
Effect of Extrinsic Motivation on Adversity Quotient in Patients With
HIV & AIDS
Yulia Dewi Puspitawati¹, Misutarno², Nursalam³
¹Post Graduate Program, Universitas Airlangga, Airlangga 4-6 Street, Surabaya, Indonesia
²Department Infection Disease Intermediary Treatment Unit, Dr. Soetomo Hospital, Surabaya
³Faculty of Nursing, Universitas Airlangga, Mulyorejo Surabaya,Indonesia
Keywords: Extrinsic motivation, Adversity Quotient, HIV & AIDS patients.
Abstract: Patients with HIV & AIDS may have various types of psychological response, so it is a very difficult
situation for them. Difficulty can be measured with Adversity Quotient. So nurses are expected to give
extrinsic motivation to bring back the quality of life for patients with HIV & AIDS. The objective of this
study was to identify the presence of the effect of extrinsic motivation on Adversity Quotient in patients
with HIV & AIDS in the Infectious Disease Intermediary Treatment Unit, Dr Soetomo Hospital, Surabaya.
This study used a quasi-experimental design. The population was taken from ambulatory patients. Samples
were taken using purposive sampling, in which the patients involved were those who only met the inclusion
criteria, with the total sample of 16 individuals. The independent variable in this study was extrinsic
motivation, which was presenting as social support, and the dependent variable was Adversity Quotient.
Data were collected using questionnaires and interviews, and were subsequently analyzed using the
Wilcoxon Signed Rank Test and Mann-Whitney Test with a significance value of 0.05. Results revealed that
the Adversity Quotient of the patient indicated the effect of extrinsic motivation on Adversity Quotient of
patients with HIV & AIDS (p = 0.017). The extrinsic motivation was found to have an effect on control
response (p = 0.027) and origin response (p = 0.028), while there was no influence on ownership response
(p = 0.334), reach (p = 0.129), and endurance (p = 0.161). The extrinsic motivation with intervention of
social support has a positive effect on the improvement of Adversity Quotient in patients with HIV & AIDS.
The level of Adversity Quotient in these patients may have an effect on the attitude in dealing with the
recovery of their disease. Further study should measure the effectiveness of Adversity Quotient training on
acceptance response in patients with HIV & AIDS.
1 INTRODUCTION
Generally, AIDS patients are in a situation that
makes them feel that death is coming in the near
future and this situation they anticipate specifically.
When an individual is declared as HIV-infected,
they will show changes in psychosocial character
(living in stress, depression, lack of social support
and behavioural changes) (Nasronudin, 2005).
Psychological responses to psychological
adaptations depend on three important factors,
including biological factors (symptoms of the course
of the disease), psychological factors (personality
and problem-solving skills and interpersonal
support) and sociocultural factors (social stigma
attached to HIV infection) (Muma, 1997).
Psychological systems emphasize the effects of
psychodynamic factors, motivation and personality
on the experience of illness and reactions to illness
(Tandiono, 2007). Transpersonal psychotherapy
(including motivation) is an option for those who
feel near-death, isolation, or other psychological
problems so that they will experience harmony
internally and externally (Maramis, 2005). High
motivation can influence behavior through increased
knowledge and skills (Colquite, 2000 in Niniek,
2004). Individuals who have Adversity Quotient
(AQ) are highly emotionally and physically flexible
enough to face adversity (Stoltz, 1997). Adversity
Quotient (AQ) has three forms of definition. First,
AQ is a new conceptual framework for
understanding and improving all facets of success.
Second, AQ is a measure of knowing one's response
Dewi Puspitawati, Y., Misutarno, . and Nursalam, .
Effect of Extrinsic Motivation on Adversity Quotient in Patients With HIV AIDS.
DOI: 10.5220/0007541502850291
In Proceedings of the 2nd International Conference Postgraduate School (ICPS 2018), pages 285-291
ISBN: 978-989-758-348-3
Copyright
c
2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
285

to adversity. During this time, these unconscious
patterns are actually already owned by each
individual. Finally, AQ is a set of tools that have a
scientific basis for improving individual responses to
deal with adversity (Stoltz, 1997). According to
Stoltz (1997), AQ consists of five dimensions:
COORE which includes control, origin, ownership,
reach and endurance. However, the effect of
extrinsic motivation on Adversity Quotient on HIV
and AIDS patients is unclear.
The prevalence of depression in patients with
HIV & AIDS has doubled compared with the normal
population. In treated patients, this figure is higher
(about 40%). A longitudinal study found that CD4 +
lymphocyte count decreased 38% more in HIV
patients with depression than in the group of HIV
patients without depression. The prevalence of
depression increased from 15-27% in 36 months
before the diagnosis of AIDS to 34% at 6 months
before the diagnosis of AIDS and 43% at 6 months
after the diagnosis (Tandiono, 2007).
