
Potential Risk Factors of End Stage Renal Disease in Patients of
Hemodialysis
Diana Laila Ramatillah
1
, Syed Azhar Syed Sulaiman
2
, Amer Hayat Khan
2
, and Ihsanil Husna
3
1 Pharmacy Faculty, Universitas 17 Agustus 1945 Jakarta
2 School of Pharmaceutical Sciences, Universiti Sains Malaysia
3 Physician at Nephrology Ward at Cempaka Putih Islamic Hospital, Jakarta
Keywords: Potential Risk Factors, ESRD, Cardiovascular, Penang, Jakarta
Abstract: The purpose of this research is to evaluate potential risk factors and its correlation with probability of dying
and frequency of hemodialysis from the first treatment among hemodialysed patients in hemodialysis center
in Penang, Malaysia and Jakarta, Indonesia. A cohort prospective study was conducted in this research.
Universal sampling were used to select 178 and 78 patients who had been followed for 9 months in
Hemodialysis Center in Jakarta and Penang, respectively. Cox regression was used to analyze probability of
dying among these patients. In HD center Jakarta, Indonesia, 47 hemodialysed patients had cardiovascular
disease while 4 of 8 of those patients who had duration of having cardiovascular disease less than 5 years
died during study and rest of them had duration of having cardiovascular disease more than 6 years with
95% Cl 1.29-4.43, P = 0.006. In a HD center in Penang, Malaysia, 28 hemodialysed patients had
cardiovascular disease and only 4 of them died during the study and all of them had duration of having
cardiovascular disease more than 6 years with 95% Cl 0.64-6.34, P = 0.23. In this study, only duration of
having cardiovascular disease showed significant relationship with probability of dying among
hemodialysed patients in Jakarta, Indonesia.
1 INTRODUCTION
According to the World Health Organization (2005),
approximately 35 million people died due to chronic
kidney disease (Levey et al., 2007). The prevalence
of End Stage Renal Disease (ESRD) in the world
were more than 2 million people (Ortiz et al., 2014).
An adjusted 5-year survival of all patients with
ESRD (treated with dialysis or transplantation) was
41% in the USA, 48% in Europe and 60% in Japan
for patients with ESRD onset between 2004 and
2008 (Robinson et al., 2016).
Risk factor is an alarm pointing to worst
condition that may happen for CKD patients. In this
case, information about risk factors on CKD is very
important for others to avoid severity of ESRD.
People who are not aware of the risk factors, signs
and symptoms of CKD may be a victim of ESRD
patients in future.
There are four categories of risk factors of end
stage renal disease. They are susceptibility,
initiation, progression and end-stage factors.
Susceptibility factors depend on sociodemographic
variables such as age, family history and race.
Initiation factors depend on the disease such as
metabolic disorder, infection, autoimmune and drug
toxicity, while, progression factors depend on the
severity of the metabolic disorder such as the higher
blood pressure, higher proteinuria and poor
glycemic control and End-stage factors depend on
lack of attention to the progression factors such as
lower dialysis dose and high serum phosphorus
(Levey, A.S., Eckardt, K., Tsukamoto, Y., Levin, A.,
Coresh, J., Rossert, J., de Zeeuw, D., Hostetter, T.,
Lameire, N., Eknoyan et al., 2005).
2 MATERIAL AND METHODS
Research was carried out in hemodialysis (HD) ward
Jakarta, Indonesia and Pulau Pinang, Malaysia.
Universal sampling were used to select 178 and 78
patients who had been followed for 9 months in
Hemodialysis Center Jakarta and Penang,
respectively. A cohort prospective study was
conducted in this research.
84
Ramatillah, D., Sulaiman, S., Khan, A. and Husna, I.
Potential Risk Factors of End Stage Renal Disease in Patients of Hemodialysis.
DOI: 10.5220/0008239800840089
In Proceedings of the 1st Muhammadiyah International Conference on Health and Pharmaceutical Development (MICH-PhD 2018), pages 84-89
ISBN: 978-989-758-349-0
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
Before requesting for the ethical approval,
researcher had a good clinical practice certificate.
Ethical clearance were sourced from ethical medical
committee from Faculty of Medicine in Indonesia
(728/UN2.F1/ETIK/2015) and Clinical Research
Center Pulau Pinang Hospital Malaysia
((5)KKM/NIHSEC/P16-133). The approval letters
were given before starting data collection.
