758-336-0
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
413
Along with the increasing number of prevalence
of hypertension incidence and complication of the
disease, these will also impact on the QOL where
the individual needs to make adjustments in order to
remain able to perform its function optimally.
Xavier, et al., (2003) concluded that elderly with
poor QOL was equivalent to low health status, and
good QOL was equivalent to good health status,
more variety of activities, social life and good family
relationships. Therefore health status is one of the
good indicators of QOL in elderly. QOL reflects
how one sees himself about his satisfaction of life
(Philips, et al., 2009).
The QOL of elderly can be influenced by level of
independence as well. The success of self-reliance is
not only related to health care, but also maximizing
the psychological resources, such as self-efficacy,
resilience, increased precautions, medical
management during sick and illness, lifestyle
changes by doing things that have a positive effect
on health.
Self-efficacy theory was developed by Albert
Bandura as a cognitive social theory in 1977. He
defined self-efficacy as a decisive belief in how one
thinks, motivates himself and how one ultimately
decides to conduct a behavior to achieve the desired
goal. A study of Luszczynska's & Dona (2005) about
general self-efficacy suggested that self-efficacy can
predict compliance in treatment regimens, health
behaviors, physical activity, effective pain
management, and disease management.
This study aimed to analyze the correlation
between self-efficacy and QOL in elderly who are
living with hypertension.
2 METHODS
This study utilized cross-sectional design. The
population was all elderly with hypertension in St.
Yosef elderly home of Surabaya which amounted to
70 people. Sample size was 45, selected by
purposive sampling. Sample criteria were medical
diagnosis was confirmed by a physician, duration of
hypertension at least one month, willing to
participate, and cooperative. Independent variable
was is self-efficacy measured by instrument of
General Perceived Self-efficacy developed by
Bandura (1986) (α=.785, r=.447-.745). It consisted
of 10 items examined by 1-4 Likert scale. The
category of self-efficacy was low (score of 10-20),
sufficient (score of 21-30), and high (score > 30).
While the dependent variable was QOL measured by
WHOQOL-BREF developed by World Health
Ofrganization (WHO, 2004) (α=.700, r=.419-.798).
It consisted of 4 items assessing 4 domains of QOL,
such as, physical, psychological, social, and
environmental. Raw score in each domain was
transformed into 0-100 range. The category of QOL
was low (score of 0-40), sufficient (score of 41-69),
and high (score of 70-100). All data was in ordinal
scale, so that Spearman Rank correlation test was
used for data analysis (α < .05). Ehical aspect was
assured by principal of anonimity, beneficence, non-
maleficence, fidelity, and confidentialty
implemented in this study. Informed consent was
signed by all respondents.
3 RESULTS
There were 45 elderly with hypertension who are
living in an elderly home of St. Yosef of Surabaya
participated in this study. Age range was 66 – 97
years old. Most respondents were female (57.78%),
75-90 years old (55.56%), primary school graduated
(40%), and had a family history of hypertension
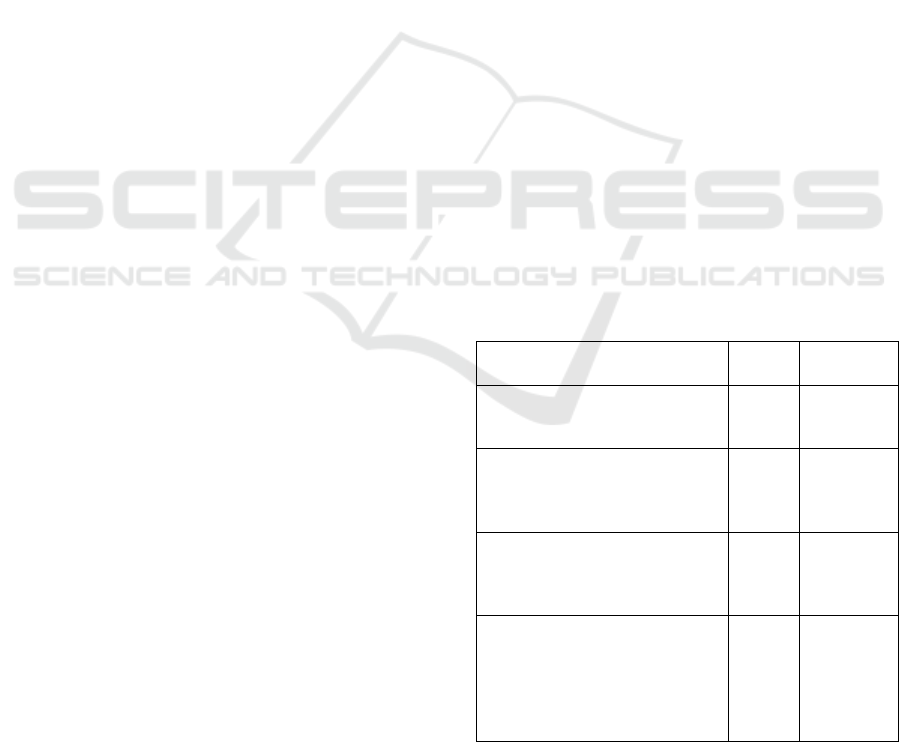
(82.22%). Table 1 explains demography
characteristic of study respondents.
