
The Impact of Using the Mental Health Smart Book (BISAA) to
Increase Physical, Psychological, Social, and Spiritual Life Qualities
in the Elderly
Hanik Endang Nihayati, Alfita Nadziir and Rr. Dian Tristiana
Faculty of Nursing Universitas Airlangga, Kampus C Mulyorejo, Surabaya, Indonesia
Keywords: Mental health smart book, Quality of life, Elderly.
Abstract: The elderly are at risk of stress because of the physical, psychological, and social changes that they
experience. Intervention is needed to increase the physical, psychological, social, and spiritual life qualities
of the elderly. One of the interventions is stress management, taught through health education by using the
mental health smart book (Buku Pintar Sehat Jiwa Lansia/ BISAA). This study aimed to analyze the effect
of BISAA in increasing the physical, psychological, social, and spiritual qualities in the elderly. A Quasi-
experiment research design was used in this study. The target population were 744 elderly people; the
affordable population were 80 elderly people and the sample comprised of 16 elderly selected by purposive
sampling. The independent variable was health education with BISAA. The dependent variables were the
physical, psychological, social, and spiritual qualities of life. Data were collected using a questionnaire
regarding physical, psychological, social, and spiritual qualities. The study was analyzed using the
Wilcoxon Signed Rank Test and the Mann Whitney U test with a significance level of p≤0.05. The results
from the Wilcoxon Signed Rank Test indicated that physical quality p = 0.014, psychological quality p =
0.011, social quality p = 0.020, and spiritual quality p=0.008. In addition, the statistical test results from the
Mann Whitney U test for physical quality indicated p = 0.028, psychological quality p = 0.012, social
quality p = 0.020, and spiritual quality p = 0.014. Based on these results, it can be concluded that BISAA
can increase the physical, psychological, social and spiritual qualities in elders, the most dominant of which
is the psychological quality. Further research is expected to analyze the effect of BISAA to increase the
environment quality for the elderly.
1 BACKGROUND
The aging process is a process that continues
naturally. The consequence of that process gives rise
to changes in the elderly, including physical,
psychological, and social changes (Azizah, 2011;
Joseph, 2015). Such changes can impact on the
health of the elderly because every change can be a
stressor (a source of stress) that requires elderly
people to adapt (Idris, 2015). When elderly people
suffer from stress, their quality of life deteriorates,
hence there is a need for others to support them and
help them cope with stress. Stress management can
help the elderly by modify various behaviors that are
risky to health and so improve the quality of life
(Edelman & Mandle, 2010).
The World Health Organization (WHO) (2013)
explained that in Southeast Asia, the elderly
population accounts for 142 million people or 18%
of the. It is estimated that by 2050, the elderly
population will have increased three times from this
year (Kemenkes, 2013). According to the National
Socioeconomic Survey (susenas) in 2014, the
number of elderly people in Indonesia reached 20.24
million people or around 8.03% of Indonesia’s total
population (Kemenkes, 2016). The number of
elderly people in Indonesia by 2021 is estimated to
reach 30.1 million people; for these figures,
Indonesia is ranked fourth in the world after China,
India and the United States. By 2050 the number is
expected to increase to more than 50 million people
(Kemenkes, 2013).
According to data obtained from the Surabaya
City Health Office, the number of elderly people in
Nihayati, H., Nadziir, A. and Tristiana, R.
The Impact of Using the Mental Health Smart Book (BISAA) to Increase Physical, Psychological, Social, and Spiritual Life Qualities in the Elderly.
DOI: 10.5220/0008325603790387
In Proceedings of the 9th International Nursing Conference (INC 2018), pages 379-387
ISBN: 978-989-758-336-0
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
379

East Java in 2013 was 4,210,339 people. The
number of elderly people in Surabaya in 2014 was
228,798 people, compared 217,116 people in 2013.
The number of elderly people in the District of
Tambak Sari in 2014 was 18,584 people. According
to data obtained from the Pacarkeling Community
Health Centre in 2016, the number of elderly people
in the working area of Pacarkeling Community
Health Center was 1,424 people. There were 744
elderly people in Pacarkeling Village and 680
elderly people in Pacarkembang Village. The
number of elderly in RW IX Pacarkeling was 80.
The Basic Health Research Data (Riskesdas) in
2007 indicated that the prevalence of mental
emotional disorders increases with age. In the age
group 55–64 years, the prevalence of emotional
mental disorders is 15.9%. This number increases in
the age group 65–74 years to 23.2% (MOH, 2008).
The survey was conducted by researchers at the
Pacarkeling Community Health Centre, Surabaya on
May 10, 2016. The Elderly Visiting Elderly
Integrated Service Post (Posyandu) is more focused
on physical complaints and physical examinations
such as weighing, height measurements, and blood
pressure and does not check mental status. The
results of the preliminary survey supplied physical,
psychological, social, and spiritual quality
questionnaires to 43 elderly people who visited the
Elderly Integrated Service Post (Posyandu) in Seroja
RW IX Pacarkeling Surabaya indicated that there are
no elderly people whose physical, psychological,
social, and spiritual quality are very good.
If the stress on elderly people is not immediately
addressed, it could cause an impact on the elderly in
the form of physical illness, psychological, social,
and spiritual problems. Physical diseases caused or
exacerbated by stress are arteriosclerosis, heart
attacks, cancer, respiratory disorders, bone loss,
nausea, diarrhea, hypertension, and strokes. Sexual
disorders and diabetes mellitus also appear due to
stress (Losyk, 2005; Sukadiyanto, 2010).
Psychological problems in the elderly include
sleeping disorders (insomnia), depression, and even
suicide. Social problems that can arise include the
decline of personal relationships and withdrawal
from others (rather than seeking social support).
