
Quality of Life in Patient Post Percutaneus Coronary Intervention
(PCI)
Siti Lestari and Tri Sunaryo
Nursing School of Polytechnic of Health, Surakarta, Indonesia
Keywords: Myocardial Infarction, Percutaneus Coronary Intervention, Quality of Life.
Abstract: Acute myocardial infarction is the result from the occurrence of acute coronary occlusion with prolonged
ischemia, then ultimately causes cell damage and myocardial infarction. To overcome stenosis or narrowing
the blood vessel, it need a PCI or Percutaneus Coronary Intervention. These conditions often have impact on
the quality of life. This study was intended to identify factors that affecting the quality of life of patients
myocardial infarction treated with PCI. This cross-sectional study was conducted among 30 respondents
who participated in this study. Chi-square was conducted to analyze the effect of age, marital status, social
support and coping mechanism toward the quality of life with α = 0.05. Statistical test result showed the
relationship of gender and QoL obtained p = 1.00, age and QoL p = 0.72), married status and QoL
p = 1.00, and coping mechanism and QoL p = 0.003. We can conclude that there was relationship
between social support, coping mechanism and the quality of life, but no relationship between age, sex,
marital status and the quality of life.
1 BACKGROUND
Acute myocardial infarction is a disease which affects
the patient in a to a great degree distressing way. It
is described as a threat that leads to a life crisis in
one's entire life and it is additionally a high family
stretch particularly for the couple (Eriksson, 2010).
The frequency of AMI is high and it is the main
source of death in the elderly moreover. According to
WHO in the world 14 million people die annually
(WHO, 2011). Myocardial infarction is also known
as heart attack. It is a condition of heart muscles death
when one or more coronary arteries which supply
oxygen-rich blood to the heart muscle turns out to be
all of a sudden blocked (Compare & Zarbo, 2013).
Blockage results from plaques made of fats and
cholesterol. The accumulation of this plaque is known
as coronary artery disease. The accumulation of
plaque is a process and also can produce chest pain
symptom known as angina pectoris (Herman &
Walsh, 2011). A myocardial infarction occurs when
a plaque burst all of a sudden and it causes a fast
aggregation of coagulating factors at the crack site
which drives a sudden block of blood stream in the
coronary supply route. Sudden obstruction prevents
blood reaching the heart muscle. The heart muscles
start to die if there is no vital supply of oxygen-rich
blood. The longer the obstruction persists, the greater
the amount of heart muscle dies.
Myocardial Infarction is a medical emergency. If
not treated on time it may lead changeless harm of
heart muscles (Linda F. Browna, Kurt Kroenkeb, C,
Dale E. Theobaldd, Jingwei Wub, C, And Wanzhu
Tub, 2011) and Maddox, 2011). Some of the
medical management used in this case are oxygen
inhalation ,anti arrhythmic drugs, in severe cases
administer I/V Morphine sulphate and diazepam as
required, I/V Heparin to prevent from
thromboembolism but it is not necessary for mild
case, pain relief (Nitro-glycerin for active pain),
prevention and treatment of any complications that
may arise, Immediate administration of aspirin and
physical exercises ought to be limited. The other non-
surgical treatment is angioplasty which is also known
as Percutaneus Coronary Intervention (PCI) (Linda F.
Browna, Kurt Kroenkeb, C, Dale E. Theobaldd,
Jingwei Wub, C, And Wanzhu Tub, 2011).
Health-related quality of life is an increasingly
important outcome measure in the management and
care of patients with chronic diseases, such as
myocardial infarct, coronary artery disease (CAD),
when the main treatment aim is not only to reduce
mortality rates, but also to enhance indications and
78
Lestari, S. and Sunaryo, T.
Quality of Life in Patient Post Percutaneus Coronary Intervention (PCI).
DOI: 10.5220/0008320800780083
In Proceedings of the 9th International Nursing Conference (INC 2018), pages 78-83
ISBN: 978-989-758-336-0
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

capacity to perform day by day exercises. Health-
related quality of life in nature is multifaceted, in
view of the subjective impression of patient's health,
and incorporates physical as well as mental and social
functioning.