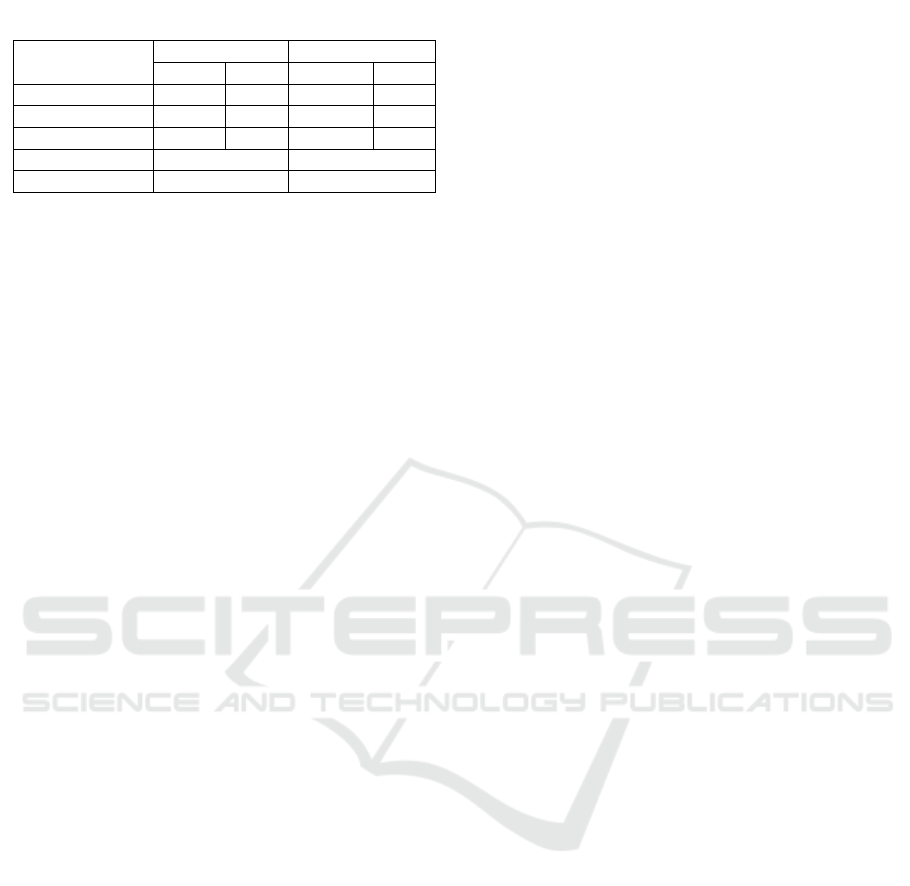
Most respondents had sufficient self-efficacy
(82.22%) and sufficient QOL (73.33%). Self-
efficacy was uncorrelated with QOL in elderly with
hypertension (p = .456). Table 2 explains the result
of descriptive statistical analysis.
Table 1: Demography characteristic.
Characteristic n %
1. Sex
a. Male
b
. Female
19
26
42.22
57.78
2. Age (years old)
a. 60-74
b. 75-90
c. >90
18
25
2
40.00
55.56
4.44
3. Family history with
hypertension
a. Yes
b
. No
37
8
82.22
17.78
4. Educational background
a. Primary school
b. Secondary school
c. High school
d. Diploma
e. Bachelor degree
18
14
7
4
2
40.00
31.11
15.56
8.89
4.44
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
414
4 DISCUSSION
Self-efficacy in elderly who are living with
hypertension defined as self-confidence and
competency for doing some tasks, such as diet
management, physical exercise, drugs
administration, stress management, socialize with
others, occupational therapy, etc., to achieve the goal
of normal blood pressure. Most respondents had
sufficient self-efficacy. This potentially influenced
by cognitive function, affective, and selection
process in elderly’s state of mind (Bandura, 1997 in
Guffron & Risnawati, 2014).
Cognitive function is a conscious mental activity,
such as thinking, remembering, learning and using
language. Cognitive function is also the ability of
paying attention, memory, consideration, problem
solving, and the ability of executive competency
such as planning, assessing, monitoring and
evaluating (Strub, et al., 2000). In elderly people, we
found decreased cognitive function generally.
