
Advanced Care Planning: An Educational Intervention for the
Elderly in Indonesia
A Pilot Randomized Controlled Trial
Rista Fauziningtyas
1
, Joni Haryanto
1
and Suhartono Taat Putra
2
1
Faculty of Nursing Universitas Airlangga, Kampus C Mulyorejo, Surabaya, Indonesia
2
Faculty of Medicine Universitas Airlangga, Kampus A Jl Mayjen Prof. Dr. Moestopo 47 Surabaya, Indonesia
Keywords: Advanced Care Planning, Palliative Care, Dementia, Cognitive Impairment, Education, Nursing, Elderly.
Abstract: Discussions involving Advanced Care Planning (ACP) can be challenging in the setting of early dementia.
In this study, we aimed to evaluate an educational intervention that focused on ACP in elderly people with
mild cognitive impairment in Indonesia. This small pilot study used a randomized control trial design. A
total of 19 respondents with mild cognitive disorders were recruited and randomly assigned to either an
experimental (video, discussion, and print material) or control group (print material alone). Knowledge of
ACP, confidence in making end-of-life decisions, and care preferences were compared between the two
groups. A significant increase was noted in knowledge (p = 0.002) and confidence (p = 0.003), yet
regarding preferences, only 30% of respondents in the experimental group completed the ACP
documentation, and therefore limited conclusions could be made. Providing information in different formats
to people with a mild cognitive impairment may increase their ability to participate in ACP. Further research
is needed involving greater numbers of respondents.
1 BACKGROUND
Respecting the choices that elderly people make,
regarding treatment preferences, is an important
component of end-of-life care. Advanced Care
Planning (ACP) is a mechanism by which health
care professionals can broach sensitive discussions
concerning death, dying, and document care
preferences. ACP is a process that focuses on the
individual and commonly involves healthcare
professionals (doctors, nurses, psychologists, and
social workers) and ideally family members
(Robinson et al., 2012; Abel et al., 2013; Blackford
& Street, 2013). The purpose of ACP is to document
care preferences and appoint a surrogate decision
maker if a person can no longer make decisions for
themselves (Schaeffer, 2011).
An important element of ACP is clarifying a
person’s knowledge of their condition, treatments,
beliefs, and identifying their wishes regarding care
(Volandes et al., 2009; Deep et al., 2010). However,
such discussions are often taboo in almost all
countries in the Asia Pacific region (Con, 2008;
National Hospice & Palliative Care Organization,
2009), including Indonesia. This hesitancy to discuss
death and dying relates to cultural values and beliefs.
For example, in the Philippines, many people
believe that the future, including death, is in the
hands of God and therefore making plans for the
end-of-life care, including discussions regarding
ACP, would be usurping God’s authority and this is
unacceptable (Con, 2008). In Indonesia, end-of-life
discussions usually occur informally when reciting
the Al- Qur’an. Consequently, in Indonesia,
healthcare professionals, and carers alike, must
discuss end-of-life issues with great sensitivity so
they do not offend. Death is a universal phenomenon
regardless of age, and, therefore, talking about death
and dying is vital to the success of ACP (Silveira &
Forman, 2012). While carrying out effective ACP
for the elderly can be challenging, especially when
in the presence of cultural taboos and cognitive
decline, it is necessary for a “good” death to occur
(Lim et al., 2012; Davies et al., 2014).
In Indonesia, the improvement in healthcare
facilities and the growing economy has led to an
increase in the standard of living and life expectancy
amongst its citizens (Kementerian Kesehatan RI,
2014). These improved conditions have led to an
Fauziningtyas, R., Haryanto, J. and Putra, S.
Advanced Care Planning: An Educational Intervention for the Elderly in Indonesia.
DOI: 10.5220/0008320600670072
In Proceedings of the 9th International Nursing Conference (INC 2018), pages 67-72
ISBN: 978-989-758-336-0
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
67

increase in the proportion of elderly people in the
population. As a consequence, various chronic
diseases of aging such as hypertension,
osteoarthritis, and, importantly, cognitive
impairment and dementia have increased (WHO,
2011). Cognitive impairment can make the elderly
feel powerless when they are facing the end of life
(WHO, 2011). One solution to minimizing this sense
of powerlessness in the elderly is to introduce an
Advance Care Planning information session into
nursing homes (Volandes et al., 2009; Deep et al.,
2010).