Spiritual problems are marked by a decline in
religious beliefs. The impact of stress can ultimately
reduce the quality of life for elderly people (Losyk,
2005).
According to the WHOQOL-SRPB BREF, the
quality of life domain includes five elements:
physical, psychological, social, environmental, and
spiritual (Skevington, 2013). Most researchers
measure quality of life using the physical,
psychological, social and environmental quality
domains. In addition to the four domains, spiritual
quality is very important because individuals who
have good spiritual qualities will live a life in
harmony both as a person and as part of the social
environment and will live peacefully because they
feel close to God. Spirituality is also a reflection of
cultural heritage for the Indonesian nation and is
believed to contain noble values and norms that are
obeyed by society, impacting greatly on life
(Imaddudin, 2015). Improving elderly people’s
quality of life of the enables them to enjoy their old
age with full meaning, happiness, health,
independence, productivity, usefulness, and
prosperity (Kemenkes, 2013).
Stress management can be taught to elderly
people through a variety of media, including via a
book described as the media of elderly mental health
smart book (BISAA). The book contains information
about the elderly, healthy elderly souls, stress, and
stress management. Stress management, which is
easy to apply to the elderly, includes using mini
relaxation, a healthy diet, physical activity, social
support, spiritual practice, and humor. This book
also features the Healthy Elderly Card (KMS) that
can be completed when visiting the Elderly
Integrated Service Post (Posyandu).
Based on the chronology of the problems
described above, the researcher is interested in
conducting research on "The Influence of Elderly
Mental Health Smart Book (BISAA) on Improving
Physical, Psychological, Social and Spiritual Quality
at the Elderly Integrated Service Post (Posyandu)
Seroja RW IX Pacarkeling Surabaya."
2 METHODS
The method used in this research was the Quasi
Experiment with a pre-post test group control
design. The target population were the elderly in
Pacarkeling Surabaya, of which there are 744, and
the reachable population of the elderly in RW IX
Pacarkeling Surabaya amounted to 80 people. The
inclusion criteria in this study were the elderly who
visited the Elderly Integrated Service Post
(Posyandu) Seroja RW IX Pacarkeling Surabaya,
aged 64–74 years, have very bad, bad, moderate or
good physical, psychological, social, and spiritual
qualities, and be able to read. The exclusion criteria
were elderly people with hearing loss.
A purposive sampling technique was used.
Sixteen elderly samples were divided into two
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
380
groups: the treatment and control groups; each group
had a total of eight elderly people. The independent
variable is health education using the elderly mental
health smart book (BISAA). The dependent
variables are the physical, psychological, social, and
spiritual qualities. The instrument used is the SAP
(Counseling Event Unit), Elderly Mental Health
Smart Book (BISAA), which contains about elderly,
healthy soul elderly, stress management, Elderly
Health Card (KMS) and a questionnaire consisting
of two parts: demographic data questionnaire
(gender, age, last education, and marital status) and
valid and reliable physical, psychological, social,
and spiritual quality questionnaires.
The study was conducted over three weeks. The
pre-test used physical, psychological, and spiritual
quality questionnaires using door to door collection
for the treatment and control group the day before
the health education mental health smart book
(BISAA) was given to the elderly pariticpants.
Intervention was held once a week as many as 3
times of treatment group meeting at Elderly
Integrated Service Post (Posyandu) Seroja RW IX
Pacarkeling Surabaya. Subsequently a post-test was
conducted using a physical, psychological, social,
and spiritual quality questionnaire for both groups
through door to door collection one week after the
third meeting. The collected data were analyzed
using the Wilcoxon Signed Rank Test and the Mann
Whitney U test with p≤0.
3 RESULTS
3.1 Respondents’ Demographic
Characteristics
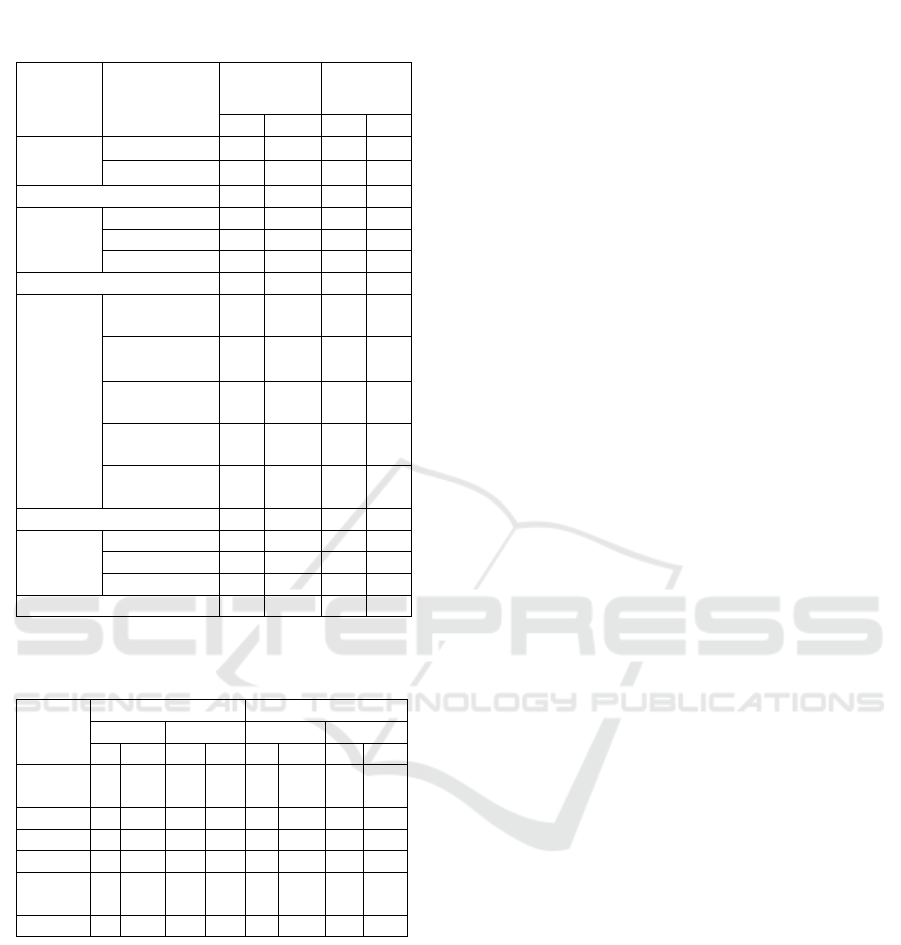
Table 1 shows that females dominated both the
treatment and control groups. In the treatment group
there were six female respondents (75%) and in the
control group there were five female respondents
(62.5%). Half (four) of the respondents in both
groups were aged 60–64 (50%). Three (37.5%)
respondents in each group had an elementary school
and senior high school education background. Most
elderly respondents (five) in both groups were
married (62.5%).
