
Digital LOTCA
How to Evaluate Acquired Brain Injury using Technology
Cristian Cuerda
1
, Jose A. Gallud
1
, Ricardo Tesoriero
1
and Habib M. Fardoun
2
1
Research Institute of Informatics, UCLM, Albacete, Spain
2
Ahlia University, Bahrein
Keywords:
LOTCA, Occupational Therapy, Distributed Interfaces, API Rest, Cross Platform Development.
Abstract:
In this article, we are going to describe the solution proposed to help people with acquired brain damage,
consisting of a service-oriented application, which provides a platform in which different tests are used that
are used in the test battery of cognitive evaluations of occupational therapy of Loewenstein. This platform
allows the patient to perform the tests on a touch screen, while the therapist can observe the results of the test
in real time on a monitor.
1 INTRODUCTION
First, we are going to define what is the Brain Da-
mage Injury, and what is the current situation of this
type of brain injuries in the world. Acquired Brain
Injury (ABI) is the involvement of brain structures
in people who, having been born without any type of
brain injury, suffer at a later time in their lives, brain
injuries that cause an impairment of cognitive, emo-
tional, behavioral and/or physical functioning. This
injury is a major health problem, due to the high num-
ber of people affected (more than 400,000 in Spain),
the duration, severity and variety of sequelae. The
ABI represents the main cause of disability in adults
in developed countries (Cerebral Injury Association
of Navarra, 2014).
The causes by which this type of injury can be ge-
nerated are very varied, and include (Cerebral Injury
Association of Navarra, 2014):
• Cranioencephalic trauma: is the brain injury from
a trauma or blow. The most frequent causes are
traffic accidents (in 80 % of cases), work acci-
dents and sports accidents.
• Stroke: cerebrovascular accidents are injuries re-
sulting from an interruption of the cerebral blood
flow system, such as embolisms and thrombosis,
or cerebral hemorrhages, including ruptured aneu-
rysms, or malformations of the veins and arteries
that irrigate the brain.
• Anoxies or hypoxia: it is the absence or poor oxy-
genation of the brain during a certain time, which
causes the neuronal death of part of the brain tis-
sue.
• Brain tumors: both the tumor itself and the proce-
dures aimed at its elimination (surgery, radiation)
cause important damage to the surrounding brain
tissue.
• Other causes: iencephalitis of various etiologies,
which may be a consequence of infectious, viral,
or toxic poisoning processes.
In the Figure 1 we can see a graphic overview of the
incidence and prevalence of ABI in Spain.
The ABI can affect all areas of human functioning.
The affected area and therefore the deficits presen-
ted by the affected person will depend on the type of
injury, the initial location and severity of the injury;
as well as the characteristics of each affected person
such as age, personality or abilities prior to the in-
jury. The sequels are grouped into four dimensions
that may or may not be present in the same person
(Red Menni of Cerebral Injury, 2015):
• Physical-motor deficits: There may be alterations
in balance, inability to stand, inability to walk, li-
mitations in the movement of one or more limbs,
or even control of the trunk and head at rest.
• Cognitive deficits: for example, deficits in le-
arning and memory, attentional deficits, lan-
guage alterations, alterations in formal thinking
(logical-deductive reasoning, problem solving,
abstraction) and alterations in the regulation of
proactive or targeted behavior (planning, initia-
tion and behavioral self-regulation).
Cuerda, C., Gallud, J., Tesoriero, R. and Fardoun, H.
Digital LOTCA - How to Evaluate Acquired Brain Injury using Technology.