Motivation has a major influence in the life of a
person, whether extrinsic motivation, for example,
parents, friends support etc, as well as intrinsic
motivation, i.e. motivation that comes from within
the individual themself. In a state of deterioration
only self-motivation in themselves can help to
recover because humans have control over their
health and well-being. The role of supporters and
those around is merely a guide that helps restore
natural and emotional balance (Santrock, 2002).
Social support affects health and protects a person
against the negative effects of severe stress
(Nursalam, 2007). HIV & AIDS patients are directed
to develop themselves with the transformation of
awareness in order to manage their emotions
independently so they can perform activities like
healthy people to improve their quality of life. Based
on the phenomenon that psychological and
motivational conditions in people with HIV & AIDS
cause different psychological responses, and also
because the effect of extrinsic motivation on
Adversity Quotient on HIV & AIDS patients has not
yet been studied, this study was conducted to
identify the effect of extrinsic motivation on
Adversity Quotient in people with HIV & AIDS.
Extrinsic motivation in the form of social support is
needed by HIV & AIDS patients to accelerate the
acceptance of the disease.
2 MATERIALS AND METHODS
This study used a quasi-experimental design by
involving a control group in addition to the
experimental group, which was carried out in the
Infectious Disease Intermediate Treatment Unit, Dr.
Soetomo Hospital, Surabaya, from June to July
2008. Samples were HIV/AIDS-infected patients
treated in the Unit. The samples were chosen by
purposive sampling method with inclusion criteria
including HIV & AIDS patients receiving ARV
treatment, confirmed as positively infected for 1-2
years, more than 20 years old, willing to participate
in research and able to communicate and able to read
and write.
Data collection in this study used questionnaires
and interviews for primary data, while for secondary
data collection was done by using the patients'
medical records. Data obtained were processed and
analyzed using Wilcoxon Signed Rank-Test test to
determine the difference of pre-test and post-test on
the dependent variable of Adversity Quotient of HIV