The collection of data also started after
determining the inclusion criteria and patients also
signed the agreement. The study included diabetic
and / hypertensive patients who undergone
hemodialysis and have aged more than 18 years old.
Patients who have cancer, HIV/AIDS, Systemic
Lupus Erythema and pregnant were excluded in this
study. All the data were transferred to the clinical
data collection form.
3 RESULTS
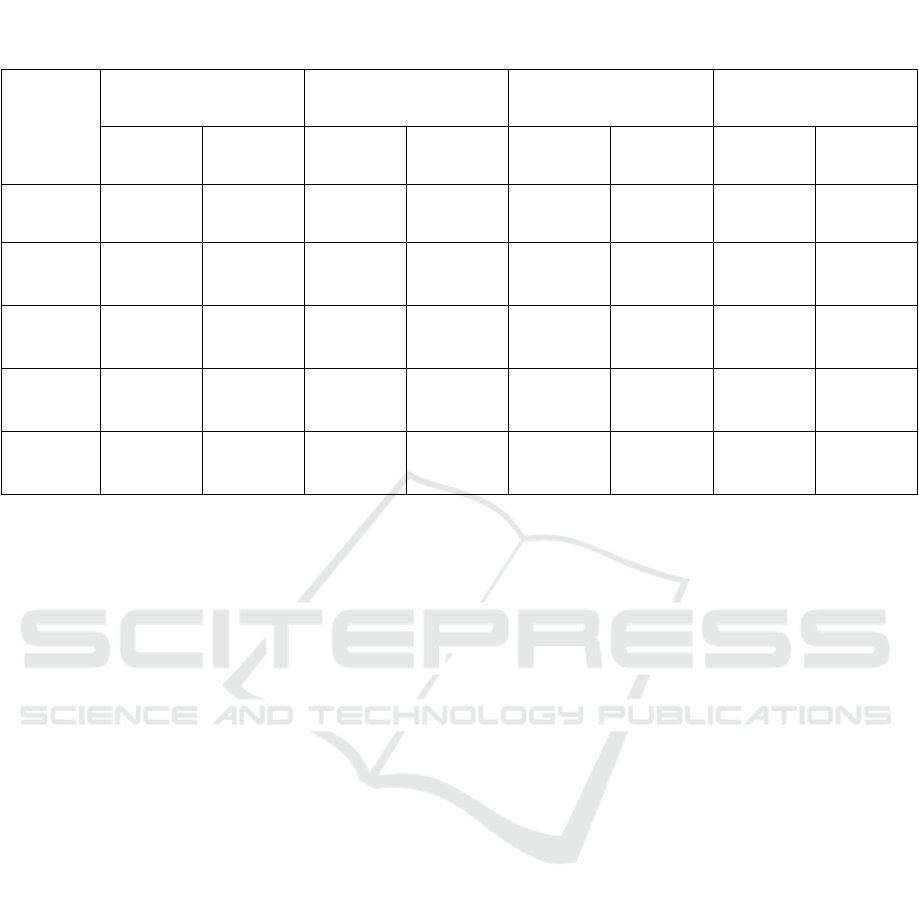
Table 1. shows correlation between potential risk
factors of ESRD and probability of dying in both
HD centers. Probability of dying can be measured
by these potential risk factors in this study, but only
duration of cardiovascular disease showed
significant relationship with probability of dying in
HD center Jakarta, Indonesia as shown in Table 1.
Cause of ESRD increased risk of death almost 2
times among hemodialysed patients in a HD center
in Jakarta, Indonesia and it also increased risk of
death more than 7 times among hemodialysed
patients in a HD center in Penang, Malaysia anytime
during 9 months followed up and P value for both
indicated no statistical difference as shown in Table
1.
Duration of having cardiovascular disease
elevated risk of death more than 2 times in both HD
center in Jakarta, Indonesia and Penang, Malaysia
anytime during the 9 months followed up but only
patients of hemodialysis in Jakarta, Indonesia who
showed significant relationship.
3.1 Cause of ESRD
Cause of ESRD is one of the potential risk factors
which can influence duration of hemodialysis among
hemodialysed patients (Disease and Kidney Disease:
Improving Global Outcomes (KDIGO) Anemia
Work Group, 2012). Table 3 shows correlation
between potential risk factors of ESRD and
frequency of HD from first time on HD in both HD
center Jakarta, Indonesia and Penang, Malaysia.