Various studies related to quality of life have been
done, but there has not found a specific research on
the factors influence the quality of life of patients
AMI with PCI, especially research that conducted by
nurses. Nurses have a very important role in the long
term, by knowing the results of research on factors
that affect the quality of life, nurses can arrange
interventions to improve quality of life , so that
nursing intervention becomes more comprehensive
and can improve restoration, and quality of life of
AMI patient after PCI
The majority of scientific literature indicates that
health-related quality of life in AMI patients
significantly improves over a half year after intense
acute coronary; nonetheless, the magnitude of
changes in quality of life is once in a while surveyed
It has been suggested that improvement in health-
related quality of life may shift contingent upon
patients’ age, gender, or treatment method. This study
aims to identify the relationship between gender, age,
marital status, social support, coping and quality of
life in patient post PCI.
2 METHODS
A survey method using cross-sectional research
design was utilized in this study. Samples were 30
patients Myocardial Infarct treated with minimum 3
months post PCI, selecting by purposive sampling
with certain criteria. Data collection of this study was
carried out for 4 months from May to August 2017.
The instrument measuring quality of life was adopted
from the 36-Item Short Form Survey Instrument (SF-
36). Descriptive statistics and inferential statistics
were applied to the data. Paired T test was used to
analysis the influence of age and quality of life, while
to analyze the influence of gender, marital status,
mechanism coping and social support toward quality
of life, statistical was used Chi-square.
3 RESULTS
There were about 30 patients participated in this
study. Most of them were male, and the quality of life
as shown in the following table 1. From Table 1 we
can see that 60% or 18 people has a good quality of
life, while the remaining 40% (12 people) is very
good. Most of respondents in the study was male 21
people or 70%, while 9 people (30%) was female.
Table 2 depicts a cross tab analysis on association
between gender and quality of life among patient MI
with PCI. In the whole, the result shows that male had
good quality of life for 13 people (61.9%) and quality
of life was very good 8 people (38.1%), while female
had good quality of life as many as 5 people (55.6%)
and 4 people (44.4%) with excellent quality of life.
Based on the statistical test results obtained p value of
1.00 (α = 0.05) so it can be concluded that gender is
not related to quality of life.
Table 3 display the distribution of respondent by
age. The average age of respondents was 51 years
with a standard deviation of 9.4 years. The youngest
age is 30 years old and 70 years old. Further analysis
was conducted to determine the association between
age and quality of life, as show in the following Table
4 that showed the average age of respondents with
good quality of life was 50.67 years with a standard
deviation of 10.33 years, whereas in patients with
excellent quality of life the average age was 52.17
with a standard deviation of 8.19. Statistical test
results obtained p value of 0.72 means age factor is
not related to quality of life.
From Table 5 we can see that most of the
respondents were married with 28 people or 93.3%,
while 2 people (6.7%) were not married. Result
analysis to prove the relationship between marital
status and quality of life could be see in Table 6.
Statistical test results obtained p value of 1.00 (α =
0.05) so it can be concluded that married status is not
related to quality of life.
Table 7 reports the mechanism coping of
respondents. More than half percent or 16 people
(53.3%) have excellent coping mechanism, 12 (40%)
have good coping mechanism, while 2 people (6.7%)
have medium coping mechanism. Result of Statictical
analysis can be seen in Table 8. Table 8 indicate that
respondents with medium degree coping mechanisms
have good quality of life (100%). While respondent
with good coping mechanism is 11 people (91.7%)
and have good quality of life and 1 person (8.3%)
very good. Respondents with excellent coping
mechanism have good quality of life 5 people
(31.3%) and 11 people (68,8%) are very good.
Furthermore, in statistical test the relationship
between coping mechanism and quality of life
obtained p = 0.003 , so it can be concluded that coping
mechanism related to quality of life. Then, people
with good coping mechanisms have a 0.67 chance to
improve quality of life.