& AIDS patients before and after intervention. The
use of the MannWhitney statistical test analyzed the
difference between Adversity Quotient between
groups with extrinsic motivation (social support) and
no extrinsic motivation. Statistical tests were
performed using the SPSS program.
3 RESULTS AND DISCUSSION
3.1 Level of Adversity Quotient of HIV &
AIDS Patients
The variables measured in this study were Adversity
Quotient of patients according to Stoltz. Results
questionnaires are presented in the table as follows:
ICPS 2018 - 2nd International Conference Postgraduate School
286
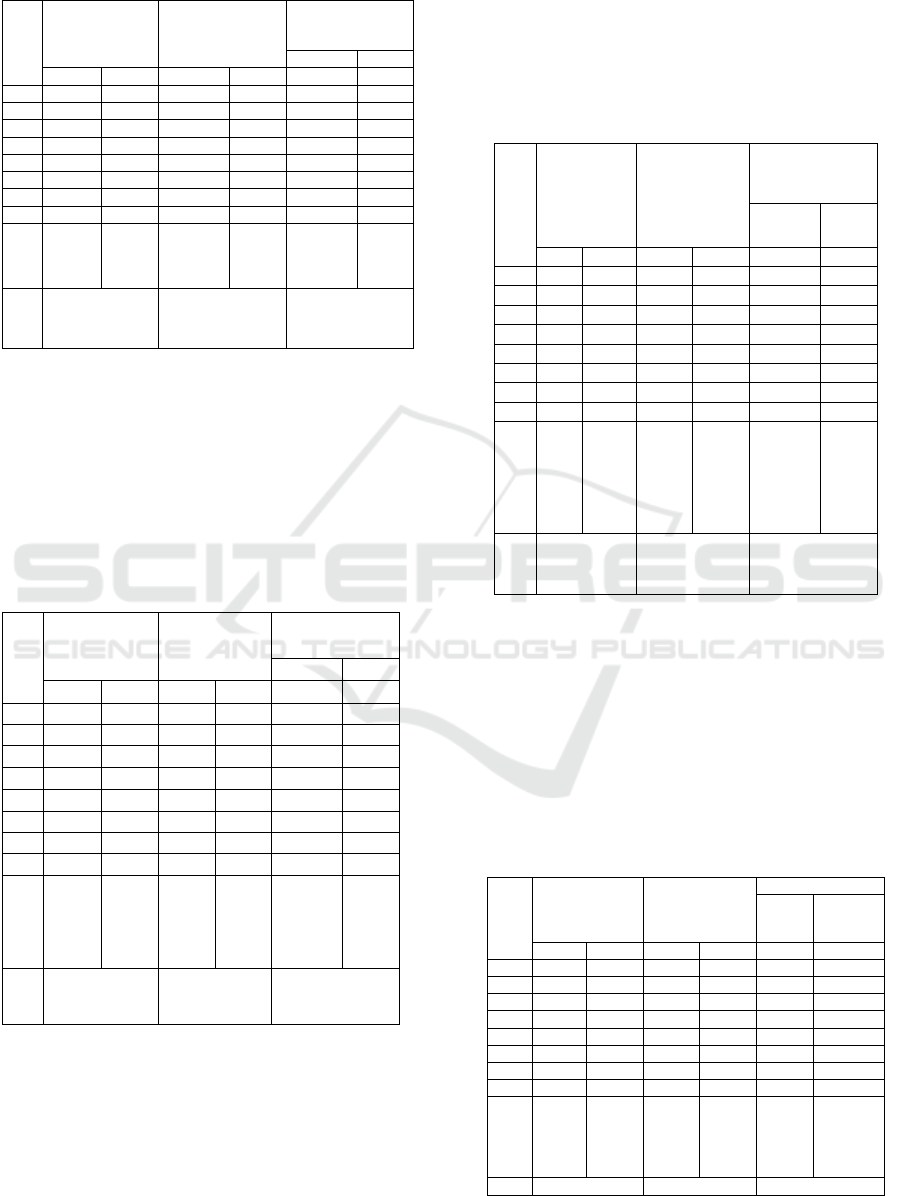
Table 1 : Level of Adversity Quotient of HIV & AIDS
patients in IDITU Clinic, Dr. Soetomo Hospital.
No
Adversity
Quotient
Intervention
Adversity
Quotient
Control
Adversity
Quotient
Intervention Control
Pre Post Pre Post Post Post
1 71 74 70 72 74 72
2 67 78 67 66 78 66
3 72 75 64 70 75 70
4 70 80 71 70 80 70
5 83 82 68 69 82 69
6 66 77 80 78 77 78
7 68 75 74 70 75 70
8 71 74 71 72 74 72
Mea
n
SD
70,75
5.338
54
77
2.828
43
70,625
4.83846
70,87
5
3.440
83
77
2.82843
70,87
5
3.440
83
Uji Wilcoxon
p = 0,017
Uji Wilcoxon
p = 0,943
Uji MannWhitney
p = 0,003
The test results show the value (p) = 0.017. This
significance value is less than 0.05, indicating the
effect of extrinsic motivation on Adversity Quotient
in HIV & AIDS patients.
3.2 Response of Control Dimension
The first dimension of Adversity Quotient is control,
response of control dimension as table below.
Table 2 : Response of control dimension.
No
(Control)
Intervention
(Control)
Control
(Control)
Intervention Control
Pre Post Pre Post Post Post
1 14 14 14 14 14 14
2 15 17 16 15 17 15
3 16 17 12 14 17 14
4 13 15 15 16 15 16
5 18 18 13 13 18 13
6 13 16 17 16 16 16
7 12 18 12 15 18 15
8 15 16 16 17 16 17
Mea
n
SD
14,5
1.927
25
16,3
75
1.40
789
14,3
75
1.92
261
15,0
0
1.30
931
16,375
1.4078
9
15,0
0
1.30
931
Uji Wilcoxon
p = 0,027
Uji Wilcoxon
p = 0,236
Uji
MannWhitney
p = 0,008
Test results show the value (p) = 0.027. This
significance value is less than 0.05, indicating the
presence of the effect of extrinsic motivation on
control responses in HIV & AIDS patients.
3.3 Response of Cause/ Origin
Dimension
The second dimension of Adversity Quotient is
cause dimention, response of cause/origin dimension
as table below.