Traditionally in Indonesia, healthcare
professionals verbally deliver information about the
end of life. This delivery method has limited
success, especially when the person is elderly. This
failure may be because the aging process can affect
sight and hearing (Nugroho, 2008). In addition, the
degree to which people understand verbal
descriptions concerning complex medical conditions
depends on their level of health (Volandes et al.,
2009). To overcome this problem, delivering
information in several formats has been shown to
improve health literacy. In a previous study in
Australia, a video decision support tool for advanced
dementia seemed to improve communication and
decision making for patients by helping them to
visualize future health states (Volandes et al., 2009;
Deep et al., 2010; Gjerberg et al., 2015). However, it
is still unknown how the video qualitatively altered
the client’s cognition regarding their future care.
This work will add information regarding cognition
in the elderly after the use of the video decision
support tool. People have different methods of
learning. Some can receive information better
visually, others through auditory means, or through a
certain sense (Franzoni & Assar, 2009). These
methods are affected by age, experience, physiology,
culture, and many other factors. Powerful media and
visualization techniques have shown to create lasting
memories and improve recall (Bert P.M. Creeemers
& Creemers, 2007; Franzoni & Assar, 2009). There
is no research to date that explores ACP discussions
amongst the elderly with an early cognitive decline
in Indonesia. Hence this study aims to address this
gap.
2 METHODS
2.1 Study Design
The researcher used a pilot experimental research
design with a randomized control group and a pre-
test/post-test design. The control group received
standard care from the participating nursing home
and a general information booklet on ACP. The
experimental group received the modified ACP
stages 1: introduction about end-of-life care and
dementia; and 2: discussion about end-of-life
preferences and progress of the disease.
2.2 Study Population, Sampling, and
Procedure
The population in this study were elderly people
who lived in a private nursing home in Surabaya,
East Java, Indonesia. There were 19 respondents:
nine in the control group and ten in the experimental
group. The inclusion criteria were as follows: had a
score of 17 or more on the Mini-Mental State Exam,
indicating that they were cognitively able to consent
to the study, were able to complete the first two
stages of the ACP program, speak either Indonesian
or Javanese, and have no major vision or hearing
issues. The exclusion criteria were moderate to
severe dementia, and/or other psychological
disorders such as schizophrenia. Simple random
sampling was the sampling technique used for this
study. The collection of data occurred over a two-
month period from May to June 2014. The ACP
Phase 1 intervention was provided during two
meetings per week for four weeks, and was
delivered as a group presentation. The information
for ACP Phase 2 was delivered in one meeting per
week for two weeks. These latter meetings consisted
of counseling and discussions and involved
respondents, researchers, and nursing personnel.
2.3 Intervention
Modifications of the ACP information included
additions made to the information booklet, a video,
and a narrated PowerPoint presentation. The two
videos used in this study were: 1) the video
"Advanced Stage Dementia," taken from research
conducted by Volandes et al. (2009); the duration of
the video is two minutes and 12 seconds; and 2) the
video "ACP”; this video was taken from the Agency
for Integrated Care (AIC), Taiwan, with a duration
of six minutes and seven seconds.
2.4 Measures
The primary outcomes were knowledge and
confidence. To measure these, questionnaires were
used. The questionnaires, investigating knowledge
and confidence, involved ten statements for which
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
68
the respondents had to answer true or false. The
questionnaires that focused on confidence contained
ten statements about the initiative of the elderly to
follow the ACP program, persistence in completing
the ACP program, and effort clients make in
achieving the expected results. The secondary
outcome included preferences regarding end-of-life
care. The questionnaire that focused on preferences
had only six items that allowed for open-ended
responses and could be completed either by the
researcher or the respondent. The questionnaire end
of life six questions, including the following
components: 1) the identity of the proxy; 2) valuable
things for the elderly; 3) hopes and fears of the
elderly; 4) medical care at the end of life; 5) the
place at the end of life; and 6) place of burial and
funeral. The instruments used in this study to
measure the effectiveness of the intervention were
developed by the researchers based on the literature
review and previous research.
2.5 Data Analysis
Data analysis was conducted using the following
statistical tests: 1) Mann Whitney (to determine the
different variables of knowledge and confidence,
before and after treatment, between the two groups);
2) Wilcoxon (to test the variables of changes in
knowledge and confidence before and after
treatment in each group). Researchers determined by
the degree of significance at p<0.05. End-of-life care
preferences were obtained through structured
interviews and are described in the results section.
2.6 Ethical Clearance
This study was certified for ethical clearance by the
Faculty of Public Health, Universitas Airlangga with
the number 86/KEPK, April 7, 2014.