Significant correlation was found among
hemodialysed patients in Penang, Malaysia. It can
be seen from median value for each group, while the
significant difference of duration of hemodialysis for
each group based on cause of ESRD was shown.
Hemodialysed patients who had hypertension had
the highest median (1062) value compared with
hemodialysed patients who had diabetic mellitus and
DM & HT in a HD center Penang, Malaysia as
shown in Table 2.
Table 1: Potential Risk Factors of ESRD and Probability of Dying Among Hypertensive/Diabetic Patients Who Undergone
Hemodialysis (Prospective Sample / 9 Months Followed up)
Potential
Risk
Factors
B
Exp (B)
Hazard Ratio
95% Cl For Exp (B) P * Value
Jakarta,
Indonesia
Penang,
Malaysia
Jakarta,
Indonesia
Penang,
Malaysia
Jakarta,
Indonesia
Penang,
Malaysia
Jakarta,
Indonesia
Penang,
Malaysia
Cause of
ESRD
0.49 2.02 1.64 7.53 0.75-3.58 0.66-85.58 0.22 0.10
Duration
of having
CKD
-3.24 -1.23 0.04 0.29 0.001-1.85 0.06-1.37 0.10 0.12
Duration
of having
CVD
0.87 0.70 2.39 2.01 1.29-4.43 0.64-6.34 0.006* 0.23
Duration
of having
HT
-0.24 -0.67 0.79 0.51 0.45-1.39 0.16-1.63 0.41 0.26
Duration
of having
DM
-0.38 0.43 0.69 1.53 0.43-1.11 0.89-2.64 0.12 0.13
Potential Risk Factors of End Stage Renal Disease in Patients of Hemodialysis
85
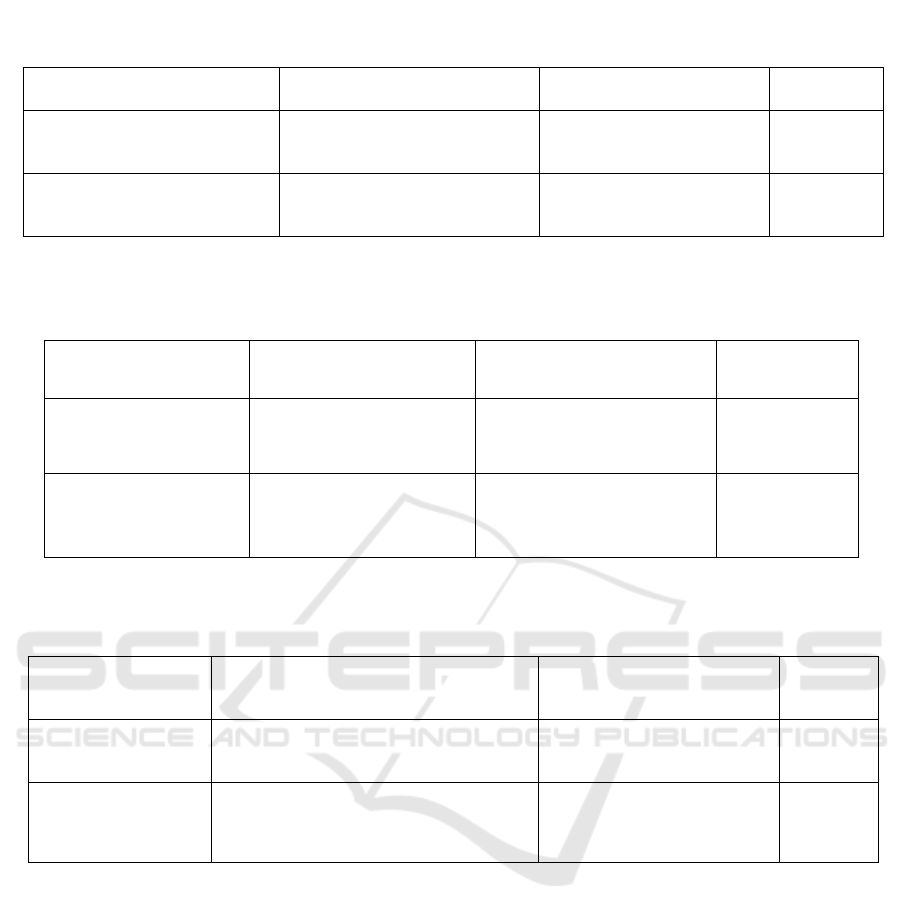
3.2 Duration of having CKD
Duration of ESRD may affect the duration of
hemodialysis among hemodialysed patients (Disease
and Kidney Disease: Improving Global Outcomes
(KDIGO) Anemia Work Group, 2012). Table 3.
shows correlation between duration of having CKD
and frequency of HD from first time on HD in both
HD centers Jakarta, Indonesia and Penang,
Malaysia.