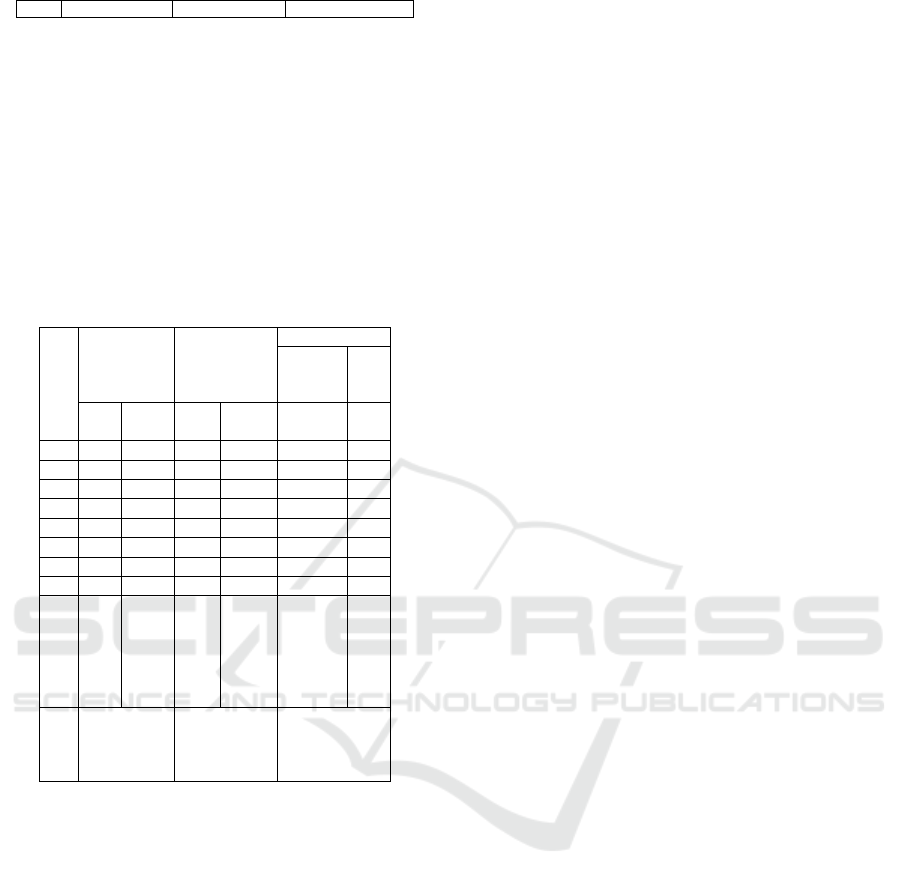
Table 3 : Response of cause/origin dimension
No
(Origin)
Interventio
n
(Origin)
Control
(Origin)
Intervention Control
Pre Pos
t
P
r
ePos
t
Pos
t
Pos
t
1 16 17 16 15 17 15
2 14 18 15 16 18 16
3 18 20 19 15 20 15
4 16 21 16 17 21 17
5 21 20 14 15 20 15
6 12 15 20 19 15 19
7 17 18 19 18 18 18
8 18 19 12 11 19 11
Mean
SD
16,
5
2.7
25
54
18,5
1.92
725
16,3
75
2.77
424
15,7
5
2.43
487
18,5
1.9272
5
15,7
5
2.43
487
Uji
Wilcoxon
p = 0,028
Uji Wilcoxon
p = 0,366
Uji
MannWhitney
p = 0,028
The test results show the value (p) = 0.028. This
significance value is less than 0.05, indicating the
persence of the effect of extrinsic motivation on the
origin response in HIV & AIDS patients.
3.4 Response of Ownership Dimension
The third dimension of Adversity Quotient is
ownership dimention, response of ownership
dimension as table below.
Table 4 : Response of ownership dimension
No
(Ownership)
Intervention
(Ownership)
Control
(
Ownershi
p)
Interven
tion
Control
Pre Post Pre Post Post Post
1 17 19 18 19 19 19
2 18 18 17 17 18 17
3 19 18 15 15 18 15
4 17 19 16 15 19 15
5 15 15 18 17 15 17
6 16 17 19 18 17 18
7 17 16 16 14 16 14
8 16 16 18 20 16 20
Mean
SD
16,87
5
1.246
42
17,25
1.488
05
17,12
5
1.356
2
16,87
5
2.100
17
17,25
1.488
05
16,875
2.10017
U
j
i Wilcoxon U
j
i Wilcoxon U
j
i MannWhitne
y
Effect of Extrinsic Motivation on Adversity Quotient in Patients With HIV AIDS
287
p
= 0,334
p
= 0,589
p
= 0,721
Test results show the value (p) = 0.334. This
significance value is greater than 0.05, indicating no
effect of extrinsic motivation on ownership
responses in HIV & AIDS patients.
3.5 Response of Reach Dimension
The fourth dimension of Adversity Quotient is reach
dimention, response of reach dimension as table
below.
Table 5 : Response of reach dimension
N
o
(Reach)
Interventio
n
(Reach)
Control
(Reach)
Interve
ntion
Co
ntr
ol
Pr
e
Post Pre Post Post Po
s
t
1 9 9 6 7 9 7
2 11 12 5 5 12 5
3 7 9 6 6 9 6
4 8 10 9 8 10 8
5 11 10 7 8 10 8
6 10 11 7 7 11 7
7 7 7 6 4 7 4
8 9 9 9 9 9 9
M
ea
n
S
D
9,0
0
1.6
03
57
9,62
5
1.50
594
6.8
75
1.4
577
4
6,75
1.66
905
9,625
1.5059
4
6,7
5
1.6
69
05
Uji
Wilcoxon
p = 0,129
Uji
Wilcoxon
p = 0,705
Uji
MannWhitne
y
p = 0,003
The test results show the value (p) = 0.129. This
significance value is greater than 0.05, meaning
there is no effect of extrinsic motivation on reach
response in HIV & AIDS patients.