Quality of Life in Patient Post Percutaneus Coronary Intervention (PCI)
79
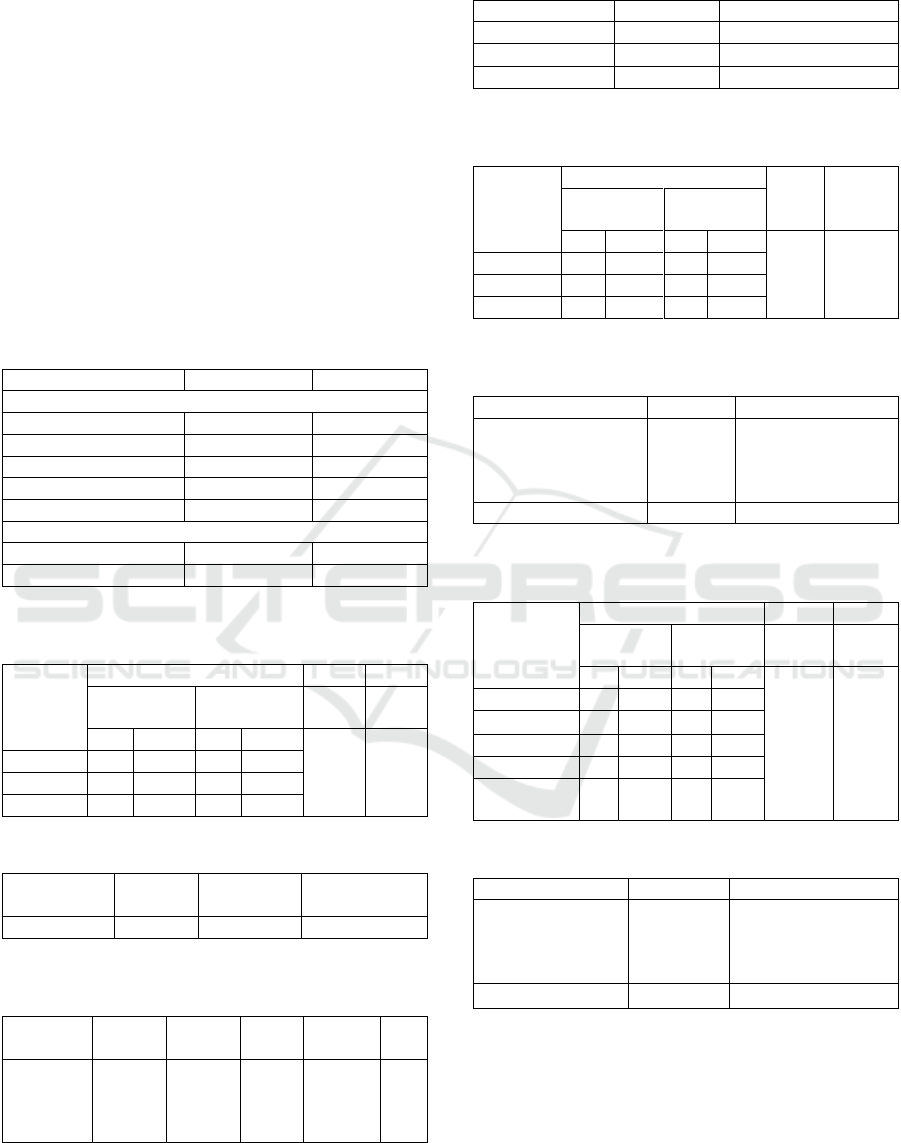
Table 9 displays half of all respondents had a good
of social support, while 10 people (33.3%) had very
good social support and 5 (11.7%) had moderate
social support. Respondents with the level of social
support are having good quality of life of 5 people
(100%) and the respondent with social support at
good level has good quality of life 12 (80%) and 3
(20%) very good. While respondents with very good
social support level have quality of life good 1 person
(90%) and 9 person (90%) very good. In the statistical
test the relationship of social support and quality of
life obtained p value 0,000 so it can be concluded that
social support is related to quality of life. And people
with good social support have a 0.67 chance to
improve the quality of life.