3 RESULTS
Respondents involved in this study were aged
between 81 and 91 years of age. Their education
level was mostly high school or equivalent, and this
level of education was almost equal across the two
groups (50% in the experimental group and 44.44 %
in the control group). MMSE examination results
showed that 67% of the control group and 60% of
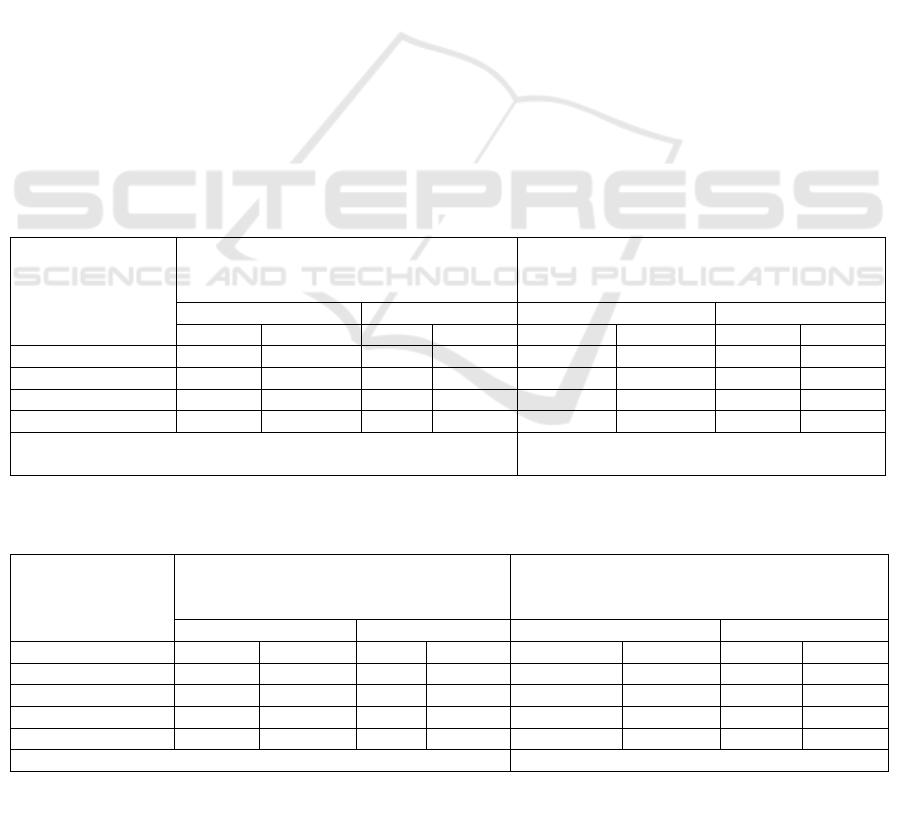
Table 1: Cross tabulation of pre-test and post-test evidence of respondents’ knowledge.
Knowledge
Control group Experimental group
Pre-test Post-test Pre-test Post-test
f% f%f %f %
Goo
d
0 0 1 11.11 0 0 10 100
Enou
g
h 7 77.77 6 66.66 10 100 0 0
Less 2 22.22 2 22.22 0 0 0 0
Total 9 100 9 100 10 100 10 100
Wilcoxon Signed Rank Test p = 0.317 (p>0.050) Wilcoxon Signed Rank Test p = 0.002
(
p
<0.050
)
*f = frequency
Table 2: Cross tabulation of pre-test and post-test evidence of respondents’ self-effication.
Confidence
Control group Experimental group
Pre-test Post-test Pre-test Post-test
f% f% f %f %
Hi
g
h 1 11.11 1 11.11 0 0 9 90
Moderate 7 77.77 8 88.88 10 100 1 10
Low 1 11.11 0 0 0 0 0 0
Total 9 100 9 100 10 100 10 100
Wilcoxon Signed Rank Test p = 0.317 (p>0.050) Wilcoxon Signed Rank Test p = 0.003 (p<0.050)
*f = frequency
Advanced Care Planning: An Educational Intervention for the Elderly in Indonesia
69
the experimental group had mild cognitive
impairment. There were only two types of religious
affiliations that the respondents identified across the
two groups; Islam (80% in the experimental group
and 67% in the control group) and Christian (20% in
the experimental group and 33% in the control
group). Most respondents were married. All
respondents were Indonesian with most from the
island of Java. The reasons for the respondents
entering the nursing home was largely due to their
wishes (60 % in the experimental group and 45 % in
the control group).