Table 1 shows the effect of extrinsic motivation
on Adversity Quotient response in HIV & AIDS
patients with significance (p) = 0.017. Quantitative
results have been significant, but there were still
respondents who have not made maximum efforts in
overcoming difficult times since the diagnosis of
HIV. This was indicated by patients who did not
increase the value of Adversity Quotient. Stoltz
(2004) suggests that Adversity Quotient is a
snapshot of one's response habits to adversity, a
consistent measure of the subconscious pattern that
has been developed by individuals for many years.
Adversity Quotient is a conceptual framework
capable of predicting an individual's ability to
overcome life's difficulties. The struggle to reach the
goal and struggle to face the existing obstacles is
analogous to the journey up the mountain. Adversity
Quotient is a conceptual framework that can predict
which individuals are capable and unable of coping
with life's difficulties.
Adversity Quotient is used to help individuals
who have to bounce back from each setback and
strengthen resistance to their illness. The existence
of motivation, social support, and the opportunity to
express feelings are able to push the patient toward a
good level of health and provide much information
related to their illness. This is especially desirable,
especially for new patients, as reflected in the
enthusiasm of new patients on given activities as
well as demonstrated by a substantial increase in AQ
in patients who have just been diagnosed.
Nasronudin (2005) states that people with HIV &
AIDS have severe psychological adaptations due to
positive results on blood samples. This greatly
affects the patient's psychological psyche and affects
the patient's immunity level. According to the theory
of psychoneuroimmunology, as the foundation for
the formation of Adversity Quotient, there is a
significant effect of the patients' resistance on the
course of the disease (increasing HIV virus results in
CD4 decline).
Factors that are quite influential on the course
of the disease in boosting immunity depends on the
individual themself. The attitude of HIV & AIDS
sufferers in facing the health condition in the future
certainly will not be much different with the
assessment of his fighting power. As an assessment
of the ability or resilience in facing difficulties in the
face of illness, Adversity Quotient includes an
assessment of whether a person feels a useful
person, has many abilities and beliefs to live a
normal life even though they are infected with HIV,
has resilience in the face of problems, and has
control over an event that creates difficulties. This
will have a great influence on the patient's immunity
and immunity.
A person with a high level of Adversity Quotient
will tend to have a positive attitude towards
everything. In people with HIV & AIDS, this level
of Adversity Quotient will have an effect on their
attitude in dealing with the cure of their illness. A
positive attitude towards the cure of their illness
helps the patient to a more constructive coping and
increasing expectations, with extrinsic motivation in
the form of social support, assisting the patient in
expressing feelings when first diagnosed, helping the
patient to respect themself and accept the condition
sincerely, the importance of the patient to others and
direct the patient to remain active in following
ICPS 2018 - 2nd International Conference Postgraduate School
288

beneficial activities, and can be useful for others.
This optimistic attitude will synergize all activities
to improve the health of the patients themselves,
regular visits, obedience in taking ARVs, and other
activities that support healing. It turned out to be
proved by the results of data analysis conducted in
this study. The results show the existence of
extrinsic motivation influence on Adversity Quotient
in HIV AIDS patients.
Table 2 shows the effect of extrinsic motivation
on the control response in HIV & AIDS patients,
with significance (p) = 0.027. These results indicate
that the ability of the patient to reverse the difficulty
and then turn into opportunity and change the sense
of helplessness to empowerment still varies.
However, the trend shows a relatively moderate
value. The control response shows how a person
controls an event that causes difficulties in their life.
Control response in HIV & AIDS patients shows an
improvement as seen in the patients' better feelings
when doctors state the diagnosis, and the patient
remains convinced that every disease has its own
remedy and believes there is a way out of the
problem.
The spirit to keep on fighting, even with positive
HIV, is present after the provision of extrinsic
motivation. Control begins with the understanding
that anything can be done. Patients with high AQ
feel higher control over their illness than patients
with low AQ. As a result, the patient takes action
that results in more control. Significance value of
control response had (p) = 0.027, indicating that
people with HIV & AIDS have control over events
when they were diagnosed. Welles (2000) says that
people who have good control tend to have a high
AQ. They do not blame others for their illness and
have responsibility for what they did in the past.
Finally, individuals who have a high AQ assume that
the problem they face is in a small sphere and they
are confident to deal with it.
Stolz (2004) argues that control is one of the
most important origins in feelings, which is
reinforced by Seligman's optimistic theory of
optimism which takes account of the impact a
person has on responding and handling adversity.