DOI: 10.5220/0006940807730779
In Proceedings of the 13th International Conference on Software Technologies (ICSOFT 2018), pages 773-779
ISBN: 978-989-758-320-9
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
773
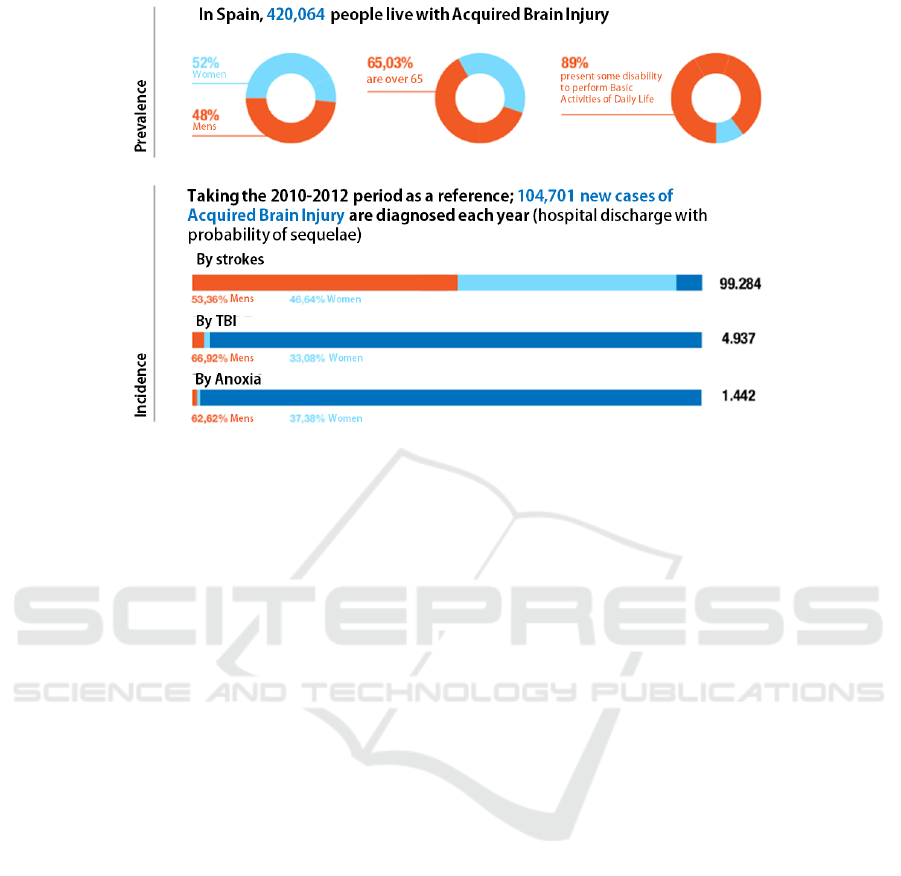
Figure 1: Incidence and prevalence of ABI in Spain.
• Alterations in communication: occur due to the
alteration of physical and cognitive abilities or the
combination thereof. In the case of physical alte-
rations, oral, written or comprehension expression
is affected. There are also language alterations
that produce the inability for oral expression or
comprehension, despite the fact that the physical-
motor system remains intact.
• Behavioral and/or Emotional Alterations: At the
same time that the cognitive alterations appear be-
havioral and/or emotional alterations associated
with changes of character or personality. The ori-
gin of behavioral alterations could be considered
in two ways: lack of inhibition, sometimes cau-
sing physically or verbally aggressive behaviors
or excessive inhibition or poor behavioral initia-
tive, in which the affected shows apathy not initi-
ating activities if not explicitly asked , he does not
enjoy the things that he used to enjoy so much,
he has a feeling of exhaustion and lethargy, and
on the emotional level he hardly expresses emoti-
ons. When an ABI occurs, there is a sudden break
with the occupational roles that the person played
until the time of injury. This usually causes that
suddenly, the person suffering a brain injury mo-
ves from a balanced and active occupational rea-
lity to a situation in which he becomes a passive
recipient of care. Then, as he recovers capacities,
he finds himself in a situation of significant decre-
ase in the level of participation, being unable or
depending on help to perform a large number of
activities.
As indicated by (Spanish Federation of Cerebral In-
jury, 2014), in the process of rehabilitation of Acqui-
red Brain Injury it has five objectives:
• Evaluate the sequelae of brain damage and the dif-
ficulties they cause.
• Reeducate and compensate for the sequelae of
brain damage to reduce disability.
• Prevent future complications of the sequelae of
the ABI or of the brain injury itself.
• Enhance conserved skills.
• Promote social and family integration.
Our solution focuses on this first stage of the re-
habilitation of brain injury, the evaluation of the se-
quels produced and the difficulties or deficits that
these cause. For this, we have started from a tradi-
tional methodology in this area called LOTCA, and
we have created a digital platform that makes it easier
to diagnose and assess the therapist.