Significant correlation between duration of
having CKD and frequency of HD from first time on
HD were found among hemodialysed patients in
both HD centers as shown in Table 3. In Indonesia,
the highest median value (1137 times) of frequency
of HD from first time on HD was shown by the third
group (≥ 11-15 years) of duration of having CKD.
However, in Malaysia, median value of 2566 times
was shown by fourth group (≥ 16-20 years) of
duration of having CKD.
Table 2. Cause of ESRD and Frequency of HD from first time on HD
N for each group of cause of
ESRD
Median for each group
(
Times of HD Fre
q
uenc
y)
P*
Frequency of HD from first
time on HD (Indonesia)
DM (33)
HT (98)
DM & HT
(
47
)
127
135
146
0.36
Frequency of HD from first
time on HD (Malaysia)
DM (5)
HT (43)
DM & HT (30)
238
1062
624.5
0.001*
* A Kruskal-Wallis Tests
Table 3.Duration of having CKD and Frequency of HD from first time on HD Among Diabetic/Hypertensive Patients
Who Undergone Hemodialysis
Component
Years (N) Duration of
having CKD
Median for each group
(Times of HD Frequency)
P*
Frequency of HD from
first time on HD
(Indonesia)
≤ 5 years (153)
≥ 6-10 years (20)
≥ 11-15 years (5)
127
598
1137
< 0.001*
Frequency of HD from
first time on HD
(Malaysia)
≤ 5 years (36)
≥ 6-10 years (24)
≥ 11-15 years (9)
≥ 16-20 years (9)
291
1008
1821
2566
< 0.001*
* A Kruskal-Wallis Test
Table 4. Duration of Having Cardiovascular Disease and Frequency of HD Since First HD Among Diabetic/Hypertensive
Patients Who Undergone Hemodialysis
Component N for each group of duration of having
cardiovascular disease
Years (N)
Median for each group
(Times of HD Frequency)
P*
Frequency of HD
Since First HD
(
Indonesia
)
≤ 5 years (41)
≥ 6 years (6)
127
280.5
0.21
Frequency of HD
Since First HD
(Malaysia)
≤ 5 years (12)
≥ 6 years (20)
659
1530
0.005*
* A Kruskal-Wallis Test
MICH-PhD 2018 - 1st Muhammadiyah International Conference on Health and Pharmaceutical Development
86
3.3 Duration of Having Cardiovascular
Disease
Duration of having cardiovascular disease may
influence the duration of hemodialysis among
hemodialysed patients (Ortiz et al., 2014). Table 5.
shows correlation between duration of having
cardiovascular disease and frequency of HD from
first time on HD in both HD center Jakarta,
Indonesia and Penang, Malaysia.
Significant correlation (p 0.005) between
duration of having cardiovascular disease and
frequency of HD from first time on HD was found
among hemodialysed patients in a HD center
Penang, Malaysia as shown in Table 4.