Good self-control enables the patient to control
themself against adverse situations, both from illness
or from the environment, including the stigma of
society towards people with HIV. Good control can
shape optimism in the face of adversity.
Table 3 shows the effect of extrinsic motivation
on the origin dimension in HIV & AIDS patients,
with significance (p) = 0.028. Patients with low AQ
tend to place undue guilt over the bad events that
occur. Low origin responses can stop feedback
because of the constant burden of self-blame. Like
critics, guilt and regret will be of little use. If guilt is
too great it can be debilitating and deconstructive,
destroying energy, hope, self esteem and the
immune system.
This result gives an illustration of the degree of
recognition of the patients that the self as the origin
of a difficulty (current illness) experienced
(expressed with guilt and regret). The sense of
responsibility for the consequences of a difficulty
was at a moderate level. Original response reveals
who or what causes a difficulty. This variable has a
link to guilt. Guilt has two important functions. First,
if the guilt is of the right level, that feeling will
cause a person to act towards improvement and help
in a state of healing. Second, if the guilt leads to
regret, it will cause a sense of destruction.
Destructive guilt destroys hope, motivation and
energy. The response of origin in HIV & AIDS
patients increased, indicated by the guilt of the
patients to the family and close friends due to HIV
positive diagnosis. The origin response is a
perception of the origin of the difficulty (starting
from the beginning of HIV) until the patient is able
to place guilt as constructive or destructive.
Table 4 shows there is no effect of extrinsic
motivation on the dimension of ownership in people
with HIV & AIDS. Although the average value
showed an increase, the (p) was 0.334. Stolz (2004)
argues that the lower the level of recognition, the
more likely it is not to recognize the consequences.
The tendency to dismiss bad events or avoid
responsibility is an unwelcome attitude.
Ownership responses reveal aspects of
recognition of adversity. Patients with high AQ tend
to acknowledge the consequences of difficulty, often
able to remember the cause. Such a sense of
responsibility forces them to act, making the patient
improve their health level more. The significance
value of ownership variable was (p) = 0.334. From
the results of this study it can be assumed that
people with HIV & AIDS less recognize the cause of
the arising difficulties, but there is still a sense of
responsibility to overcome these conditions. The
absence of influence on this dimension is due to the
inability of the patient to affirm the importance of
themself to others. Response of ownership of HIV &
AIDS is indicated in responsibility and acceptance
of the disease suffered.
Table 5 shows the effect of extrinsic motivation
on the reach dimension in HIV & AIDS patients.
Although the mean score indicates an increase, the
(p) was 0.129, and the significance of the Mann-
Effect of Extrinsic Motivation on Adversity Quotient in Patients With HIV AIDS
289

Whitney test showed the significance difference of
post-treatment group values and post-control group
values with (p) = 0.003.
Stolz (2004) states that responses with low AQ
will cause the difficulties to extend to other facets of
life. Conversely, the range limitations will be even
greater. These results illustrate the ability of HIV &
AIDS patients to limit the adverse effects of the
progression of their illness to other parts of their life
at a moderate level. Reach describes the level of
arising difficulties that reaches other parts of one's
life. The significance value was 0.129, so it was
assumed that people with HIV & AIDS responded to
adversity in an unlimited and widespread way.
Response reach in patients is indicated by the
family caring for the patient. On the other hand, the
patient themself feels that they themself have
troubled the others. Reach here covers the closeness
of the patient with family and close friends. The
patient will fall and drop if the family blames the
patient for their illness being the result of their own
fault.
Stoltz (2004) argues that a person with a high
endurance response rate assumes that the cause of
adversity is temporary, rapidly passes and less likely
to occur, which means not significant. Extrinsic
motivation has no effect on the endurance dimension
because the difficult times experienced by HIV &
AIDS patients are permanent. This is because the
patient must consume drugs continuously and
always keep the body condition so as not to decline.
4 CONCLUSIONS
Extrinsic motivation with social support
interventions has a positive effect on Adversity
Quotient improvement in HIV & AIDS patients. The
level of Adversity Quotient of HIV & AIDS patients
will have an effect on their attitude in dealing with
the cure of their illness. HIV & AIDS patients who
are extrinsically motivated will affect the control
response to the disease. The responsiveness of the
control dimension is influenced by the perception of
control over the bad situations, both from oneself
and the environment, and optimism in the face of
adversity.
Extrinsic motivation positively affects the
response of the origin dimension in HIV & AIDS
patients. This dimensional response is influenced by
feelings of guilt as constructive, supported by nurses
who can provide feedback on their behavior.