3.2 Measured Variables
3.2.1 Physical Qualities
Table 2 indicates that physical quality was moderate
for most (five or 62.5%) respondents before the
intervention was provided to the treatment group.
The pre-test in the control group showed that many
(three or 37.5%) elderly respondents had medium
and good physical qualities. Following the
intervention, most elderly respondents (five or
62.5%) had good physical qualities while most of
the respondents in the control group had moderate
physical condition (five or 62.5%).
Table 1: Demographic Characteristic Data of the
Respondents.
Data Category
Treatment
Grou
p
Control
Grou
p
f % f %
Sex
Male 2 25 3 37.5
Female 6 75 5 62.5
Total 8 100 8 100
Age
60
–
64 4 50 4 50
65
–
69 2 25 1 12.5
70
–
74 2 25 3 37.5
Total 8 100 8 100
Education
Did not go
to School 0 0 0 0
Elementary
School 3 37.5 3 37.5
Junior High
School 2 25 2 12.5
Senior High
School 3 37.5 3 37.5
Undergraduate
Stud
y
0 0 0 0
Total 8 100 8 100
Marital
Status
Unmarrie
d
0 0 0 0
Marrie
d
5 62.5 5 62.5
Widowe
d
3 37.5 3 37.5
Total 8 100 8 100
Table 2: Physical Quality Distribution of the
Respondents.
Physical
Treatment Control
Pre-Test Post-Test Pre-Test Post-Test
f % f % f % f %
Very
Ba
d
0 0 0 0 0 0 0 0
Ba
d
0 0 0 0 2 25 0 0
Moderate 5 62.5 1 12.5 3 37.5 5 62.5
Goo
d
3 37.5 5 62.5 3 37.5 3 37.5
Very
Goo
d
0 0 2 25 0 0 0 0
Total 8 100 8 100 8 100 8 100
The Impact of Using the Mental Health Smart Book (BISAA) to Increase Physical, Psychological, Social, and Spiritual Life Qualities in the
Elderly
381
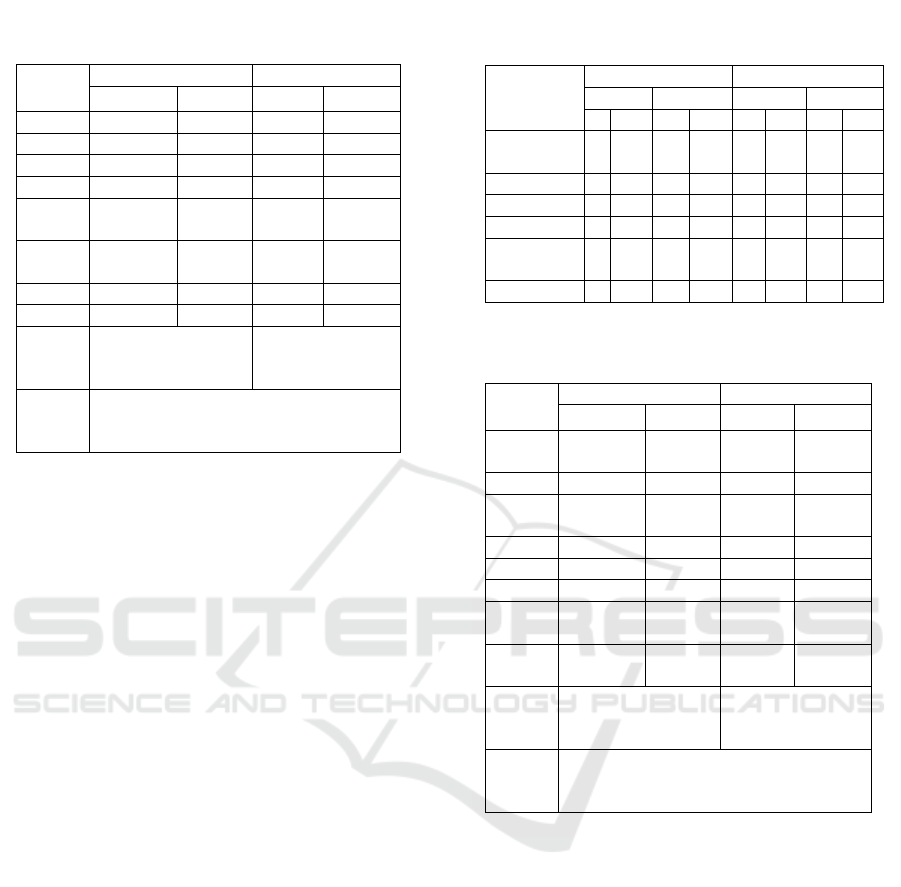
From Table 3 it can be seen that physical
qualities in the treatment group, after being provided
with health education using the elderly mental health
smart book (BISAA), mostly increased to six (75%).
