
Yaws: Neglected and Abandoned?
Time to Re-Emerged
Erda Avriyanti, Pati Aji Achdiat
Department of Dermatology and Venereology, Faculty of Medicine,
Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Bandung 40161, Indonesia
Keywords: epidemiology, South East Asia, Treponema pallidum subspecies pertenue, yaws
Abstract: Yaws, a disease caused by Treponema pallidum subspecies pertenue infection, is a neglected tropical
disease. Until now, yaws is still one of the public health problems in South East Asia, even though it had
been forgotten before. But, recently it has re-emerged once again. Yaws becomes the aim of the mass-
treatment eradication of World Health Organization (WHO) by 2020 through the mass-treatment program.
The main target of the success of this campaign is a good knowledge of the disease epidemiology. We
undertook a review of the historical trends and new information from endemic countries, with a point of
view to assessing the state of knowledge about yaws. The plague of yaws now exists in Africa, Asia, and the
South Pacific. About 12 countries establish as endemic countries, one of them is Indonesia that located in
South East Asia region. Between 2008 and 2012 more than 300,000 new cases into the WHO. Based on
Ministry of Health Regulation Republic of Indonesia No. 8 in 2017 on eradication of yaws, it is necessary to
administer continuous, effective, and efficient program. Several dilemmas of yaws are low levels of
reporting, potential misdiagnosis, and limited documentation on the prevalence of asymptomatic infections.
The current data is likely to underestimate the agonize of the disease. Thereupon, more effort is needed to
improve the current interactive data, that is likely to have positive vibes on yaws eradication plan.
1 INTRODUCTION
Yaws or also called framboesia, pian, buba, paru,
parangi,(Perine et al., 1984; Marks et al., 2015) or
patek (GREEN and HARMAN, 1986) is an
infectious disease caused by Treponema pallidum
subspecies pertenue (T. pallidum subsp. pertenue),
also have a close taxonomy with Treponema
pallidum subspecies pallidum (T. pallidum subsp.
pallidum), as syphilis causes.(Marrouche et al.,
2012) The yaws term was first introduced by the
Dutch physician Willem Piso in the seventeenth
century to describe the clinical picture of the disease
in South America from the term ulcers which in
Carib are yaya.(Piso and Marcgrave, 1648) Its
clinical picture resembling raspberries, so it is also
known as yaws derived from the French "framboise"
which means raspberry.(Marks et al., 2015)
The clinical features of yaws are divided into
several stages, namely primary, secondary, latent,
and tertiary stages. The available serological tests
cannot distinguish between yaws and syphilis.
Though yaws has different characteristics with
syphilis, such as in the form of basic ulcers of dirty
lesions, the size could reach 5 cm, pain, and itching,
and have a predilection in lower limbs. If left
untreated, the lesion may become chronic and
destructive,(Marks et al., 2015) causing potentially
disability, pain, and social problems in the
patient.(Marrouche et al., 2012) Other things that
distinguish yaws with syphilis include geographic
distribution, patient’s age characteristics, non-
venereal type of transmission, that is transmitted
through skin contact rather than sexual contact, and
the clinical picture of the disease.(Mitja et al., 2013;
Marks et al., 2015)
Yaws generally attacks children who live in the
tropical area.(Marrouche et al., 2012; Marks et al.,
2015) This disease is still a public health problem in
Indonesia as a tropical country in terms of
eradication of yaws. The World Health Organization
(WHO) aims to eradicate yaws by 2020, which
consists of an initial mass treatment of endemic
communities followed by surveys every 6 months to
actively detect and treat remaining cases and their
contacts.(Marks et al., 2015) The changed of use of
a single oral dose of azithromycin from benzathine
penicillin injection has made mass treatment more
Avriyanti, E. and Achdiat, P.
Yaws: Neglected and Abandoned? Time to Re-emerged.
DOI: 10.5220/0008154902450248
In Proceedings of the 23rd Regional Conference of Dermatology (RCD 2018), pages 245-248
ISBN: 978-989-758-494-7
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reser ved
245

feasible and is currently recommended in areas
where yaws is prevalent. Due to benzathine
penicillin injection therapy has several
disadvantages such as causing pain in the patient,
difficulties of drug storage process, and limited
supply so that oral azithromycin is preferred.