Table 1: Distribution of respondents
Category
Frequency
Precentage
Quality of Life
Not Good
0
0
Moderate
0
0
Good
18
60
Very Good
12
40
Total
30
100
Gender
Male
21
70
Female
9
30
Table 2: Cross tab analysis between gender and quality of
life
Gender
Quality of life
OR
P
good
very good
95%
CI
Va
lue
N
%
N
%
1.3
1.00
Male
13
61.9
8
38.1
Female
5
55.6
4
44.4
Total
18
60
12
40
Table 3: Distribution of respondents by age
Variabel
Mean
Standar
Deviasi
Minimal
Maksimal
Age
51.4
9.40
30-70
Table 4: The average age of respondents with good quality
of life
Quality
of Life
Mean
SD
SE
P
Value
N
Good
Very
good
50.89
52.17
10.33
8.19
2.44
2.36
0.72
18
12
Table 5: Distribution of respondents by marital status
Marital Status
Total
Precentage
Married
28
93.3
Not married
2
6.7
Total
30
100
Table 6: Cross tabulation analysis on association between
marital status and quality of life
Marital
status
Quality of life
OR
P
Good
Very good
95%
CI
Value
N
%
N
%
1.55
1.00
Married
17
60.7
11
39.3
no marry
1
50
1
50
total
18
60
12
40
Table 7: Respondent distribution based on level of
mechanism of coping
Coping Mechanism
Total
Procentage
Not Good
Moderate
Good
Excellent
0
2
12
16
0
6.7
40.0
53.3
Total
30
100
Table 8: Cross tabulation between coping mecanism and
quality of life
Coping
Mechanism
Qualiy of Life
OR
P
Good
Very
Good
95%
CI
Value
N
%
N
%
0.67
0.003
less
0
0
0
0
moderate
2
100
0
0
good
11
91.7
1
8.3
very good
5
31.3
11
68.8
total
18
60
12
40
Table 9: Distribution of respondents based on social support
Social Support
Total
Precentage
Not Good
Moderate
Good
Very Good
0
5
15
10
0
11.7
50.0
33.3
Total
30
100
4 DISCUSSION
The mean age of respondents was 51.4 years with a
standard deviation of 9.40. The youngest age 30
years and oldest 70 years. This indicates that the age
of the respondent is in the early adult range to the
elderly, where the range is at risk for experiencing
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
80

various diseases, including myocardial infarction.
According to basic health research data 2013, the
prevalence of coronary heart disease increases with
age, the highest at age 65-74 years.
The results of this study are in line with a study
conducted on 88 patients by (Panthee, Kritpracha, &
Chinnawong, 2011) that the average of coronary
heart disease patients was 57.43, with the youngest
age 28 years and the oldest 85 years. Another study
conducted Wang et al., (2016), of 128 patients
indicated that the average patient aged 55.4 with a
standard deviation of 9.5. Similarly, in a study
conducted Kroemeke, (2016) the mean age of heart
patients was 52.26 with a standard deviation of 7.08.
Furthermore, the study conducted by (Ginny Brunton
et al., 2015) describes the age factor as a isk factor.
Statistical test results obtained p value of 0.72, it
means that age factor is not related to quality of life.
This is in line with a study conducted by Ruijie Li, et
al, (2012) on 624 MI patients with PCI with 60 years
of age (73.6%), 60-79 years (55.7%) and over 80
years (21.3%). The result is that older patients
experience an increase in physical health best
compared to younger.
According Rubbyana (2012) that quality of life is
a subjective perception of the individual against the
physical, psychological, social, and environmental
conditions in everyday life that happened. WHO
describes the quality of life as an individual
perception of their position in life in the context of the
culture and value system where they live and live in
relation to their life goals, expectations, standards and
the focus of their lives. This concept covers several
broad dimensions: physical health, psychological
health, social and environmental relations.
Most of the gender in this study were men, 21
people or 70%. This happens because men have a risk
of heart disease than women. This is also in line with
a research conducted by Bosworth in 2000 with 4278
patients and 63% of whom are men. Similarly, studies
conducted by (Panthee, Kritpracha, & Chinnawong,
2011) on 88 patients and 72.7% of them are men. The
data suggest that men are at greater risk than women.
This is in accordance with a study conducted by (N,
Suryadipradja, & Shatri, 2005), that MI occurs mostly
in men compared with women with a ratio of 2.5-3:
1.
