
The GezelschApp
A Dutch Mobile Application to Reduce Social Isolation and Loneliness
Stephanie Jansen-Kosterink
1,2
, Patrick Varenbrink
3
and Arno Naafs
4
1
Cluster Telemedicine, Roessingh Research and Development, Enschede, The Netherlands
2
Telemedicine Group, University of Twente, Enschede, The Netherlands
3
Alifa, Enschede, The Netherlands
4
Present Media, Enschede, The Netherlands
Keywords: Older Adults, Loneliness, Social Isolation, Information Communication Technology, mHealth.
Abstract: The social isolation among older adults is a growing concern, as both social isolation and loneliness have been
associated with ill health. Information communication technology can overcome the social and spatial barriers
of social interaction by enabling easy affordable communication and activities of multiple form between older
adults and others anytime and anywhere. Therefore, technology-supported intervention, such as the
GezelschApp could prevent and ameliorate social isolation and loneliness among older adults. The aim of this
paper is to introduce this new technology, to provide an overview of the current evaluation and to present the
intermediate results concerning the usability of end-user acceptance of this technology. The GezelschApp is
a mobile application to reduce social isolation and loneliness among older adults. This application, also
accessible by PC and tablet, gives older adults access to a homepage with six features (an inbox for messages,
news, activities, information, tips and friends). On beforehand interested older adults are screened by a coach
before they receive a personal access code. During the 3 months evaluation of the GezelschApp the usability,
end-user acceptance, level of experienced loneliness and quality of life are assessed. Although the evaluation
of the GezelschApp is still running, the first focus groups (n=10) with users highlight the need of the current
application to make new friends in a save manner and to participate in social activities.
1 INTRODUCTION
As demographic ageing is a global trend, the social
isolation among older adults is a growing concern.
Compared to the general population the prevalence of
social isolation among older adults (60 years and
older) is high. Often loneliness is referred as a
problem specifically for older adults. This is partial
supported by literature as loneliness is common only
among the very old, that is, those aged 80 and over.
(Dykstra, 2009). It is important to draw the distinction
between social isolation and loneliness (de Jong
Gierveld et al., 2006). Social isolation can be defined
as an objective lack of interactions with others or the
wider community and loneliness can be defined as the
subjective feeling of the absence of a social network
or a companion.
Both social isolation and loneliness have been
associated with ill health. Following a recent review
paper of Leigh-Hunt et al (Leigh-Hunt et al., 2017)
there is a strong evidence that both social isolation
and loneliness are associated with increase all-cause
mortality and social isolation with cardiovascular
disease and depression. However, determining
causality is difficult as much of the research in this
area involves observational studies. Concerning these
association the prevention and amelioration of social
isolation and loneliness of adults is becoming an
important topic of policy-makers in various countries
(Dickens et al., 2011).
There are various interventions to prevent and
ameliorate social isolation and loneliness. Based on
the purpose, mechanisms of action and intended
outcomes these interventions can be categorized.
Gardiner et al. (Gardiner et al., 2016) suggests the
following six categories; social facilitation
interventions, psycho-logical therapies, health and
social care provision, animal interventions,
befriending interventions and leisure/skill
development. As well-conducted studies of the
effectiveness of these social interventions for
alleviating social isolation are rare, the evidence
concerning these interventions are indistinctive.
However, following the results of a review of Dickens
142
Jansen-Kosterink, S., Varenbrink, P. and Naafs, A.
The GezelschApp.
DOI: 10.5220/0006732501420147
In Proceedings of the 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2018), pages 142-147
ISBN: 978-989-758-299-8
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
et al (Dickens et al., 2011) it appears there are
common characteristics of effective interventions.
Effective interventions were those developed within
the context of a theoretical basis and those offering
social activity and/or support within a group format.
Next to these two characteristics, interventions in
which older adults are active participants also
appeared more likely to be effective.