2 OCCUPATIONAL THERAPY IN
ACQUIRED BRAIN INJURY
Loewenstein’s Occupational Therapy Cognitive As-
sessment (LOTCA) (Katz N., 1989) battery of eva-
luation was developed as a technique used to mea-
sure basic cognitive abilities and visual perception in
adults with neurological disabilities. It provides an
in-depth evaluation of basic cognitive skills and it can
IDEE 2018 - Special Session on Interaction Design in Educational Environments
774

be used for treatment planning and review of treat-
ment progress (McDermott, 2011). The LOTCA bat-
tery measures the basic cognitive abilities required for
daily functions including orientation, visual percep-
tion and psychomotor skills, problem solving abili-
ties and thought operations. The development of this
battery is based on information obtained from clinical
and neuropsychological experience and development
theories.
Usually, LOTCA is used in the initial stage of the
evaluation of patients, but it can be used to establish
therapeutic goals and review the cognitive status over
time (Annes G., 1996) (Zwecker M, 2002) The ori-
ginal version of LOTCA (Katz N., 1989) was deve-
loped to be used by individuals under 70 with neu-
rological dysfunction and was made up of 20 items
grouped into 4 areas: Orientation, (2 items), percep-
tion (6 items), visual-motor organization ( 7 items)
and thought operations (5 items).
Next, we will proceed to describe the characteris-
tics of the specific measurement of each one of the
aforementioned areas:
• Orientation: the tests in the area of orientation
evaluate the orientation of the individual in space
and time.
• Visual perception: tests in the area of visual per-
ception evaluate the individual’s ability to identify
images of everyday objects, objects photographed
from unusual angles, distinguish between supe-
rimposed figures and recognize spatial relations-
hips between objects.
• Spatial perception: the tests related to spatial per-
ception evaluate the ability of the individual to dif-
ferentiate between right and left, to determine the
spatial relationships between objects and himself.
• Motor praxis: the tests related to motor praxis eva-
luate the ability of individuals to imitate motor
actions, use objects and perform symbolic actions.
• Visuomotor organization: the tests related to the
visual-motor organization evaluate the ability of
the individual to copy geometric figures, repro-
duce a two-dimensional model, copy a design of a
colored block and a clean block design, reproduce
a puzzle, a complete task of a peg board and draw
a clock.
• Thought operations: thinking operations evaluate
the individual’s ability to complete tasks that in-
clude: ordering, categorizing and drawing geome-
tric sequences (Annes G., 1996).
These analyzes have been standardized for the Is-
raeli population (Annes G., 1996) (Cermak S. A.,
1995) and suitable for use in the populations of the
United States (Katz N., 1997). Regarding the evalua-
tion time, LOTCA and LOTCA-II take approximately
45 minutes, with a range that ranges between 30 and
90 minutes (Annes G., 1996) (Zwecker M, 2002).
Regarding the suitability of individuals, LOTCA
can be used with:
• Patients who have had a stroke, cardiovascular ac-
cident, stroke, stroke, cerebrovascular accident,
etc. (Bar-Haim Erez A., 2003)
• Elderly individuals with dementia (Bar-Haim
Erez A., 2003).
• Individuals with traumatic brain injuries (An-
nes G., 1996).
• Individuals with intellectual disabilities (Jang Y.,
2009) and mental illness (Josman N., 2006) can
also use it.
• An adapted version was developed for children
with learning difficulties (Josman N., 2010).
• Patients with aphasia (Jang Y., 2009).
3 ARCHITECTURE OF THE
SOLUTION
So far we have studied how technology can help diag-
nose and evaluate people with Acquired Brain Injury,
and what are the most common techniques used today.
Next, we will explain the solution we propose.
The proposed solution, briefly explained, consists
of a client-server application, in which the therapist
can create a personalized session for his patient, in-
cluding data such as his name or the patient’s own.
This session contains a test of the battery proposed
by LOTCA, belonging to the area of operations of
thought.
If we performed this test in a traditional way, the
therapist would provide the patient with a set of cards
containing different geometrical shapes with different
colors, and the patient should group them according
to the pattern provided by the therapist.
To carry out this task, our solution proposes a dis-
tributed application, in which the patient will work on
a touch screen solving the test, while the therapist ob-
serves the results in real time on another screen that
will act as a monitor. In this test, the patient will be
shown a set of cards with geometrical figures of dif-
ferent colors.