Patients with HIV & AIDS who had extrinsic
motivation did not show any change in response of
ownership dimension. This ownership dimension
response is influenced by the efforts of nurses in
affirming the importance of the patient to others
(family or friends).
Patients with HIV & AIDS who received
extrinsic motivation showed no significant change in
response to reach dimension and endurance
dimensions. The response to reach is influenced by
the impact of specific or extended difficulties, while
the endurance response is affected by time in the
face of adversity and the expectations in the face of
adversity itself.
ACKNOWLEGEMENTS
I am grateful to all of those with whom I have had
pleasure to work during this project. Each of the
members of my thesis committee has provided me
with extensive personal and professional guidance
and taught me a great deal about both scientific
research and life in general. I would especially like
to thank Dr. Nursalam, the chairman of my
committee. As my teacher and mentor, he has shown
me, by his example, what a good researcher should
be.
REFERENCES
Ahmadi, A. 1998. Psikologi Umum. Jakarta: Rineka Cipta.
Arikunto. 2002. Manajemen Penelitian. Edisi 5. Jakarta:
Rineka Cipta, Hal: 178-198.
Boenisch, E. dan Haney, C. M. 1998. Menggapai
Keseimbangan Hidup. “The Stress Owner’s Manual
Meaning, Balances & Health In Your Life”.
Terjemahan oleh Oka Joehana. 2005. Jakarta:
Gramedia.
Bunner dan Suddart. 2002. Buku Ajar Keperawatan
Medical Bedah, Sneltzen’s Texbook of Medical
Surgical 8th Edition. Terjemahan oleh W Agung.
Jakarta: EGC
Chotimah, K. 2005. Hubungan antara Adversity Quotient
dengan Perilaku Produktif Pada Wanita Peran Ganda
di PT. Telkom Kantor Divisi Regional V Jatim.
Skripsi tidak dipublikasikan, Fakultas Psikologi
Universitas Airlangga Surabaya.
Encyclopedia Britanica. 2006. Artikel Learning Theory
Education Philosophy of Meaning of Life.
(Online)(http://british.net/edu/, diakses 13 Februari
2008).
Faqih, A. 2007. Sekilas Tentang Motivasi Berprestasi
(Online) (http://psikologi/net/, diakses 24 April 2008).
Frank, J. L. Tanpa Tahun. Psychology The Science of
People, 2nd Edition. Lippincoln hal 147, 196.
Green, C. W. 2006. Laporan Lokakarya HIV dan AIDS
ASEAN dan Jepang. Artikel. Jakarata: Yayasan
Spritia, 12 Nov 2006.
ICPS 2018 - 2nd International Conference Postgraduate School
290

Hudzaifah. 2005. Hakikat Memotivasi Diri:
Kajian/Akhlaq dan Kepribadian. (Online)(
http://www.hudzaifah.org/ diakses 26 April 2008).
KPA (Komisi Penanggulangan AIDS) Nasional, Tanpa
Tahun. Mengenal dan Menanggulangi HIV AIDS.
Jakarta: Press.
Kustanti, E. K. 2006. Hubungan Antara Tingkat Adversity
Quotient dengan Sikap Menghadapi Masa Depan Pada
Remaja yang Tinggal di Panti asuhan Yayasan
Wakhid Hasyim Surabaya. Skripsi tidak
dipublikasikan, Fakultas Psikologi Universitas
Airlangga Surabaya.
Lee, J. V. 2005. Pure Power Inti Pemberdayaan Pribadi
yang Luar Biasa. Jakarta: Bhuana Ilmu Populer.
Maramis, M. M. 2005. ”Manfaat Psikoterapi” dalam
Psikoneuroimunologi Kedokteran editor Taat Putra.
2005. Surabaya: Gideon Offset.
Misutarno. 2006. Hubungan Penerapan Exercise (Senam)
terhadap Peningkatan Limfosit T-CD4 Pada Pasien
HIV-AIDS di Unit Perawatan Intermediet Penyakit
Infeksi RSU Dr. Soetomo Surabaya. Skripsi tidak
dipublikasikan, Program Studi S1 Ilmu Keperawatan
Fakultas Kedokteran Universitas Airlangga Surabaya.
Mulyana, I. 2007. Tujuh Teori Motivasi. (Online)
(http://oeconomicus.wordpress.com/ diakses 27 April
2008).
Muma, R. D. Lyons, B. A. Borucki, M. J. Pollard, R. B.
1997. Aspek Sosial dan Psikologis dari AIDS. Dalam:
HIV Manual untuk Tenaga Kesehatan. Edisi Bahasa
Indonesia (Prawitasari S) editor Anugerah P, Asih Y.
Jakarta: EGC hal 275.