Based on Table 1, the good level of knowledge
of the respondents in the experimental group was
increased (n = 100%) compared to the control group
(n = 11.11%). The statistical test in the experimental
group showed there was a significant change of
respondents' knowledge with a p-value = 0.002
(p<0.050).
Moreover, Table 2 also showed a high level of
confidence in the respondents. In the experimental
group there was an increase (n = 90% compared to
the control group (n = 11.11%). The statistical test
for the experimental group showed there was a
significant change of respondents' confidence with a
p-value = 0.003 (p<0.050).
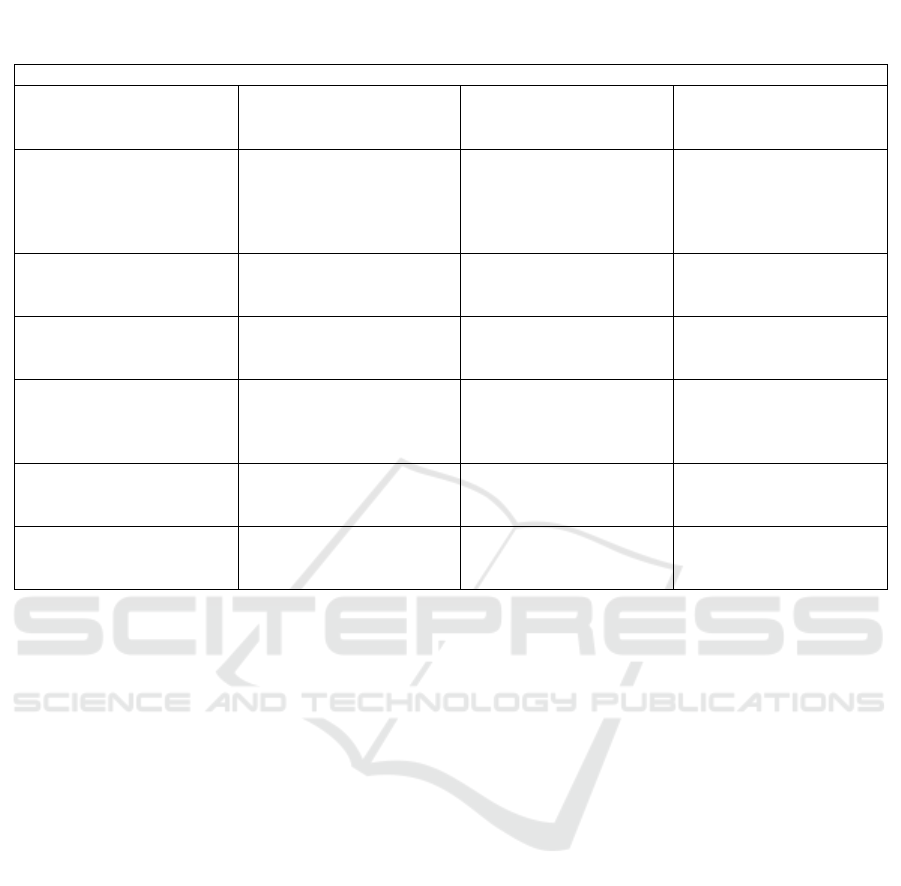
None of the respondents in the control group
could finish the question regarding end-of-life care
planning, while only 30% respondents in the
experimental group completed the same question.
The results of the discussion phase are explained in
Table 3.
4 DISCUSSION
In summary, the results of this research suggest that
changes in the method of giving information to the
elderly can increase knowledge and the confidence
to discuss treatment at the end of their lives. This
condition does not allow the elderly to convey their
desires regarding treatment at the end of life. Only
30% of the elderly can discuss their final treatment.
Most respondents submit all decisions regarding
late-life care to the family.
Based on the characteristics of the respondents,
both treatment groups were Indonesian and mostly
Javanese. The Javanese culture states that talking
about death is taboo and precedes the will of God
the Almighty, so talk of death is avoided by most
elderly people. Also, history indicates that most
elderly patients enter the home nursing by their own
free will. This indicates that elderly people still have
a very close relationship with their family; the
selection of end-of-life care must be discussed with
Table 3: The end-of-life care answer.
End-of-Life Care Plannin
g
1. The identity of the
proxy
60% had already chosen
the proxy
40% did not know
“My first sons are people
who are responsible for my
medical treatment and give
me money for this nursing
home.”