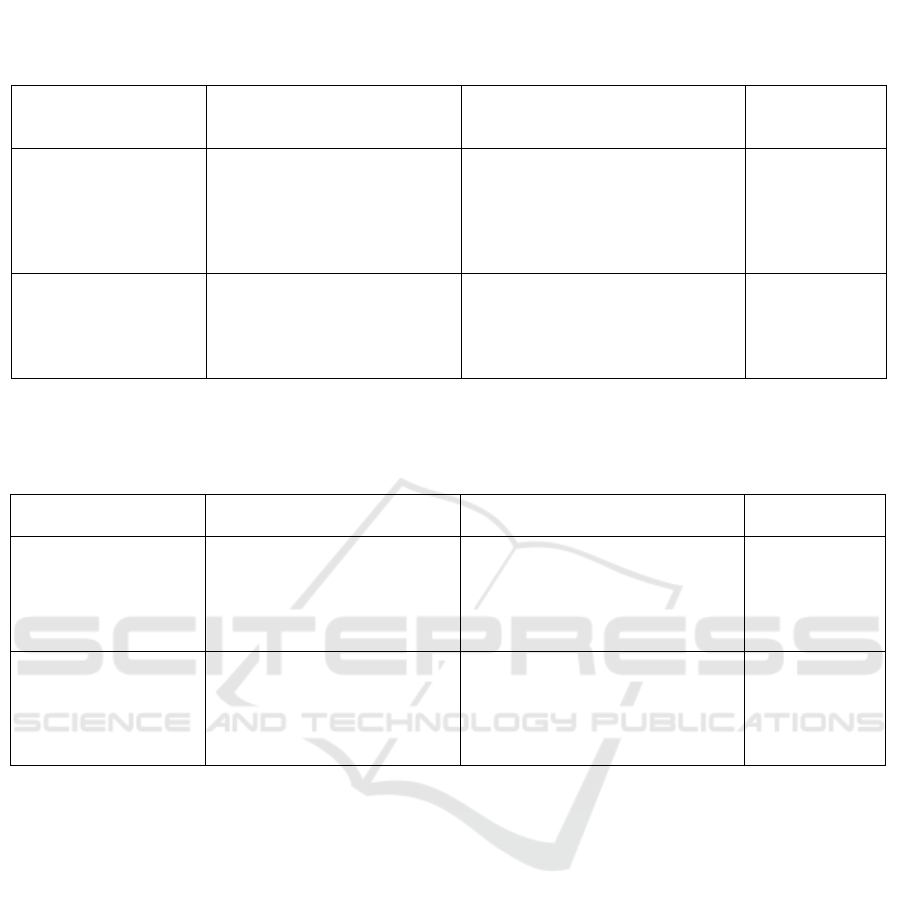
Duration of having hypertension and frequency
of HD since first HD were found significant among
hemodialysed patients in both HD centers of
Malaysia (P <0.001) and Indonesia (P <0.001) as
shown in Table 5. In Indonesia, the highest median
value of frequency (447.5 times) of HD from first
time on HD was shown by the third group (≥11-15
years) of duration of hypertensive patients.
However, in Malaysia, patients with ≥ 16-20 years
duration showed frequency of 1665 times in
hypertensive patients.
3.4 Duration of Having Diabetes
Mellitus
Duration of having diabetes Mellitus may affect the
duration of hemodialysis among hemodialysed
patients. Table 6 shows correlation between duration
of having diabetes mellitus and frequency of HD
from first time on HD in both HD center Jakarta,
Indonesia and Penang, Malaysia.
Significant correlation between duration of
having diabetes mellitus and frequency of HD since
first HD was found among hemodialysed patients in
a HD center Penang, Malaysia as shown in Table 6.
Table 5. Duration of Having Hypertension and Frequency of HD Since First HD Among Diabetic/Hypertensive Patients
Who Undergone Hemodialysis
Component N for each group
Years (N) of duration of having
h
yp
ertension
Median for each group (Times of
HD Frequency)
P*
Frequency of HD Since
First HD (Indonesia)
≤ 5 years (117)
≥ 6-10 years (34)
≥ 11-15 years (14)
≥ 16-20 years (6)
≥ 21 years (7)
125
401.5
447.5
225
197
<0.001*
Frequency of HD Since
First HD (Malaysia)
≤ 5 years (6)
≥ 6-10 years (26)
≥ 11-15 years (20)
≥ 16-20 years (13)
≥ 21
y
ears
(
13
)
208.5
636.5
966.5
1665
1542
<0.001*
*Kruskal Wallis Test
Table 6. Duration of Having Diabetes Mellitus and Frequency of HD Since First HD Among Diabetic/Hypertensive
Patients Who Undergone Hemodialysis
Component N for each group of duration of
having diabetes mellitus
Median for each group (times of
HD Frequency)
P*
Frequency of HD Since
First HD (Indonesia)
≤ 5 years (26)
≥ 6-10 years (22)
≥ 11-15 years (17)
≥ 16-20 years (8)
≥ 21 years (9)
135
126
172
228.5
141
0.74
Frequency of HD Since
First HD (Malaysia)
≤ 5 years (5)
≥ 6-10 years (8)
≥ 11-15 years(11)
≥ 16-20 years (5)
≥ 21 years (6)
240
475
802
565
888.5
0.01*
* A Kruskal-Wallis Tests
Potential Risk Factors of End Stage Renal Disease in Patients of Hemodialysis
87

4 DISCUSSION
In Penang, Malaysia, all these five potential risk
factors (cause of ESRD, duration of having CKD,
duration of having cardiovascular disease, duration
of having hypertension and duration of having
diabetic mellitus) showed significant correlation
with frequency of HD from first treatment.