In the recent years, there has been an exponential
growth in the use of information communication
technology (ICT) in healthcare. These so called
technology-supported health interventions are widely
evaluated in various target groups (Ekeland et al.,
2010, Kairy et al., 2009) and have the potential to
increase the accessibility to care, to improve the
quality of care and to lower health-care costs
(DeChant et al., 1996). Various papers are published
and addressed the effectiveness of technology-
supported health interventions to reduce social
isolation and loneliness in older adults (Chipps et al.,
2017). ICT can overcome the social and spatial
barriers of social interaction by enabling easy
affordable communication and activities of multiple
form between older adults and others anytime and
anywhere (Chen and Schulz, 2016). Technology-
supported health interventions to reduce social
isolation and loneliness in older adults are divers and
categorized into online activities, interpersonal,
Internet-supported communi-cation and Internet-
supported therapeutics. Older adults can benefit from
technology-supported health interventions and will
use them after proper training (Chen and Schulz,
2016). However, these interventions are not suitable
for all older adults. Therefore, for a positive effect of
these technology-supported health interventions in
reducing social isolation and loneliness tailor-made
interventions and training for the older adult is
necessary.
In the Netherlands a new technology-supported
health intervention to reduce social isolation and
loneliness in older adults is developed and will be
evaluated in the municipality of Enschede. The aim
of this paper is to introduce this new technology, to
provide an overview of the current evaluation and to
present the intermediate results concerning the
usability of end-user acceptance of this technology.
2 METHODS
This paper focusses on a technology supported health
intervention to reduce social isolation and loneliness
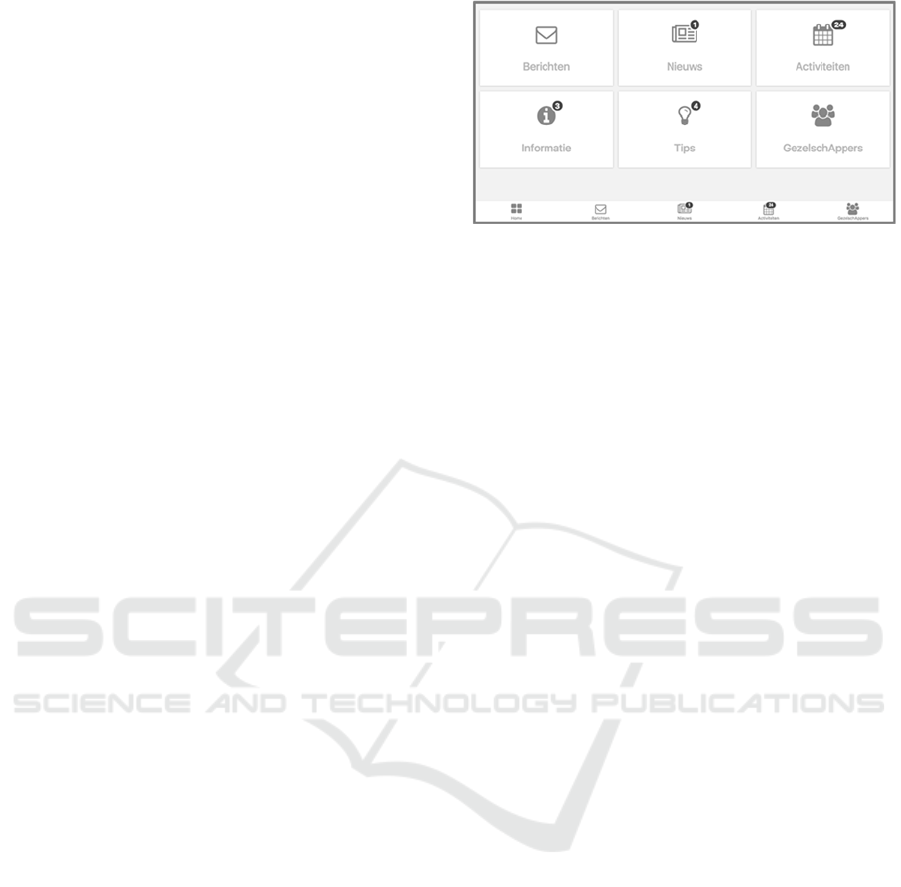
in older adults, named GezelschApp. A merge of the
two Dutch words “Gezelschap” (the most suited
Figure 1: Homepage of the GezelschAPP.