Then, Statistical test results obtained p value of
1.00 (α = 0.05) so it can be concluded that sex is not
related to quality of life. This is in line with research
conducted by (Kristofferzon ML, Löfmark R, 2005)
that there is no difference in the quality of life
between men and women. Similarly, the study
conducted by Kose and Martha, 2016 showed no
difference in the quality of life between men and
women. Similarly, the study conducted by (Kose, &
Marta, 2016) showed no difference in the quality of
life between men and women.
Judging from the marital status, most of the
patients were married and still have a partner of 93%
and do not have a partner as much as 7%. This result
is in accordance with the study conducted by Chan,
Chau & Chang, 2005 from 115 patients 80% in
married status.
Furthermore, statistical test results obtained p
value of 1.00 (α = 0.05) so it can be concluded that
married status is not related to quality of life.
However, since the partner is one of the support
systems that will be able to provide positive support
for the partner and will decrease anxiety, as the study
conducted by (Panthee, Kritpracha, & Chinnawong,
2011) patients who have no partner found more
anxiety than those who have a partner.
Coupling mechanism is a pattern to withstand
tensions that threaten him or solve problems. The
existence of personal and life-threatening problems
will lead to both adaptive and non-adaptive reactions,
where the problem will create anxiety for the
individual. This is in accordance with the opinion of
Kroemeke (2016) that experience or experience life-
threatening diseases such as MI will certainly lead to
stress.
Furthermore, strategies typically used by
individuals include coping that focuses on problem
solving or problem solving focused coping, as
strategies where individuals are actively seeking
problem solving to eliminate stressful conditions or
situations. In addition, other strategies that can be
used are emotionally focused or emotion-focused
coping, where the individual involves attempts to
regulate his emotions in order to adapt to the impact
that will result in a condition of stress. The way the
individual handles stressful situations is determined
by the individual's own resources and how much
stress he experiences (Ahyarwahyudi, 2010).
In statistical test, the relationship between coping
mechanism and quality of life obtained p value 0.003
so that it can be concluded that coping mechanism
related to quality of life, with positive correlation, the
better coping mechanism the higher quality of life
client. Furthermore, people with good coping
mechanisms have a 0.67 chance to improve quality of
life. This is in accordance with studies conducted
Panthee, Kritpracha, & Chinnawong, (2011) that
coping is correlated with quality of life. Coping
mechanism especially coping strategy-oriented
problem or problem focused coping related to the
quality of life, especially the dimensions of function
Quality of Life in Patient Post Percutaneus Coronary Intervention (PCI)
81

and health. In this case, more men use this strategy
than women. The study also found that problem
focused coping strategies have a positive effect while
coping strategies avoid having negative effects. In
males, according to Kristofferzon ML, Löfmark R
(2005) often coping mechanisms are optimistic, self-
reliant and confrontational. Nevertheless, the study
conducted by Kose, & Marta (2016) showed different
results, there was no significant correlation between
quality of life with coping strategies in men and
women.
Social support will be effective in treating
psychological pressures in difficult times and
pressing, for example in MI patients often experience
distress and anxiety. The prevalence of anxiety and
depression in MI varies (Wang et al., 2016) Social
support also helps strengthen immune function,
reduce physiologic responses to stress and strengthen
functions to respond to chronic diseases (Taylor &
Broffman, 2011).
The result of statistical test on the relationship
between social support and quality of life is obtained
p value 0,000, so it can be concluded that social
support is related to quality of life. People with good
social support have a 0.67 chance to improve the
quality of life. The results of this study are in line with
the study conducted by (Lett HS, Blumenthal JA,
Babyak MA, Catellier DJ, Carney RM, Berkman LF,
Burg MM, Mitchell P, Jaffe AS, 2007) that positive
social support is associated with improving quality of
life and increasing outcomes of patients with
Coronary Heart Disease. Furthermore, Chung,
Moser, Lennie and Rayens, 2009 explain the lack of
social support and depression affect the decline in
quality of life. Social support will improve the quality
of life if depression is also handled properly.