Indonesia is the only country in Southeast Asia to
report cases of yaws in WHO report year
2012.(International Symposium on Yaws and Other
Endemic Treponematoses, 1985) Based on Ministry
of Health Regulation Republic of Indonesia No. 8 in
2017 on eradication of yaws, it is necessary to
administer the continuous, effective, and efficient
program.(The Ministry of Health Republic of
Indonesia, 2017) One of the key determinants of the
success of the eradication campaign is a good
understanding of the disease epidemiology,
particularly its geographic distribution and risk
factors. Based on the description above, this review
hopefully could be an insight of accurate of yaws
specifically in Indonesia region.
2 THE ORIGIN OF YAWS
Yaws has been known since the early 16th century
that happened to slaves in Spain. In the 17th century,
the disease was reportedly suffered by slaves in
North America. In the early 1950s, an estimated 50-
150 million people worldwide experienced yaws.
(World Health Organization, 2013) Approximately
75% of patients are children aged less than 15 years
(peak incidence occurs in children aged 6-10 years).
Men and women have the same opportunities for
this disease. (World Health Organization, 2006)
At least 90 countries have reported endemic
yaws,(Hackett, 1989; World Health Organization,
2013.) especially in Africa with an incidence rate of
over 10,000 cases per year, and the highest
incidence is reported in four countries: Ivory Coast,
Ghana, Cameroon and the Congo reaches more than
100,000 cases per year.(Hackett, 1989) In Asia,
however, yaws was reported in areas of India, China,
Thailand, Cambodia, Laos, Malaysia, and
Indonesia.(Kazadi et al., 2014)
In the mid-1950s and early 1960s, WHO
undertook a worldwide mass treatment of yaws
around the world with benzathine penicillin injection
treatment that dramatically decreased the prevalence
of the disease.(Mitja et al., 2013) Since 1990,
reporting to WHO was not mandatory because it did
not become endemic anymore in many countries, so,
epidemiological data becomes very limited. But,
based on the WHO report up to 2013, 12 countries
were reportedly endemic, consisting of 8
countries in Africa namely Benin, Cameroon,
Central African Republic, Ivory Coast, Republic of
Congo, Democratic Republic of Congo, Ghana, and
Togo; three countries in the Western Pacific region
namely Vanuatu, Papua New Guinea, and the
Solomon Islands; and one country from the
Southeast Asian region, Indonesia (Figure 1). (Mitja
et al., 2013; Kazadi et al., 2014)
Figure 1. Worldwide distribution of yaws in 2012.(Kazadi
et al., 2014)
In 1950, according to WHO, cases of yaws in
Indonesia occurred in Aceh, Jambi, Bengkulu, South