Nasronudin. 2005. ”Pengaruh Psikososial Terhadap
Perkembangan Infeksi HIV Menjadi AIDS” dalam
Psikoneuroimunologi Kedokteran editor Taat Putra.
2005. Surabaya: Gideon Offset.
Nasronudin. 2007. Infeksi Human Immunodeficiency
Virus. Makalah disampaikan dalam seminar Februari
2007. Fakultas Kedokteran Universitas Airlangga.
Niniek, L. P. 2004. Pengaruh Self Eficacy Melalui
Kemampuan Kognitif, Motivasi dan Afektif Kader
Kesehatan Gigi Terhadap Perilaku Sehat Gigi.
Disertasi tidak dipublikasikan Program Pascasarjana
Universitas Airlangga surabaya.
Nursalam. 2007. Asuhan Keperawatan pada Pasien
Terinfeksi HIV dan AIDS. Jakarta: Salemba Medika,
hal:15-16, 24-27, hal 30.
Nursalam, 2003. Konsep dan Penerapan Metodologi
Penelitian Ilmu Keperawatan: Pedoman Skripsi, tesis,
dan Instrumen Penelitian Keperawatan. Jakarta:
Salemba Medika.
Nursalam, 2005. Efek Model Pendekatan Asuhan
Keperawatan (PAKAR) terhadap Perbaikan Respons
Kognisi dan Biologis pada Pasien terinfeksi HIV.
Disertasi tidak dipublikasikan Program Pascasarjana
Universitas Airlangga.
Oktaviyanti, V. 2006. Kualitas Hidup ODHA (Orang
dengan HIV dan AIDS) Diitinjau Dari Efektifitas
Komunikasi dalam Keluarga. Skripsi tidak
dipublikasikan, Fakultas Psikologi Universitas
Airlangga Surabaya.
Oliver, M. F. dan Peter, J. M. 2007. ”Motivations of The
Ethical Consumen”. Journal of Bussiness Ethic,
(Online E-Library Unair 1 Mei 2008).
Purwanto. 1996. Psikologi Pendidikan. Bandung: Remaja
Rosdakarya.
Riyahmawati, H. 2008. Pengaruh Latihan Asertif terhadap
Dinamika Penyesuaian Emosional Pasien Setelah
Didiagnosa HIV di Unit Perawatan Intermediet
Penyakit Infeksi. Skripsi tidak dipublikasikan,
Program Studi S1 Ilmu Keperawatan Fakultas
Kedokteran Universitas Airlangga Surabaya.
Santrock, J. W. Life Span Development. Jakarta:
Erlangga.
Sara, L. N. 2008. “The Relationship of Acceptance or
Denial of HIV-Status to Antiretriviral Adherence
Among Adult HIV Patients in Urban Botswan Social”.
Science and Medicine, (Online-E-Library Unair)1 Mei
2008.
Stoltz, P. G. 1997. Adversity Quotient Mengubah
Hambatan Jadi Peluang. Terjemahan oleh Hermaya T.
2004 Jakarta: Gramedia.
Sudrajat, A. 2007. Teori-Teori Motivasi (Online)
(http://akhmadsudrajat.wordpress.com/ diakses 27
April 2008).
Tandiono, E. Wibisono, S. Darmabrata, W. 2007. Peran
Consultation-Liaison Psychiatry pada Penatalaksanaan
Pasien Dengan HIV dan AIDS. PPDS Bagian
Psikiatri, Fakultas Kedokteran Universitas Indonesia
RSUPN Dr. Cipto Mangunkusumo, Jakarta
Tim PSIK. 2007. Buku Pedoman Penyusunan Proposal
dan Skripsi. Surabaya: Airlangga Press.
Wardhani, J. H. 2003. Pengaruh Tingkat Adversity
Quotient (AQ) terhadap Orientasi Karir di PT. Danzas
Surabaya dan Jakarta. Tesis tidak dipublikasikan,
Program Studi Pengembangan Sumber Daya Manusia
Minat Studi Bisnis & Industri Pasca Sarjana
Universitas Airlangga Surabaya.
Widyawati, I. Y. 2005. Pengaruh Dukungan Keluarga
terhadap Perubahan Respons Sosial Emosional Pasien
HIV dan AIDS di Unit Perawatan Intermediet
Penyakit Infeksi RSUD. Dr. Soetomo Surabaya.
Skripsi tidak dipublikasikan, Program Studi S1 Ilmu
Keperawatan Fakultas Kedokteran Universitas
Airlangga Surabaya.
Yahya, H. 2007. Stress dan depresi Akibat Tidak
Menjalankan Agama. (Online) (http://www.
harunyahya.com/indo/artikel/076.htm, diakses 19
Februari 2008)
Effect of Extrinsic Motivation on Adversity Quotient in Patients With HIV AIDS
291