The results of the analysis using the Wilcoxon
Signed Rank Test in the treatment group obtained a
sig value (2-tailed) of p = 0.014, so p <0.05. These
results indicate that there is a difference between the
physical quality before and after being given health
education by the elderly mental health smart book
(BISAA) in the treatment group.
In the control group, most (six or 75%) of the
respondents did not indicate a difference in the
physical quality between the pre-test and post-test
results. The statistical test results using Wilcoxon
Signed Rank Test in the control group obtained a sig
value (2-tailed) of p = 0.157 so p> 0.05. These
results indicate that there is no difference in physical
quality between the pre-test and post-test in the
control group.
Statistical test results using the Mann Whitney U
Test sig (2-tailed) value was p = 0.028 so p <0.05.
These results indicate that there is a difference
between the physical quality of the treatment group
and the control group.
3.2.2 Psychological Qualities
Table 4 indicates that most respondents (five or
62.5%) in the treatment group demonstrated
moderate psychological qualities before the
intervention. In the control group, half (four or 50%)
demonstrated moderate psychological qualities.
After the intervention, half (four or 50%) of
respondents in the treatment group demonstrated
very good psychological qualities, while the post-
test results in the control group showed that many
respondents had moderate and good psychological
qualities with three (37.5%) respondents for each.
Table 5 indicates that after being given
intervention, the psychological qualities of elderly
respondents increased to seven (87.5%). The results
of the statistics test using the Wilcoxon Signed Rank
Test in the treatment group obtained a sig value (2-
tailed) of p = 0.011 so p <0.05. These results
indicate that there is a difference between
psychological qualities before and after the delivery
of health education using the elderly mental health
smart book (BISAA) with the treatment group.
In the control group, most participants (five or
62.5%) showed that the psychological qualities
Table 3: Data Result of the Pre-test and Post-test in
Physical Quality.
Respon-
dent
Treatment Control
Pre-Test Post-Test Pre-Test Post-Test
1 Moderate Goo
d
Ba
d
Moderate
2 Moderate Goo
d
Moderate Moderate
3 Moderate Goo
d
Goo
d
Goo
d
4 Moderate Moderate Moderate Moderate
5 Good
Very
Goo
d
Good Good
6 Good
Very
Goo
d
Moderate Moderate
7 Goo
d
Goo
d
Goo
d
Goo
d
8 Moderate Goo
d
Ba
d
Moderate
Wilcoxon
Signed
Ran
k
p = 0.014 p = 0.157
Mann
Whitney
U Test
Post-Test p = 0.028
Table 4: Psychological Quality Distribution of the
Respondents.
Psycho-
logical
Treatment Control
Pre-Test Post-Test Pre-Test Post-Test
f % f % f % f %
Very
Ba
d
0 0 0 0 0 0 0 0
Ba
d
0 0 0 0 1 12.5 0 0
Moderate 5 62.5 1 12.5 5 62.5 5 62.5
Goo
d
3 37.5 4 50 2 25 3 37.5
Very
Goo
d
3 37.5 4 50 2 25 3 37.5
Total 8 100 8 100 8 100 8 100
Table 5: Data Result of the Pre-test and Post-test in
Psychological Quality.
Respon-
dent
Treatment Control
Pre-Test Post-Test Pre-Test Post-Test
1 Moderate
Very
Goo
d
Moderate Bad
2 Moderate Goo
d
Moderate Moderate
3 Good
Very
Goo
d
Moderate Good
4 Moderate Moderate Ba
d
Ba
d
5 Moderate Goo
d
Goo
d
Goo
d
6 Moderate Goo
d
Ba
d
Moderate
7 Good
Very
Goo
d
Good Good
8 Good
Very
Goo
d
Moderate Moderate
Wilcoxon
Signed
Ran
k
p = 0.011 p = 0.564
Mann
Whitney
U Test
Post Test p = 0.012
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
382
between the pre-test and post-test did not change.
Statistical test results using the Wilcoxon Signed
Rank Test, in the control group, obtained a sig value
(2-tailed)of p = 0.564 so p> 0.05. The results show
that there was no difference in the psychological
quality between pre-test and post-test in the control
group. The statistical test results used the Mann
Whitney U Test sig (2-tailed) with a value of p =
0.012 so p <0.05. These results indicate that there is
a difference between the psychological qualities of
the treatment group and the control group.