Memory is one of the earliest cognitive function
which decline. Long-term memory is less likely to
change, while short-term memory is instantly
changes in 0-10 minutes. For declining intellectual
functions, the fluid intelligent such as list recall,
geometric memory, word finding speed, problem
solving, responsiveness, and attention quickly
diverted (Kusumoputro, 2004). The ability to
understand or grasp the understanding of the elderly
has decreased. This is influenced by the decreased in
concentration and hearing function. In the elderly,
the problems faced more and more by time. Many
things can easily be solved in ancient times, but are
now hampered by the decline in cognitive function.
Other obstacles are derived from memory loss,
comprehension, and others that result in more
problem-solving difficulties (Azizah, 2011).
In performing individual tasks, we need to set the
goals and objectives of behavior so that individuals
can formulate appropriate actions to achieve those
goals. The setting of personal goals is influenced by
the individual's assessment of his cognitive abilities.
Cognitive function allows individuals to predict the
daily events that will result in the future. The
assumption that arises on this cognitive aspect is the
more effective the individual's ability in analyzing
and in practicing to express his personal ideas. It
will support the individual to act appropriately to
achieve the expected goal. Individuals will foresee
events and develop ways to control events that affect
their lives. This expertise requires an effective
cognitive process of various kinds of information
(Bandura, 1997 in Guffron & Risnawati, 2014).
Affection occurs naturally within the individual
and plays a role in determining the intensity of the
emotional experience. Affection is directed by
controlling anxiety and depressive feelings that
hinder the right mind set to achieve goals. The
process of affection is related to the ability to cope
with emotions that arise in self to achieve the
expected goals. The individual's belief in his ability
to influence the level of stress and depression
experienced when faced with difficult or threatening
tasks. Individuals who believe they are capable of
controlling a threat will not arouse an intrusive mind
set. Individuals who do not believe in their abilities
will experience the anxiety of not being able to
manage the threat (Bandura, 1997 in Guffron &
Riisnawati, 2014).
The selection process relates to the individual's
ability to select appropriate behavior and
environment, so as to achieve the expected
objectives. Individual inability to perform behavioral
selection makes individuals unconfident, confused,
and easily give up when faced with difficult
problems or situations. Self-efficacy can shape the
lives of individuals through the selection of activity
and environment types. Individuals will be able to
carry out challenging activities and choose situations
that are believed to be capable of handling.
Individuals will maintain competence, interests, and
social relationships over the prescribed choice. It can
be concluded that the process of self-efficacy
includes cognitive, affection, and selection processes
(Bandura, 1997 in Guffron & Risnawati, 2014).
Study result showed that there was no correlation
between self-efficacy and quality of life (QOL) in
elderly who are living with hypertension. QOL has
been used as an indicator of how well a society
meets the needs of its elderly. There are various
potential variables mediate the relationship between
self-efficacy and QOL or possibly affecting QOL
stronger than self-efficacy alone in this study
context. Generally, QOL is influenced by living
standard. Reasonable standard of living has changed
with time and cultural settings. In a society with
Table 2: Table of frequency and descriptive statistic.
Category Self-efficacy QOL
n % n %
Low 0 0 12 26.67
Sufficient 37 82.22 33 73.33
Hi
g
h 8 17.78 0 0
Mean 28.27 46.09
Std. Deviation 3.39 9.30
The Correlation between Self-efficacy and Quality of Life in Elderly Who are Living with Hypertension
415

inequalities in living standard, there is elevated
stress level, especially in the lowest socio-economic
status, leading to poorer health and even lower life
satisfaction (Marmot & Richard, 2006). Low socio-
economic status possibly affects QOL because
financial insecurity or problems has led to high
stress level among elderly in general, especially
related to retirement and family neglect.
Although QOL scores tends to decreased with
increasing age, a support of physical functions
optimization in older adults can be important for
increasing QOL and functional independence
(Bozkurt & Yilmaz, 2016). In elderly with
hypertension, some vascular risk factors are
associated with functional impairment due to clinical
and subclinical vascular disease (Canavan, et al,
014). Age-related physiological changes also bring a
reduction in functional capabilities resulted in
problems with self-care, activities of daily life, and
psychosocial problems. It has been identified that
intense exercise was not an obligatory condition for
optimal QOL in elderly people. Active part in
moderate intensity daily activities associated with
higher QOL (Pavlova, et al., 2015).
Other factor that possibly affects QOL in elderly
who are living with hypertension is social support,
especially from family subgroup. Elderly living with
their spouse and children had better social support
family subgroup scores compared to ones living
alone. A positive correlation was found between
social support and QOL (Unsar, et al, 2016). A study
in Korea towards 1,056 elderly showed that the
elderly who give and receive family support had
higher QOL than the one who only receive support.