Meanwhile, only two potential risk factors showed
significant relationship in HD center Jakarta,
Indonesia including duration of having CKD and
duration of having hypertension.
Duration of having CKD was dependent on
frequency of hemodialysis since first treatment.
Duration of having CKD was calculated by how
many session (frequency) of hemodialysis, which
had been done by those patients. It is the same with
duration of cardiovascular, hypertensive and diabetic
among those patients. Length of duration these
diseases will be equal to frequency of hemodialysis
because those diseases can not be excluded
permanently.. Agarwal, 2005 reported that the use of
antihypertensive drugs treatment improve survival
(Agarwal, 2005).
In this finding, frequency of hemodialysis among
diabetic and / hypertensive patients influenced
duration of having CKD and duration of having
hypertension in both HD centers. Some studies
identified that increasing dialysis time and frequency
affect hypertensive condition (Fagugli et al., 2001,
2006; Culleton et al., 2007).
Many factors contributed length of hemodialysis
session, some of them are good medication and less
of complication. Chandrashekar et.al., 2014 reported
that there is no significant difference in terms of
survival among diabetics compared with non-
diabetics (Chandrashekar, Ramakrishnan and
Rangarajan, 2014). Another study revealed that the
survival of patients on hemodialysis with diabetes
mellitus was lower than those patients without
diabetes mellitus (Ghaderian et al., 2015).
In Australia, New Zealand and the United States,
Cardiovascular Disease (CVD) was reported as the
leading cause of death in dialysis patients (Annual
Data Report Minnepolis, 2006; McDonald, 2015).
Another study, Mailloux et al., 1991 identified the
causes of death in maintenance dialysis patients who
survived at least 90 days and were monitored during
a 16 year period and cardiovascular disease was one
of the causes of death among those patients
(Mailloux et al., 1991).
Cardiovascular disease is one of the
complications of end-stage renal failure (Marry
Anne and Alledredge, 2013). The statement about
correlation of CV in presence of CKD is still a
controversy (Herzog et al., 2011). In this study,
duration of cardiovascular disease influenced the
probability of dying / risk of mortality among
hemodialysed patients in a HD center Jakarta,
Indonesia.
5 CONCLUSION
Five potential risk factors of ESRD were found in
this study: cause of ESRD, duration of having CKD,
duration of having cardiovascular disease, duration
of having hypertension and duration of having
diabetes mellitus. Only duration of having
cardiovascular disease showed significant
relationship with probability of dying but only in
HD patients in Jakarta, Indonesia; whereas duration
of having cardiovascular disease elevated risk of
death more than 2 times in both HD centers in
Jakarta, Indonesia and Penang, Malaysia.
6 DISCLOSURE OF POTENTIAL
CONFLICTS OF INTEREST
AND ACKNOWLEDGEMENT
The authors declared that we have no conflict of
interest.
REFERENCES
Agarwal, R. 2005 ‘Hypertension and survival in
chronic hemodialysis patients - Past lessons and
future opportunities’, Kidney International,
67(1), pp. 1–13.
Annual Data Report Minnepolis. 2006. Renal Data
System U.S.
Chandrashekar, A., Ramakrishnan, S. and
Rangarajan, D. 2014. ‘Survival Analysis of
Patients on Maintenance Hemodialysis’, Indian
Journal of Nephrology, 24(4), pp. 206–13.
Culleton, BF, Walsh, M, Klarenbach, SW, Mortis,
G, Scott-Douglas , N, Quinn, RR, Tonelli, M,
Donnelly, S, Friedrich, MG, Kumar, A,
Mahallati, H, Hemmelgarn, BR, Manns, BJ..
2007. ‘Effect of Frequent Nocturnal
Hemodialysis Versus Conventional
Hemodialysis on Left Ventricular Mass and
Quality of Life: A Randomized Controlled
Trial’, Jama, 298, pp. 1291–1299.