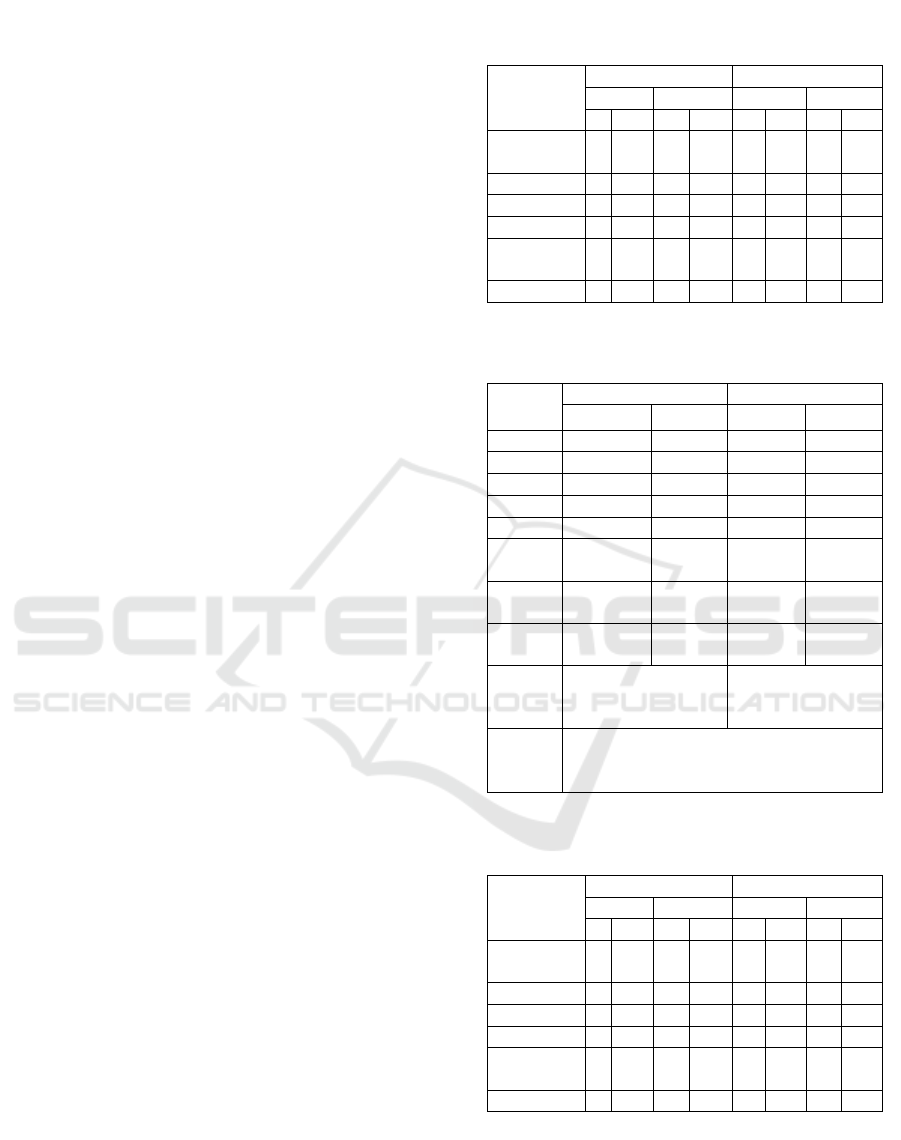
3.2.3 Social Qualities
Table 6 indicates that five (62.5%) elderly
respondents demonstrated moderate social qualities
before being provided with intervention in the
treatment group and the same result was indicated in
the pre-test in the control group. After the
intervention was given, results for the the treatment
group indicated that half (four or 50%) of
responbdents had good social qualities while, in the
post-test for the control group, most (five or 62,5%)
indicated moderate social qualities.
From Table 7, it is evident that six (75%) eldely
respondents indicated an increase in social qualities
following the intervention. The results of the
statistics analysis using the Wilcoxon Signed Rank
Test for the treatment group obtained a sig value (2-
tailed) of p = 0.020 so p <0.05. These results
indicate that there is a difference between social
qualities before and after the health education was
delivered, using the elderly mental health smart
book (BISAA) for the treatment group.
In the control group, most respondents (six or
75%) indicated no change in psychological qualities
between the pre-test and post-test. Statistical test
results using the Wilcoxon Signed Rank Test in the
control group obtained a sig value (2-tailed) of p =
0.157 so p> 0.05. These results indicate that there is
no social quality difference between the pre-test and
post-test in the control group.
Statistical test results using the Mann Whitney U
Test sig (2-tailed) value were p = 0.020 so p <0.05.
These results indicate that there is a difference
between the social qualities of the treatment group
and the control group.
3.2.4 Spiritual Qualities
Table 8 indicates that half of the respondents (four
or 50%) in the treatment group had good spiritual
qualities before being given intervention and before
the pre-test in the control group. Following the
intervention, most (five or 62.5%) respondents’
spiritual qualities in the treatment group were very
good, while the post-test in the control group
indicated that many (three or 37.5%) of elderly
Table 6: Social Quality Distribution of the
Respondents.
Social
Treatment Control
Pre-Test Post-Test Pre-Test Post-Test
f % f % f % f %
Very
Ba
d
0 0 0 0 0 0 0 0
Ba
d
0 0 0 0 1 12.5 0 0
Moderate 5 62.5 1 12.5 5 62.5 5 62.5
Goo
d
3 37.5 4 50 2 25 3 37.5
Very
Goo
d
0 0 3 37.5 0 0 0 0
Total 8 100 8 100 8 100 8 100
Table 7: The Data Result of the Pre-test and Post-test
in Social Quality.
Respon-
dent
Treatment Control
Pre-Test Post-Test Pre-Test Post-Test
1 Moderate Goo
d
Goo
d
Goo
d
2 Moderate Goo
d
Moderate Moderate
3
Goo
d
Goo
d
Moderate Moderate
4 Moderate Moderate Moderate Moderate
5 Moderate Goo
d
Moderate Moderate
6 Good
Very
Goo
d
Bad Moderate
7 Good
Very
Goo
d
Good Good
8 Good
Very
Goo
d
Moderate Good
Wilcoxon
Signed
Ran
k
p = 0.020 p = 0.157
Mann
Whitney
U Test
Post-Test p = 0.020
Table 8: The Spiritual Quality Distribution of the
Respondents.
Spiritual
Treatment Control
Pre-Test Post-Test Pre-Test Post-Test
f % f % f % f %
Very
Ba
d
0 0 0 0 0 0 0 0
Ba
d
1 12.5 0 0 1 12.5 1 12.5
Moderate 3 37.5 0 0 3 37.5 3 37.5
Goo
d
4 50 3 37.5 4 50 3 37.5
Very
Goo
d
0 0 5 62.5 0 0 1 12.5
Total 8 100 8 100 8 100 8 100
The Impact of Using the Mental Health Smart Book (BISAA) to Increase Physical, Psychological, Social, and Spiritual Life Qualities in the
Elderly
383
respondents have moderate and good spiritual
qualities.