Sumatra, East Java, and most of Eastern Indonesia
covering Nusa Tenggara, Sulawesi, Maluku and
Papua.(World Health Organization, 2006) The
decrease of yaws cases prevalence in Indonesia was
significantly reported in 1995, from 2,210 per
10,000 population in 1985 to less than 1 case per
10,000 population in 1995. In the report, it was
found that the number of cases in Java and Sumatera
in 1995 was less than 0.1 cases per 100,000
residents; while in East Indonesia, Papua, Maluku,
East Nusa Tenggara, and Sulawesi, the number of
cases of yaws was still more than 1 case per 100,000
population.(General Directory of Disease Control
and Health Environmental, 2005) In 2004, there
were 4,015 cases of yaws in Indonesia. While in the
period of 2008, there was an increment of yaws
cases became 5,926 cases in Indonesia, with the
highest prevalence in East Nusa Tenggara, Maluku,
and Papua. Figure 2 shows the spread of yaws cases
especially in Indonesia, that prominently found in
the province of East Nusa Tenggara. During the
period 2010-2013, reported cases of yaws as many
as 13,084 cases.(Mitjà et al., 2015)
RCD 2018 - The 23rd Regional Conference of Dermatology 2018
246
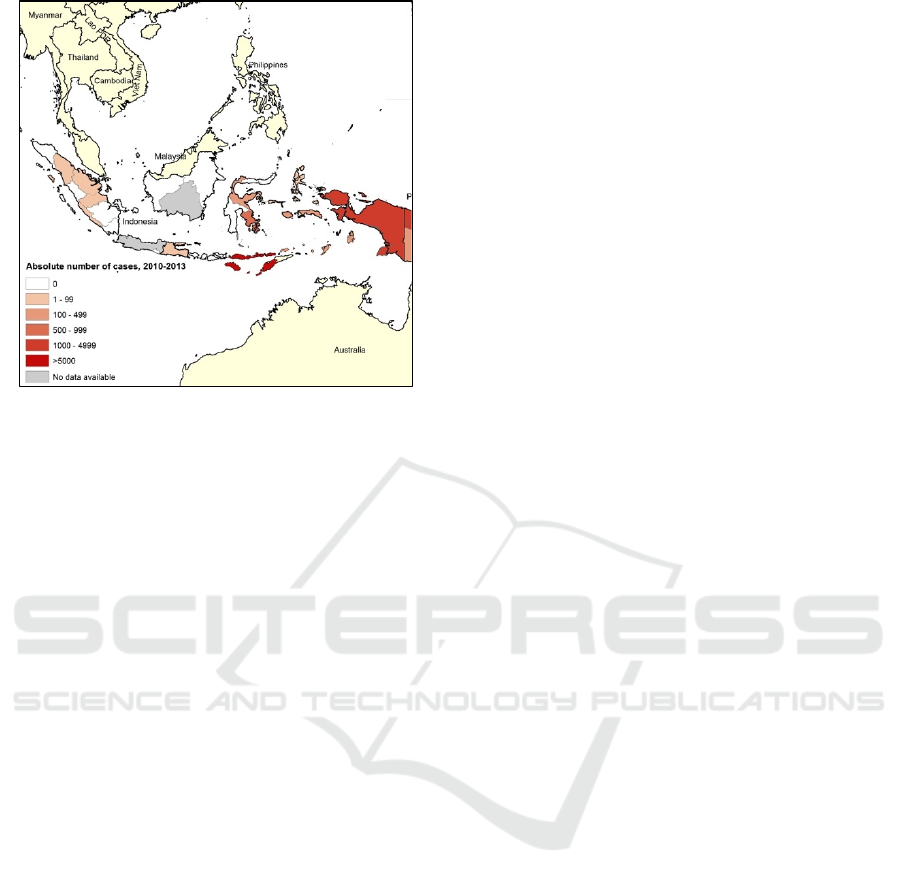
Figure 2. The distribution of yaws in South East Asia in
period of 2010-2013.14
3 NEW SPIRITS FOR
ERADICATION
In 2014, there were 1,521 cases of yaws reported in
Indonesia, particularly in Banten, East Nusa
Tenggara, Southeast Sulawesi, Maluku, Papua, and
West Papua provinces.(The Ministry of Health
Republic of Indonesia, 2017) The 2012 serological
survey results in several districts/municipalities
indicated that the prevalence of yaws ranged from
20-120 per 100,000 population aged 1-15 years.
Some areas with a history of endemic of yaws, such
as Aceh, Jambi, and South Sumatra provinces, did
not report any presence of yaws, but it could not
ascertain those regions as free area of yaws.(The
Ministry of Health Republic of Indonesia, 2017)
Indonesia has point of target for yaws eradication by
2017 (following global target) using active and
passive case detection and prompt treatment; some
of the major problems faced by the program include
the difficulty of reaching endemic communities scat-
tered over many small islands.
Indonesia has a combined yaws and leprosy
programme which functions under the Sub-
Directorate of Leprosy and Yaws. This allows for
the use of common resources to detect and manage
both diseases at national, provincial and district
levels.
Recently, in the early year of 2017, several
regions in Indonesia have been visited by WHO
team to assess eradication efforts and review the
implementation of the national elimination plan.