“I have five children, and
they will pay for my
financial needs. If I have
health problems they will
hold a
f
amil
y
meetin
g
.”
2. Valuable things for the
elderly
100% said the most
valuable thing in their life
is thei
r
family
3. Hopes and fears of the
elderly
80% of respondents said
they still have unfulfilled
expectations and fea
r
20% of respondents said
they have no fear
4. Medical care at the end
of life
30% of respondents chose
medical care that supports
a quality of life without
p
rolonging life
30% do not know about
medical care
40% respondents chose
medical care that
prolonging life
5. The place for the end
of life
50% of respondents chose
end-of-life treatment at
home with family
10% of respondents chose
end-of-life treatment at
the nursing home
40% of respondents chose
end-of-life treatment in
hospital
6. Place of burial and
funeral.
70% respondents have still
not made decisions for a
p
lace for
b
urial and funeral
30% respondents have
already chosen a place for
b
urial and funeral
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
70

the family. It is the cause of the elderly have not
chosen by complete end of life care. Based on
Indonesian culture, the elderly are important
members of the extended family. Their family,
especially their children, have a close relationship
with them (Riasmini, Sahar, & Resnawati, 2013), so,
every decision must be discussed with the family.
A third of the respondents who made the
selection are no different to the seven other
respondents regarding age, MMSE, or level of
education. Improved knowledge, self-affection and
behavior are also evident. This may be caused by
their health being less favorable than other
respondents. They already have limitations such as
difficulty in walking, accompanied by post-stroke
disorders. This is what allowed a third of
respondents to make a choice for end-of-life care.
The Asian culture allows discussion about a
person's chronic disease, but this is carried out by
health personnel and takes place with family or
people close to and not directly with the patient.
Family support is strongly associated with selection
decisions about end of life (Bravo et al., 2012; Lim
et al., 2012; Goodman et al., 2013). Lim et al. (2012)
also state that discussion regarding the end of life in
the Asian culture is still considered taboo. Modified
ACP stages 1 and 2 have helped respondents discuss
end-of-life healthcare, but respondents are still not
open to discussing it.
Stress affects perception response. In this study,
stress perception relates to knowledge and
confidence. Perceptual responses in this study are
the end-of-life preferences. This study showed no
difference in the theory. Improved knowledge and
changes in confidence are not concomitant with the
election of end-of-life care chosen by the elderly
(Putra, 2011). Knowledge and confidence in the
experimental group increased, but only a few
respondents could discuss end-of-life care planning.
This could be caused by the video provided not
being based on condition of Indonesian culture. So,
there are cultural factors that need to be considered
in the formation of perceptual responses. The
inability of the elderly to imagine the quality of their
lives under certain circumstances, the so-called
''paradoxical defect'', and the benefits and
disadvantages of the treatment received may be the
reason that not all elderly people are capable of
discussing and planning the end of their lives
(Volandes et al., 2009; Deep et al., 2010).
This study has several limitations. ACP
programs only used phase 1 and 2; phases 3–5 have
not been carried out due to the time constraints of
the study. Videos that were played by the
researchers were taken from Australia and Taiwan
with dialogue in English and Mandarin, so
respondents may have had difficulty understanding
the contents of the video, although it was translated
into Indonesian. Discussions during Phase 2 did not
include the family. A small number of respondents
were included because it was challenging to
persuade respondents to join this research. In the
future, a larger number should be included to
achieve more reliable results. Researchers advice on
further research includes involving the family in
Phase 2 of the ACP and create videos regarding
dementia and ACP based on Indonesian culture.
This would facilitate all respondents making end-of-
life care decisions. Nurses and nursing can motivate
the elderly to make plans for their end-of-life care
through the ACP modification program, as an
independent nursing intervention.
5 CONCLUSIONS
An accurate and timely discussion of diseases and
end-of-wlife care will help patients communicate
with family and loved ones. ACP can give the
elderly a real chance to have control over the
ultimate choice of their lives. By educating the
elderly on the topic of early treatment planning and
effectively communicating and involving the
families and medical personnel involved, nurses can
provide patients with the best opportunity to make
sure that others respect the final decision of their
life.
REFERENCES
Abel, J. et al. (2013) ‘The impact of advance care
planning of place of death, a hospice retrospective
cohort study,’ BMJ Supportive & Palliative Care,
3(2), pp. 168–173. doi: 10.1136/bmjspcare-2012-
000327.