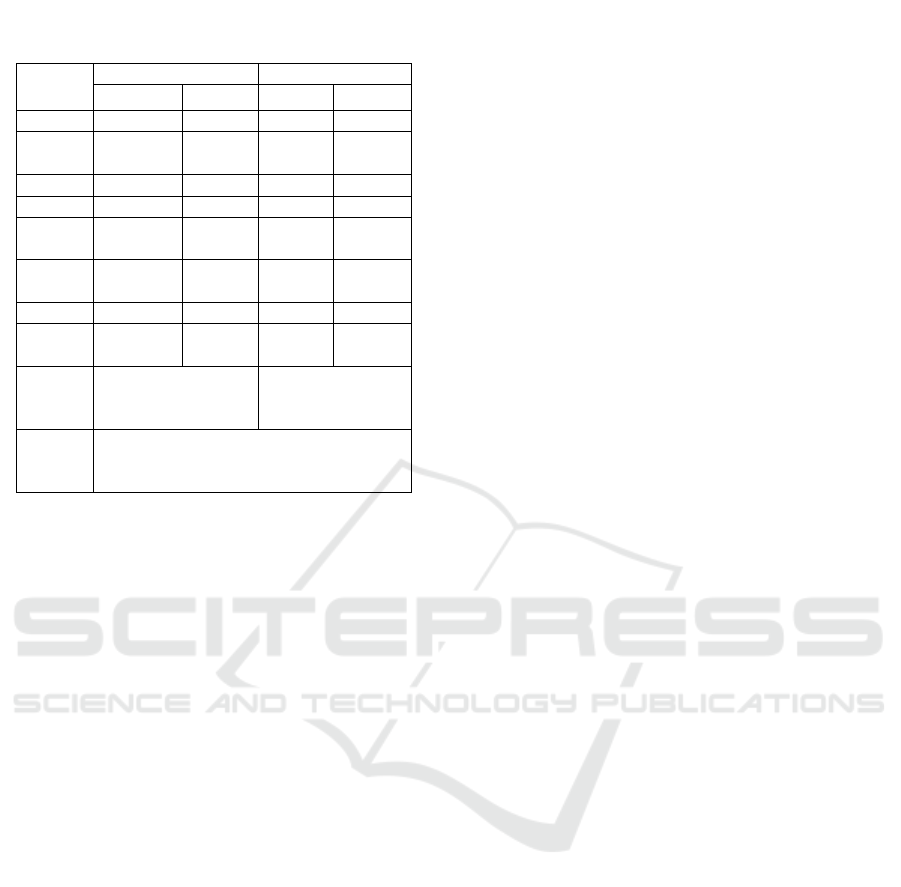
Table 9 indicates that after being given
intervention in the treatment group, the spiritual
qualities of all (eight or 100%) elderly people were
good. The results of the statistics test using the
Wilcoxon Signed Rank Test in the treatment group
obtained a sig value (2-tailed) of p = 0.008 so p
<0.05. These results indicate that there is a
difference between the spiritual qualities before and
after being given health education by the elderly
mental health smart book (BISAA) in the treatment
group.
In the control group most (seven or 82.5%)
respondents’ spiritual qualities between the pre-test
and the post-test did not change. The results of the
statistical test using the Wilcoxon Signed Rank Test
in the control group, obtained a value of sig (2-
tailed) at p = 0.317 so p> 0.05. These results indicate
that there is no difference in the psychological
qualities between pre-test and post-test in the control
group.
The statistical test results using the Mann
Whitney U Test sig (2-tailed) value was p = 0.014 so
p <0.05. These results indicate that there is a
difference between the psychological quality of the
treatment group and the control group.
4 DISCUSSION
4.1 Physical Qualities
Table 2 indicates that most treatment group
respondents’ physical qualities were moderate
before being provided with health education with
the media of elderly mental health smart book
(BISAA) as they sometimes have the ability to
perform daily activities, and have enough energy
and ability to carry out an activity. The pre-test in
the control group showed that many respondents had
moderate and good physical qualities, as they often
have enough energy to perform the activity and
sometimes feel satisfied.
After being given health education using the
elderly mental health smart book (BISAA), it was
determined that regarding the physical qualities of
the treatment group, most (75%) experienced
improvement, such as being more able to perform
daily activities, have enough energy to carry out the
activity, getting along with others, and satisfied by
sleep. The post-test regarding physical qualities in
the control group indicated that the majority of
respondents (75%) did not change or remain the
same as they often had enough energy to perform the
activity and were sometimes satisfied with their
sleep.
Mubarak (2007) describes health education as a
dynamic process of behavior change. Stress
management can improve physical qualities because
of stress management strategies that conduct mini
relaxation, healthy diet, and physical activity
(Edelman & Mandle, 2010).
Mini relaxation can concentrate the mind so that
the blood vessels can become more elastic.
Circulation will be smoother so that the body
becomes relaxed and warm; the work of the heart
will feel lighter, which certainly affects the workings
of other organs to improve physical qualities
(Handoyo, 2004).
A healthy diet makes it is possible for the body
to obtain good nutrition to improve physical
functions and improve physical quality (Swarth,
2006). Scientists state that an active lifestyle and
regular exercise can help prevent or delay the onset
of illness and disability, increase appetite, help with
the recovery of old diseases, increase energy,
balance, immunity, and flexibility, thus improving
physical quality (Hutapea, 2005).
In the treatment group there were elderly people
whose physical qualities were the same as they were
before intervention was given. This is because the
elderly were not paying enough attention when the
Table 9: Data Result of the Pre-test and Post-test in
Spiritual Quality.