There are six different types of figures, and each
of them is represented in three different colors, there
being a total of eighteen different cards. The patient
must group these cards according to the parameters
Digital LOTCA - How to Evaluate Acquired Brain Injury using Technology
775
indicated, which may be, for example, by colors, by
shape, repeating a previously given pattern, etc.
The therapist will observe in real time on his mo-
nitor how the patient moves the different cards on the
screen, allowing him to observe and analyze strange
behaviors that indicate that the patient suffers some
type of injury. In addition, he can also view statistical
information such as the total time the session has been
running.
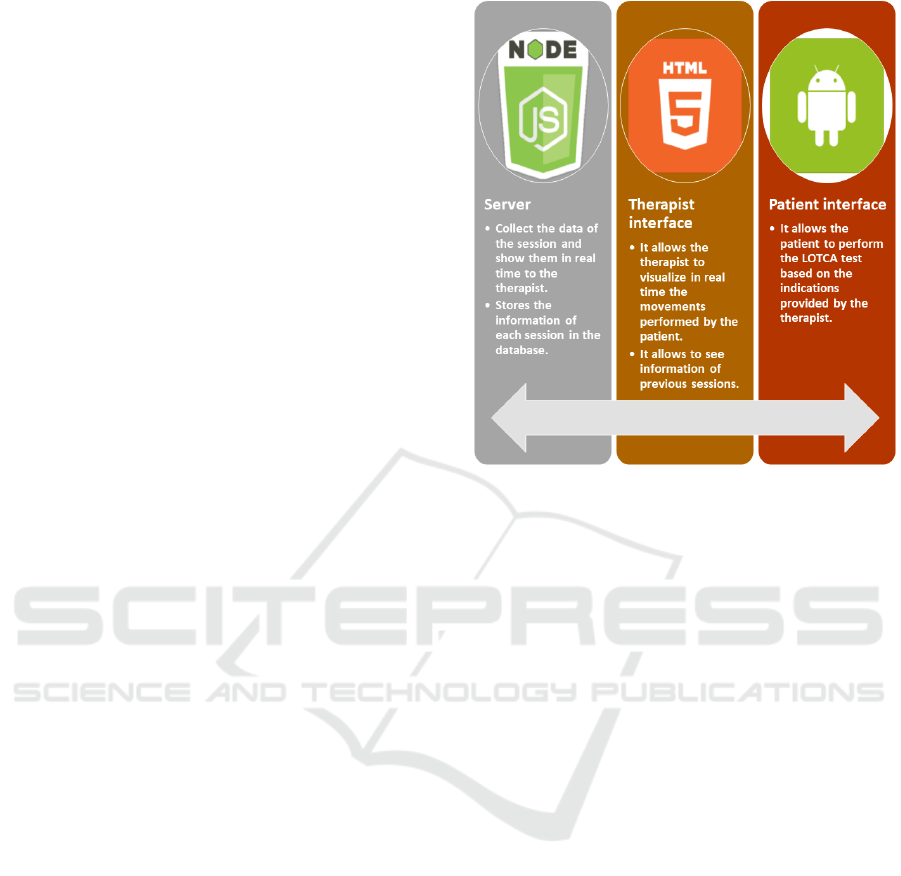
To make this communication distributed between
the screen of the therapist and the patient possible, it
is necessary that there is a server that acts as an in-
termadiary and that collects all the data and proces-
ses them properly. This server, implemented using
Node.js, has a REST services layer and is connected
to a NoSQL database implemented in MongoDB, in
which the data is stored in the session. The server
is responsible for collecting the information that the
therapist introduces about the session he want to cre-
ate, processes them and generates the test, allowing
the patient to connect to that session. Once the pa-
tient connects, it collects all the movements of cards
that it makes, and making use of Web Sockets, sends
them in real time to the therapist’s monitor. In addi-
tion, the server is also responsible for storing all of
this data in the database, so that the information of a
certain session can be viewed at any time.
This can be done using the display module of the
application results. This module allows, given a spe-
cific session that has already been carried out, to visu-
alize which cards have been moved by the patient in a
specific time slot, showing their position of origin, the
path traveled and the final position. The therapist can
modify that time frame to visualize which cards have
moved in different lengths of time. Figure 2 shows
the architecture of the application in a schematic way.