Bert P.M. Creeemers and Creemers, B. P. M. (2007)
‘Combining different ways of learning and teaching in
a dynamic model of educational effectiveness,’
Journal of Basic Education, 17(1), pp. 1–39.
Blackford, J. and Street, A. F. (2013) ‘Facilitating advance
care planning in community palliative care:
conversation starters across the client journey,’
International Journal Of Palliative Nursing, 19(3), pp.
132–139. doi: 10.12968/ijpn.2013.19.3.132.
Bravo, G. et al. (2012) ‘Promoting advance planning for
health care and research among older adults: A
randomized controlled trial,’ BMC Medical Ethics.
BioMed Central Ltd, 13(1), p. 1. doi: 10.1186/1472-
Advanced Care Planning: An Educational Intervention for the Elderly in Indonesia
71

6939-13-1.
Con, A. (2008) ‘Cross-cultural considerations in
promoting Advance Care Planning. Canadian Insitute
of Health Research’. Available at:
www.bccancer.bc.ca.
Davies, N. et al. (2014) ‘Quality end-of-life care for
dementia: What have family carers told us so far? A
narrative synthesis.’, Palliative Medicine, 28(7), pp.
919–930. doi: 10.1177/0269216314526766.
Deep, K. S. et al. (2010) ‘“It helps me see with my heart”:
How video informs patients’ rationale for decisions
about future care in advanced dementia,’ Patient
Education and Counseling. Elsevier Ireland Ltd,
81(2), pp. 229–234. doi: 10.1016/j.pec.2010.02.004.
Franzoni, a. L. and Assar, S. (2009) ‘Student learning
styles adaptation method based on teaching strategies
and electronic media,’ Educational Technology &
Society, 12, pp. 15–29. doi: 10.1109/ICALT.2008.149.
Gjerberg, E. et al. (2015) ‘End-of-life care
communications and shared decision-making in
Norwegian nursing homes - Experiences and
perspectives of patients and relatives,’ BMC
Geriatrics. BMC Geriatrics, 15(1), pp. 1–13. doi:
10.1186/s12877-015-0096-y.
Goodman, C. et al. (2013) ‘Preferences and priorities for
ongoing and end-of-life care: A qualitative study of
older people with dementia resident in care homes,’
International Journal of Nursing Studies. Elsevier Ltd,
50(12), pp. 1639–1647. doi:
10.1016/j.ijnurstu.2013.06.008.
Kementerian Kesehatan RI (2014) Infodatin Lanjut Usia.
Lim, S. et al. (2012) ‘Advance Care Planning Guidelines
for working with Asian patients and their families’,
pp. 1–11.
National Hospice and Palliative Care Organization (2009)
Chinese-American Outreach Guide. Available at:
http://www.nhpco.org/sites/default/files/public/Access
/Chinese_American_Outreach_Guide.pdf.
Nugroho, W. (2008) Keperawatan Gerontik dan Geriatrik
3rd ed. Jakarta, Indonesia: EGC.
Putra, S. T. (2011) Psikoneuroimunologi kedokteran.
Surabaya: Pusat Penerbitan dan Percetakan Unair.
Riasmini, N. M., Sahar, J. and Resnawati, Y. (2013)
‘Pengalaman keluarga dalam penanganan lanjut usia
di masyarakat dari aspek budaya indonesia’, Journal
Ners, 8(1), pp. 98–106.
Robinson, L. et al. (2012) ‘A systematic review of the
effectiveness of advance care planning interventions
for people with cognitive impairment and dementia,’
Age and Ageing, 41(2), pp. 263–269. doi:
10.1093/ageing/afr148.
Schaeffer, B. Y. J. (2011) ‘Supporting End-of-Life
Decisions’, pp. 1–5.
Silveira, M. J. and Forman, J. (2012) ‘End-of-life care
from the perspective of primary care providers’,
Journal of General Internal Medicine
, 27(10), pp.
1287–1293. doi: 10.1007/s11606-012-2088-3.
Volandes, A. E. Et al. (2009) ‘Video decision support tool
for advance care planning in dementia: randomized
controlled trial’, BMJ, 338(may 28 2), pp. b2159–
b2159. doi: 10.1136/bmj.b2159.
WHO (2011) ‘Palliative Care for Older People: Better
Practices’, WHO Regional Office for Europe., pp. 1–
72.
INC 2018 - The 9th International Nursing Conference: Nurses at The Forefront Transforming Care, Science and Research
72