Respon-
dent
Treatment Control
Pre-Test Post-Test Pre-Test Post-Test
1 Moderate Goo
d
Goo
d
Goo
d
2 Good
Very
Goo
d
Moderate Moderate
3 Moderate Very Moderate Moderate
4 Ba
d
Goo
d
Goo
d
Goo
d
5 Moderate Good Good Good
6 Good
Very
Goo
d
Bad Bad
7 Goo
d
Ver
y
Moderate Moderate
8 Good
Very
Goo
d
Good
Very
Goo
d
Wilcoxon
Signed
Ran
k
p = 0.008 p = 0.317
Mann
Whitney
U Test
Post-Test p = 0.014
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
384

intervention was given, and one of the elderly people
had an elementary school educational background so
was unable to absorb and understand the health
education provided. In the control group there were
elderly people whose physical quality increased
even though they did not receive intervention. This
is because the elderly have an awareness in
maintaining their physical health and actively follow
the elderly integrated service post (Posyandu) and
avoid foods that can worsen their health condition.
4.2 Psychological Qualities
Table 4 determines that most respondents had
moderate psychological qualities before being given
health education through the elderly mental health
smart book (BISAA), such as sometimes accepting
their body appearance, having negative feelings
(loneliness, despair, anxiety, and depression), and
having positive feelings (happy and cheerful). The
pre-test in the control group showed that half of the
respondents had moderate psychological qualities
such as having positive feelings (happy and
cheerful), sometimes feeling satisfaction.
After being given the health education through
elderly mental health smart book (BISAA), it was
determined that most respondents (87.5%) in the
treatment group the result is psychological quality in
treatment group found that their psychological
qualities, with indicators such as frequently
accepting body appearance, never having negative
feelings (loneliness, despair, anxiety, depression),
frequently having positive feelings (happy and
cheerful) and frequently demonstrating the ability to
concentrate. The post-test of psychological qualities
in the control group showed the majority (62.5%)
did not change; some had positive feelings (happy
and cheerful) and sometimes they were satisfied
with themselves.
Mubarak (2007) describes health education as a
dynamic process of behavior change. Stress
management can improve psychological quality
because of stress management strategies linked to
carrying out mini relaxation, healthy diet, physical
activity, and humor (Edelman & Mandle, 2010).
Mini relaxation can calm the mind, feeling,
psychology, form mental resilience, accelerate
healing and stress relief (depression), to improve
psychological qualities (Handoyo, 2004). According
to Swarth (2006) a healthy diet allows the body to
obtain good nutrition that can improve the health
conditions of the elderly to overcome stress and
develop psychological qualities.
Physical activity can release endorphins from the
brain, resembling the effects of morphine.
Endorphins prompt feelings of comfort. Physical
exercise also creates mental and emotional relief that
helps a person cope and prevent stress to improve
psychological qualities (Swarth, 2006).
In addition, individuals who have high levels of
humor are known to cope better with stress, establish
relationships with people around them, and are
physically healthier. When an individual can cope
well with stress, then feelings of disappointment or
sadness that may arise as a result of a mismatch of
expectations with reality are reduced, therefore
individuals have good psychological qualities
(Hardianti, 2014).
In the treatment group there were elderly people
whose psychological qualities were the same before
and after the intervention. This is because they were
not paying enough attention during the intervention
and had elementary school background, so had less
ability to absorb the health education provided. In
the control group there was an elderly person whose
psychological quality increased, despite not
receiving intervention. This is because the elderly
person was aged between 60 and 64 and had a life
partner, therefore the psychological quality was
good and his high school educational background
meant that he could understand various problems
that could interfere with his psychological qualities
and know how to handle them. Furthermore, there
are elderly people in the control group who
experienced a degradation in psychological qualities
because they were often worried about their health
condition; they are 74 years old and feel lonely
because they do not have spouse or are widowed and
live alone.
4.3 Social Qualities
Table 6 indicates that social qualities before the
health education intervention using the elderly
mental health smart book (BISAA) in group of
treatment and pre-test in control group were mostly
moderate. Respondents were sometimes satisfied
with interaction from others and sometimes satisfied
with the support given by a friend.
After being given health education using elderly
mental health smart book (BISAA), it was found that
social qualities in the treatment group had increased
for 75% of the sample, relating to satisfaction in
interacting with others and often feeling satisfied
with the support given by friends. The post-test of
social qualities in the control group indicated there
was no change in the results.
The Impact of Using the Mental Health Smart Book (BISAA) to Increase Physical, Psychological, Social, and Spiritual Life Qualities in the
Elderly
385

Stress management can improve social qualities
because stress management strategies seek to
provide social support. Social support can be
obtained by telling stories and talking about
problems regarding the social environment with
others, such as family, friends, and close relatives.
Therefore they obtain suggestions and gain good
advice, support, and assistance without criticism,
ultimately improving social qualities (Edelman &
Mandle, 2010).
In the treatment group there were elderly people
whose social quality category was the same as
before the intervention. This is because the elderly
people were not paying enough attention during the
intervention and they had an elementary school
educational background so had less ability to absorb
the provided health education. Furthermore, in the
control group there were elderly people whose
psychological qualities increased, although they did
not recieve any intervention. This is because the
elderly respondents’ personalitieare likely to gather
and interact with other elderly people.
4.4 Spiritual Quality
Table 8 indicates that before being given the health
education using the elderly mental health smart book
(BISAA), half of the respondents in the treatment
group had good spiritual qualities, such as often
feeling that worship activities would help his life be
better, hoping and believing God would help with
his life, and amazement about God's creation. The
pre-test in the control group showed that half of the
respondents also had good spiritual qualities.