The reason for choosing Javascript and specifi-
cally, Node.js to implement the server, is the high
performance provided by this technology in service-
based applications. Node.js uses an event loop (Event
Loop), which manages all asynchronous operations.
In case of needing a blocking operation, an asynchro-
nous request is sent to that Event Loop together with
a callback, and the server continues with the request
when it can. If we compare it with other technologies
such as PHP and Java, in which every new connection
to the server generates a new thread, with its corre-
sponding memory consumption, Node.js for each new
connection to the server, creates a new event inside
the main engine of Node.js. This translates into great
memory savings and therefore, support for a larger
number of simultaneous requests using fewer resour-
ces. In addition, another of the great advantages is
the ease and speed of implementation and execution
Figure 2: View of the architecture of the application.
of unit tests.
The fact of choosing a NoSQL database like Mon-
goDB is fundamentally due to the advantages that this
type of database provides in matters of performance
and scalability with respect to a SQL database. In the
developed application, we do not work with sensitive
data about patients and, in particular, with data related
to their medical file, which according to Spanish le-
gislation are considered specially protected data. The-
refore, the solution adopted does not require extre-
mely restrictive measures regarding the storage and
processing of data, although it does use encryption in
those data that may lead to the theft of user informa-
tion.
4 WORKING WITH THE
DIGITAL LOTCA
To finish, we will show how the application we have
developed works. First, we will show the functioning
of the therapist’s interface. To access it, the therapist
must enter the application (see Figure 3) and select
the option ”I am the therapist”. Once this is done, the
therapist’s interface will be displayed.
From this interface, the therapist can create a new
session or can visualize information about a session
that he has already done previously. If the therapist
wishes to create a new session, he must enter an iden-
tifier for that session if he wish (although one is pro-
vided automatically), his name and that of the patient
IDEE 2018 - Special Session on Interaction Design in Educational Environments
776

Figure 3: Main user interface selection menu.
Figure 4: Menu to create a new session.
who is going to perform the session, as shown in the
Figure 4. Once the session is created, an interface will
be displayed in which the patient’s screen is included,
which will be shown empty until the patient enters the
session, and a lateral menu in which the cards can be
shuffled in case the order in the one that appears is not
the right one, end the session, or handle the chrono-
meter that measures the times of the session, as seen
in the Figure5.
Figure 5: The therapist’s interface before the patient enters.
Once this is done, the patient accesses the session
that has been created. To do this, hr must select the
option ”I am the patient” in the main application menu
(Figure 3). Then, he must enter the identifier of the
session that the therapist chose when creating the ses-
sion (Figure 6)
When the patient joins the session, only the set of
cards necessary to complete the session will be shown
on the screen. When working with a touch screen,
he can freely drag those cards to group them follo-
wing the pattern proposed by the therapist based on
Figure 6: Menu to join a session.
Figure 7: Patient interface when joining the session.
the LOTCA test (Figure 7).
In the therapist’s interface, the patient’s screen is
now displayed, and each movement of cards that he
makes can be seen in real time from the therapist’s
interface, as shown in the 8.
Figure 8: The therapist interface when the patient joins the
session.
On the other hand, the therapist is offered the op-
tion of viewing information about previous sessions.
To do this, he must first enter the identifier of the ses-
sion he wants to view, as shown in the Figure 9.
When he has entered the identifier, a visuali-
zer will be displayed where the therapist can scroll
through the bar that appears at the bottom of the
screen for the different moments of time the session
has. On the right side, he can edit the time slot over
which information is displayed, expressed in seconds.
For example, if the therapist moves with the lower bar
to position 20 and in the menu on the right, selects a
Digital LOTCA - How to Evaluate Acquired Brain Injury using Technology
777

Figure 9: The therapist interface when the patient joins the
session.
step of 5 seconds, the system will show information
about the position occupied by the cards in the second
20 of the session, and about the changes that they have
suffered in the last 5 seconds. For the id, the system
shows highlighted the cards that have moved in that
time slot, while the cards that have not moved, are
shown with a weaker color. In addition, the trajec-
tory followed by the cards displaced in that time slot,
their original position (using a card with the grated
contour) and their final position (using a card with the
solid outline), as shown in the figure 10.