5 CONCLUSIONS
There is no relationship between age, gender and
marital status with quality of life of MI patients with
PCI. On the other hand, study found that there was
relationship between social support, coping
mechanism with quality of life of MI patients with
PCI.
REFERENCES
Ahyarwahyudi (2010). Mekanisme Koping.
http://Aharwahyudi, Wordpress
Brunton, Ginny, Caird, Jenny, Sutcliffe, Katy, Rees,
Rebecca, Stokes, Gillian, Oliver, Sandy, et al. (2015).
Depression , anxiety , pain and quality of life in people
living with chronic hepatitis C A systematic review and
meta-analysis. Interpretation A Journal Of Bible And
Theology, (2301).
Compare, A., & Zarbo, C. (2013). Social support ,
depression , and heart disease : a ten year literature
review. Compare A Journal Of Comparative
Education, 4(July), 1-7. doi:
10.3389/fpsyg.2013.00384.
Eriksson, M. (2010). Recovery From An Acute Myocardial
Infarction – A Longitudinal Study Of Couples Recovery
From An Acute Myocardial Infarction –.
Herman, P. M., & Walsh, M. E. (2011). Hospital
Admissions for Acute Myocardial Infarction , Angina ,
Stroke , and Asthma After Implementation of Arizona ’
s Comprehensive Statewide Smoking Ban. American
Journal of Public Health, 101(3), 491-496. doi:
10.2105/AJPH.2009.179572.
Kose, Peter Anita & Marta, S. L. (2016). KOse and Martha.
International Journal of Nursing Education and
Research, 4(1), 6. doi: 10.5958/2454–
2660.2016.00001.6.
Kristofferzon ML, Löfmark R, C. M. (2005). Coping, social
support and quality of life over time after myocardial
infarctionCoping, social support and quality of life over
time after myocardial infarction. Journal of Advanced
Nursing . 2005 Oct;52(2):113-24, 113-24. doi: DOI:
10.1111/j.1365-2648.2005.03571.x.
Kroemeke, A. (2016). Changes in well-being after
myocardial infarction : Does coping. Quality of Life
Research, 25(10), 2593-2601. Springer International
Publishing. doi: 10.1007/s11136-016-1286-6.
Lett HS, Blumenthal JA, Babyak MA, Catellier DJ, Carney
RM, Berkman LF, Burg MM, Mitchell P, Jaffe AS, S.
N. (2007). Social support and prognosis in patients at
increased psychosocial risk recovering from
myocardial infarction. Health Psychol. 26(4):418-27,
(July), 418-27. doi: 10.1037/0278-6133.26.4.418.
Linda F. Browna, Kurt Kroenkeb, C, Dale E. Theobaldd,
Jingwei Wub, C, And Wanzhu Tub, C. (2011). The
Association of Depression and Anxiety with Health-
Related Quality of Life in Cancer Patients with
Depression and/or Pain, 19(7), 734-741. doi:
10.1002/pon.1627.The.
N, H. R. K. H., Suryadipradja, H. R. M., & Shatri, H.
(2005). The Influence of Depression on The Quality of
Life of Male Patients Post Acute Myocardial Infarct.
Depression.
Panthee, B., Kritpracha, C., & Chinnawong, T. (2011).
Correlation between Coping Strategies and Quality of
Life among Myocardial Infarction Patients in Nepal.
Nursing, (Mi), 187- 194.
Rubbyana, U. (2012). Hubungan antara Strategi Koping
dengan Kualitas Hidup pada Penderita Skizofrenia
Remisi Simptom, 1(02), 59-66.
Taylor, S. E., & Broffman, J. I. (2011). Psychosocial
Resources : Functions , Origins , and Links to Mental
and Physical Health. Advances, 44, 1-57. Elsevier Inc.
doi: 10.1016/B978-0-12-385522-0.00001-9.
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
82

Wang, W., Chow, A., Thompson, D. R., Koh, K.,
Kowitlawakul, Y., & He, H.-gu. (2016). Predictors of
Health- Related Quality of Life Among Patients With
Myocardial Infarction. Western Journal of Nursing
Research. doi: 10.1177/0193945914546201.
Quality of Life in Patient Post Percutaneus Coronary Intervention (PCI)
83