After being given health education using the elderly
mental health smart book (BISAA), it was
determined that the spiritual quality in the treatment
group all experienced improvement, and took part in
activities such as worshipping every day, often
feeling that the worship activities helped to improve
life, always hoping and believing that God will
support life, and always feel amazed by God’s
creation. A post-test of the spiritual qualities in the
control group showed that the majority of
respondents (82.5%) did not change, and took part in
activities such as worshipping every day, often
feeling that the worship activities helped to improve
life, always hoping and believing that God will
support life, and always feel amazed by God’s
creation.
Mubarak (2007) describes health education as a a
dynamic process of behavior change. Stress
management can improve spiritual qualities because
one of the stress management strategies is to
participate in spiritual practice by being closer to
God Almighty through the practice of worship such
as prayer, fasting, praying, and attending recitation
(Edelman & Mandle, 2010).
In the control group there were elderly people
whose spiritual qualities increased despite not
receiving intervention. This is because some elderly
personalities are always obedient to God and
continually participate in worship.
5 CONCLUSIONS
Health education using the elderly mental health
smart book (BISAA) has an influence on the
improvement of physical, psychological, social and
spiritual qualities in the elderly, and most
significantly with psychological qualities.
Health officers can conduct health education at
the Elderly Integrated Service Post (Posyandu) with
the elderly mental mealth smart book (BISAA) to
help improve the physical, psychological, social, and
spiritual qualities of the elderly. Future researchers
could identify the influence of the elderly mental
health smart book (BISAA) on the improvement of
environmental qualities in the elderly.
REFERENCES
Azizah, L. M. (2011). Keperawatan Lanjut Usia Edisi
Pertama. Yogyakarta: Graha Ilmu.
Depkes RI. (2009). Pedoman Pelayanan Kesehatan Jiwa
Usia Lanjut Edisi 2. Jakarta: Depkes Ditjen Pelayanan
Medik.
Edelman, C. L. & Mandle, C. L. (2010). Health Promotion
throughout the Life Span. Missouri: Mosby Elvesier.
Handoyo. (2004). Meditasi. Jakarta: Gramedia.
Hardianti, H. (2014). Pengaruh Sense of Humor Terhadap
Kualitas Hidup pada Lansia Pensiunan di Kota
Malang. Skirpsi. Malang: Universitas Brawijaya.
Hutapea, R. (2005). Sehat dan Ceria di Usia Senja.
Jakarta: PT Rineka Cipta.
Idris, H., Bidjuni, H. & Karundeng, M. (2015).
Perbandingan Antara Penerapan Terapi Okupasi dan
Logoterapi terhadap Tingkat Stress Lansia di Panti
Werdha Damai Perkamil Kecamatan Ranomuut
Manado dan panti Werdha Senja Cerah Paniki
Kecamatan Mapanget Manado. ejournal
keperawatan(e-Kp) Volume 3, Nomor 2.
http://ejournal.unsrat.ac.id/index.php/j
kp/article/viewFile/8298/7857. Retreived 22 April
2016.
Imaddudin, A. (2015). Mengembangkan Kesejahteraan
Spiritual Peserta Didik Sebagai Katalis Bangsa
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
386

Inovatif. PEDAGOGIK Vol. III, No. 1. http://ejournal-
unisma.net. Retreived 28 April 2016.
Kementrian Kesehatan Republik Indonesia. (2013).
Pentingnya Peran Masyarakat dan Keluarga dalam
Meningkatkan Kualitas Hidup Lansia. Jakarta.
www.depkes.go.id. Retreived 7 April 2016.
Kementrian Kesehatan Republik Indonesia. (2013).
Populasi Lansia Diperkirakan Terus Meningkat
Hingga Tahun 2020. Jakarta. www.depkes.go.id.
Diakses pada tanggal 7 April 2016.
Kementrian Kesehatan Republik Indonesia. (2013). Triple
Burden Ancam Lansia. Jakarta. www.depkes.go.id.
Retreived 7 April 2016.
Kementrian Kesehatan Republik Indonesia. (2016). Lansia
yang Sehat, Lansia yang Jauh dari Demensia. Jakarta.
www.depkes.go.id. Retreived 7 April 2016.
Losyk, B. (2005). Kendalikan Stres Anda! Cara
Mengatasi Stres dan Sukses di Tepat Kerja. Jakarta:
PT Gramedia Pustaka Utama.
Mubarak, W. I. (2007). Promosi Kesehatan Sebuah
Pngantar Proses Belajar Mengajar dalam
Pendidikan. Yogyakarta: Graha Ilmu.
Skevington, S. M., Gunson, K. S. & O’connell, K. A.
(2013). Introducing the WHOQOL-SRPB BREF:
developing a short-form instrument for assessing
spiritual, religious and personal beliefs within quality
of life. Quality of Life Research, 22 (5). pp. 1073-
1083. ISSN 0962-9343.
http://opus.bath.ac.uk/31070/1/Skevin
gton_Quality_of_life_research_2012.p df. Retreived
28 April 2016.
Sukadiyanto. (2010). Stress dan Cara Menguranginya.
Cakrawala Pendidikan, Th. XXIX, No. 1.
https://core.ac.uk/download/files/335/ 11061911.pdf.
Retreived 9 Mei 2016.
Swarth, J. (2006). Stress and Nutrition. Jakarta : Bumi
Aksara.
WHO. (2013). World Health Organization
http://www.who.int//sunstanceabuse/researchtools.
Retreived 22April 2016.
Yusuf, A., Fitryasari, R. & Nihayati, H. E. (2015). Buku
Ajar Keperawatan Kesehatan Jiwa. Jakarta: Salemba
Medika.
The Impact of Using the Mental Health Smart Book (BISAA) to Increase Physical, Psychological, Social, and Spiritual Life Qualities in the
Elderly
387