Figure 10: Session history viewer interface.
5 CONCLUSIONS
As a summary, we can say that our solution allows di-
gitizing and computerizing a set of tests proposed in
the LOTCA methodology for the diagnosis and eva-
luation of people with acquired brain damage.
Our solution allows the patient to work in a similar
way to the one he would do if he worked in a tradi-
tional way, by providing him with a touch screen in
which he can drag and move freely the cards used in
the test.
In addition, our solution allows the therapist to vi-
sualize at all times what movements the patient is per-
forming, without directly interfering with their task,
since they can visualize these movements in a moni-
tor that can be found anywhere. This allows that even
other therapists can visualize that session in real time,
even if they are not physically next to the patient.
The display module of old sessions allows the
therapist to access at any time the information of the
sessions, sharing this information with other collea-
gues who were not present at the time of the test, or re-
turning to analyze the movements that the patient has
made, in order to detect other anomalies that could
not be detected in real time.
Finally, we believe that this platform can conti-
nue to grow, implementing all the tests included in
LOTCA, and thus be able to replace the laborious tra-
ditional tests with these digitized tests.
REFERENCES
Annes G., Katz N., C. S. (1996). Comparison of younger
and older healthy american adults on the loewenstein
occupational therapy cognitive assessment. Occupati-
onal Therapy International, 3:157–173.
Bar-Haim Erez A., K. N. (2003). Cognitive profiles of indi-
viduals with dementia and healthy elderly: The loe-
wenstein occupational therapy cognitive assessment
(lotca-g). Physical and Occupational Therapy in Ge-
riatrics, 22:29–42.
Cerebral Injury Association of Navarra (2014).
https://www.adacen.org/blog/index.php/que-es-
el-dano-cerebral-y-cuales-son-sus-secuelas/.
Cermak S. A., Katz N., M. E. G. S. P. C. F. V. (1995). Per-
formance of americans and israelis with cerebrovascu-
lar accident on the loewenstein occupational therapy
cognitive assessment. American Journal of Occupati-
onal Therapy, 49:500– 506.
Jang Y., Chern J-S., L. K.-C. (2009). Validity of the loe-
wenstein occupational therapy cognitive assessment
in people with intellectual disabilities. American Jour-
nal of Occupational Therapy, 63:414–244.
Josman N., Abdallah T. M., E.-Y. B. (2010). Cultural factors
affecting the differential performance of israeli and
palestinian children on the loewenstein occupational
therapy cognitive assessment. Research in Develop-
mental Disabilities, 31:656–663.
Josman N., K. N. (2006). Relationships of categorization
on tests and daily tasks in patients with schizophrenia,
post-stroke patients and healthy controls. Psychiatry
Research, 141:15–28.
Katz N., Itzkovich M., A. S.-E. B. (1989). Loewenstein
occupational therapy cognitive assessment (lotca) bat-
tery for brain-injured patients: Reliability and validity.
American Journal of Occupational Therapy, 43:184–
192.
Katz N., Champagne D., C. S. (1997). Comparison of the
performance of younger and older adults on three ver-
sions of a puzzle reproduction task. American Journal
of Occupational Therapy, 51:562–568.
McDermott, A. (2011). Loewenstein Occupational Ther-
aphy Cognitive Assessment. Nicol Korner-Bitensky.
Red Menni of Cerebral Injury (2015). http://xn–
IDEE 2018 - Special Session on Interaction Design in Educational Environments
778

daocerebral-2db.es/papel-de-la-terapia-ocupacional-
en-la-rehabilitacion-del-dano-cerebral/.
Spanish Federation of Cerebral Injury (2014).
https://fedace.org/talleres-dano-cerebral.html.
Zwecker M, Levenkrohn S., F. Y.-Z. G. O. A. A. A. (2002).
Mini-mental state examination, cognitive fim instru-
ment, and the loewenstein occupational therapy cog-
nitive assessment: Relation to functional outcome of
stroke patients. Archives of Physical Medicine and
Rehabilitation, 83:342–5.
Digital LOTCA - How to Evaluate Acquired Brain Injury using Technology
779