MICH-PhD 2018 - 1st Muhammadiyah International Conference on Health and Pharmaceutical Development
88

Disease, K. C. P. G. for A. in C. K. and Kidney
Disease: Improving Global Outcomes (KDIGO)
Anemia Work Group. 2012. ‘KDIGO Clinical
Practice Guideline for Anemia in Chronic
Kidney Disease’, Kidney International
supplement, 2(4), pp. 279–335. doi:
10.1038/kisup.2012.40.
Fagugli, RM, Reboldi, G, Quintaliani, G, Pasini, P,
Ciao, G, Cicconi, B, Pasticci, F, Kaufman, JM,
Buoncristiani, U. 2001.‘Short Daily
Hemodialysis : Blood Pressure Control and Left
Ventricular Mass Reduction in Hypertensive
Hemodialysis Patients’, Am J Kidney Dis, 38, pp.
371–376.
Fagugli, RM, Pasini, P, Pasticci, F, Ciao, G,
Cicconi, B, Buoncristiani, U. 2006.‘Effects of
Short Daily Hemodialysis and Extended
Standard Hemodialysis on Blood Pressure and
Cardiac Hypertrophy : A Comparative Study’,
Nephrology, 19, pp. 77–83.
Ghaderian, SB,
Hayati, F,
Shayanpour, S,
Beladi
Mousavi, SS. 2015. ‘Diabetes and end-stage
renal disease ; a review article on new concepts’,
Journal of Renal Injury Prevention, 4(2), pp. 28–
33.
Herzog, CA, Asinger, RW, Berger, AK, Charytan,
DM, Díez, J, Hart, RG, Eckardt, KU, Kasiske,
BL, McCullough, PA, Passman, RS, DeLoach,
SS, Pun, PH, Ritz, E. 2011. ‘Cardiovascular
disease in chronic kidney disease. A clinical
update from Kidney Disease: Improving Global
Outcomes (KDIGO)’, Kidney International,
80(6), pp. 572–586.
Levey, A.S., Eckardt, K., Tsukamoto, Y., Levin, A.,
Coresh, J., Rossert, J., de Zeeuw, D., Hostetter,
T., Lameire, N., Eknoyan, G. 2005. ‘Definition
and classification of chronic kidney disease: A
position statement from Kidney Disease:
Improving Global Outcomes (KDIGO)’, Kidney
International, 67(6), pp. 2089–2100.
Levey, AS, Atkins, R, Coresh, J, Cohen, EP,
Collins, AJ, Eckardt, KU, Nahas, ME, Jaber, BL,
Jadoul, M, Levin, A, Powe, NR, Rossert, J,
Wheeler, DC, Lameire, N, Eknoyan, G. 2007.
‘Chronic kidney disease as a global public health
problem: Approaches and initiatives – a position
statement from Kidney Disease Improving
Global Outcomes’, Kidney International.
Elsevier Masson SAS, 72(3), pp. 247–259.
Mailloux, LU, Bellucci, AG, Wilkes, BM,
Napolitano, B, Mossey, RT, Lesser, M,
Bluestone, PA. 1991. ‘Mortality in Dialysis
Patients : Analysis of the Causes of Death’, Am J
Kidney Dis, 18(3), pp. 326–335.
Marry Anne, K.-K. and Alledredge, B. K. 2013.
Koda-Kimble and Young’s Applied
Therapeutics: The Clinical Use of Drugs.
McDonald, S. P. 2015. ‘Australia and New Zealand
Dialysis and Transplant Registry.’, Kidney
international supplements, 5(1), pp. 39–44.
Ortiz, A, Covic, A, Fliser, D, Fouque, D, Goldsmith,
D, Kanbay, M, Mallamaci, F, Massy, ZA,
Rossignol, P, Vanholder, R, Wiecek, A, Zoccali,
C, London, GM; Board of the EURECA-m
Working Group of ERA-EDTA.
2014.‘Epidemiology, contributors to, and clinical
trials of mortality risk in chronic kidney failure’,
The Lancet, 383(9931), pp. 1831–1843.
Robinson, BM, Akizawa, T, Jager, KJ, Kerr, PG,
Saran, R, Pisoni, RL.2016. ‘Factors affecting
outcomes in patients reaching end-stage kidney
disease worldwide: differences in access to renal
replacement therapy, modality use, and
haemodialysis practices’, The Lancet,
388(10041), pp. 294–306.
Potential Risk Factors of End Stage Renal Disease in Patients of Hemodialysis
89