After achieving interruption of transmission of yaws,
a country needs to report zero yaws cases for three
consecutive years and provide serological evidence
to support the interruption of transmission in
children aged 1-5 years in order to request yaws-free
status by WHO. Indonesia and East Timor are the
only two remaining yaws-endemic countries in
WHO’s South-East Asia region.World Health
Organization, 2006 Furthermore, in West Java,
Indonesia, yaws patients were detected in Baduy
village people, the disease itself are prone to the
communities live there, since the people still have
culture and habit of not aware of the hygiene of the
environment. Thus, seeing those phenomena, the
eradication program of yaws should have more
concern related with the prevention and
management.
4 CONCLUSIONS
The accurate data is likely to exclude
underestimation of the agonizing of the disease.
Therefore, more works are needed to improve the
current interactive data, that is likely to have better
on the impact on yaws eradication plan, to emerge
another point of view of yaws. Then, yaws should
not be forgotten, because of this disease still around
us.
REFERENCES
General Directory of Disease Control and Health
Environmental. 2005. Patek Manual of Infectious
Disease Eradication. Jakarta: The Ministry of Health
Republic of Indonesia. pp. 12-3 (in Bahasa Indonesia).
GREEN, C.A., HARMAN, R.R.M., 1986. Yaws truly–a
survey of patients indexed under “Yaws” and a review
of the clinical and laboratory problems of diagnosis.
Clinical and Experimental Dermatology 11, 41–48.
Hackett, C.J., 1989. Endemic Treponematoses. In:
Manson PE, Bell DR, editor. Manson’s Tropical
Disease. 19
th
ed. London: Bailliere Tindal. pp. 623-45.
International Symposium on Yaws and Other Endemic
Treponematoses. 1985. Washington, DC, Apr 16–18,
1984. Rev Infect Dis. 7(Suppl. 2): S217-S351.
Kazadi, W.M., Asiedu, K.B., Agana, N., Mitjà, O., 2014.
Epidemiology of yaws: An update. Clinical
Epidemiology.
Marks, M., Lebari, D., Solomon, A.W., Higgins, S.P.,
2015. Yaws. International Journal of STD & AIDS 26,
696–703.
Marrouche, N., Ghosn, S.H., 2012. Endemic (nonvenereal)
treponematoses. In: Wolff, K., Goldsmith, L.A., Katz,
S.I., Gilchrest, BA., Paller, A.S., Leffell, D.J., editor.
Yaws: Neglected and Abandoned? Time to Re-emerged
247

Fitzpatrick’s Dermatology in general medicine. 8
th
ed.
New York: McGraw-Hill. pp. 2493.
Mitja, O., Asiedu, K., Mabey, D., 2013. Yaws. Lancet
(London, England) 381, 763–773.
Mitjà, O., Marks, M., Konan, D.J.P., Ayelo, G., Gonzalez-
Beiras, C., Boua, B., Houinei, W., Kobara, Y., Tabah,
E.N., Nsiire, A., Obvala, D., Taleo, F., Djupuri, R.,
Zaixing, Z., Utzinger, J., Vestergaard, L.S., Bassat, Q.,
Asiedu, K., 2015. Global epidemiology of yaws: A
systematic review. The Lancet Global Health 3, e324–
e331.
Perine, P.L., Hopkins, D.R., Niemel, P.L., St John, R.,
Causse, G., Antal, G.M., 1984. World Health
Organization. Handbook of endemic treponematoses:
yaws, endemic syphilis and pinta. World Health
Organization.
Piso, W., Marcgrave, G. 1648. Historia naturalis
Brasiliae. Amsterdam: Elsevier. pp. 35–8 (in Latin).
The Ministry of Health Republic of Indonesia. 2017. Rules
of Ministry of Health Number 8 Year 2017, Yaws
Eradication. Jakarta: The Ministry of Health Republic
of Indonesia. (in Bahasa Indonesia).
World Health Organization. 2013. Global Health
Observatory Data Repository: yaws. Geneva: World
Health Organization.
(http://apps.who.int/gho/data/node.main.NTDYAWS)
(Accessed 20 November 2017).
World Health Organization. 2006. Yaws eradication in the
South-East Asia Region. India; WHO.
RCD 2018 - The 23rd Regional Conference of Dermatology 2018
248