Elderly and the younger generation put more value
on two-way intergenerational relation based on
mutual care and assistance (Kim & Cheong-Seok,
2003). Family and friend support are different across
ethnic because culture also influence the support
pattern in our society (Poulin et al, 2012).
Cultural factor could also be a potential factor
influencing QOL Social and cultural norms,
informed by religious principles that prescribe
familial elder care, impact how QOL is described by
elderly. It is also possible that religious faith or
traditions might provide a different account of how
individual’s own religious faith impacts expectations
of care and QoL in old age (Shreshta & Zarit, 2012).
A study in Singapore towards elderly showed that
QOL was more likely to be determined by socio-
cultural context rather than along racial lines (Wong,
2003).
5 CONCLUSIONS
There was no correlation between self-efficacy and
QOL in elderly who are living with hypertension.
Self-efficacy was potentially influenced by cognitive
function, affective, and selection process in elderly’s
state of mind. Independency level, family support,
socio-economic status, living standard, and culture
were potentilly influenced QOL in elderly who are
living with hypertension stronger than self-efficacy.
ACKNOWLEDGEMENTS
This study and publication were funded by Faculty
of Nursing, Widya Mandala Catholic University
Surabaya (WMCUS).
REFERENCES
Azizah. (2011). Keperawatan Lanjut Usia. Yogyakarta:
Graha Ilmu
Basic Health Research. (2013). Badan Penelitian dan
Pengembangan Kesehatan Kementrian Kesehatan
Republik Indonesia. Retrieved from:
http://www.depkes.go.id/resources/download/general
/Hasil%20Riskesdas%202013.pdf.
Bozkurt, Ü., Yilmaz, M. 2016. The determination of
functional independence and quality of life of older
adults in a nursing home. International Journal of
Caring Sciences, 9(1): 198-210.
Brunner., Suddarth. (2002). Buku Ajar Keperawatan
Medikal Bedah, edisi 8 volume 2. Jakarta: EGC.
Canavan, M., Glynn, L.G, Smith, A., Mulkerrin, E.C.,
Murphy, A.W., Mulqueen, J., McGrath, E.,
O'Donnell, M.J. 2014. Vascular risk factors,
cardiovascular disease and functional impairment in
community-dwelling adults. Gerontology, 60(3): 212-
221.
Corwin, E.J. 2009, Buku Saku Patofisiologi, edisi 3.
Jakarta: EGC.
Kim, I.K., Kim, C.S. 2003. Patterns of family support and
the quality of life of the elderly. Social Indicators
Research, 62(1): 437-454.
Kusumoputro, S. 2004. Mengenal Awal Pikun Alzheimer.
Jakarta: UI-press.
Luszczynska, A., Dona, B.G. 2005. General self-efficacy
in various domains of human functioning: evidence
from five countries. International Journal of
Psychology, 40(2): 80–89.
Marmot, M., Richard, G.W. 2006, Sosial Determinants of
Health. 2
nd
. Ed., USA: Oxford University Press.
Muttaqin, A. (2009). Asuhan Keperawatan Klien dengan
Gangguan Sistem Kardiovaskular dan Hematologi.
Jakarta: Salemba Medika.
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
416

Padila. (2013). Asuhan Keperawatan Penyakit Dalam.
Yogyakarta: Nuha Medika.
Pavlova, I., Bogdan, V., Borek, Z., Borek, I. 2015. Life
quality and physical activity of Ukrainian residents.
Journal of Physical Education and Sport, 124: 809-
814.
Price, S.A., Wilson, L.M. (2006). Patofisiologi: Konsep
Klinis Proses-proses Penyakit, Edisi 6, Volume 1.
Jakarta: EGC.
Poulin, J., Deng, R., Ingersoll, T.S., Witt, H., Swain, M.
2012. Perceived family and friend support and the
psychological well-being of American and Chinese
elderly persons. J Cross Cult Gerontol, 27(4): 305-17.
Shrestha, S., Zarit, S.H. 2012. Cultural and contextual
analysis of quality of life among older Nepali women.
J Cross Cult Gerontol, 27(2): 163-182.
Strub, R.L., Black, F.W. (2000). The Mental Status
Examination in N,eurology 4th Ed., Philadelphia: F. A.
Davis.
Unsar, S., Erol, O., Sut, N. 2016. Social support and
quality of life among older adult. International
Journal of Caring Sciences, 9 (1): 249-257.
Wong, G.K.M. 2003. Quality of life of the elderly in
Singapore’s multi-racial society. International Journal
of Social Economics, 30(3): 302-319.
WHO. (2004). Instrument BREF. Retrieved from:
www.who.int
The Correlation between Self-efficacy and Quality of Life in Elderly Who are Living with Hypertension
417