English translation is “company”) and Applicatie
(English translation is “application”). This mobile
application, also accessible by PC and tablet, gives
older adults access to a homepage with six features
(Figure 1). The GezelschApp is developed by 8TING.
The six features of the GezelschApp are an inbox
for messages, news, activities, information, tips and
friends.
- Inbox (“Berichten”): In the inbox users
receive messages concerning the current
news, activities, information, tips and friend
requests. With the inbox users also can send
messages to their friends and their personal
coach.
- News (“Nieuws”): This feature provides the
latest news to the users concerning a healthy
and active lifestyle.
- Activities (“Activiteiten”): The activities in
the neighbourhood of the users are listed
here. All activities in the municipality of
Enschede are digitalized and available
online, there are sport activities, social
activities, education activities, cultural
activities, wellbeing activities, culinary
activities, and other activities suitable for
older adults. Based on the interests of the
user (profile information and user data)
appropriated activities are presented.
- Information (“Informatie”): All kind of
information concerning social activities,
healthy and active aging and the use of the
application is saved here.
- Tips (“Tips”): This feature provides tips to
increase the number of social activities and
social interactions.
- Friends (“GezelschAppers”): All users of
the application are showcased here. The full
contact details of a user are only visible for
their friends and their coach. Users can
become friends by sending and accepting
friend requests. Friends can send each other
messages and invite each other for activities.
The GezelschApp
143

Only screened older adults receive a personal access
code (username and password). After older adults
have shown interest in using the application, a face-
to-face appointment is planned. During this
appointment, a social worker of the local welfare and
wellbeing organisation visits the older adults at home.
After the social worker has made an estimation
whether or not the interested older adult is a suitable
user, the application is introduced to the older adult.
Together the social worker and the older adult create
an user account and profile information as a screen
image, interests and hobbies are added to this
account. During this introduction, the social worker
sends a first friend request to the older adult. This
request needs to be accepted by the older adult as this
social worker will during the use of the application,
coach the older adults to participate in activities and
close (online) friendships.
The application gives the coach the opportunity
based on the profile information and user data to send
personal messages and tips focussing on social
activities, healthy and active ageing and the use of the
application to the users. These messages and tips can
be sent to users personal or as batch to a group of
users. Next to these messages and tips, coaches can
activate users by sending them emails to their
personal email account and text messages to their
mobile phone. On behalf of the users, coaches can
create new activities submitted by the users.
Next to the profile information, the application
provides the coach intelligence on the user use of the
application. In a clear overview, the coach can see
whether a user sends friend request, accepts friend
request or participates in activities. With this
information, the coach can provide tailor-made
coaching to the user with the aim to increase the use
of the application and reduce social isolation and
loneliness. This extra information of the user for
coaches, forces the coach to change their way of
working with social isolated older adults.
There are two main reasons for the developers to
develop the GezelschApp and not use an existing
application to reduce social isolation and loneliness in
older adults, such as Facebook. First, to eliminate
unwanted relationships arising such as preys on
vulnerable and lonely older adults. Therefore, a
secure and save (online) environment was requested.
A non-public application was developed with
imbedded an initial screening contact between the
interested older adults and the social worker of the
local welfare and wellbeing organisation. Second, to
ensure the use of the GezelschApp and to help the
users to participate in activities and close (online)
friendships an active coach was requested. In existing
applications, this role of a coach is not foreseen.
2.1 Participants
Users of the application are during the face-to-face
appointment asked to voluntary participate in the
study to assess the added value of this application for
older adults. Older adults are included when they
experience loneliness, are residents of the
municipality of Enschede, have sufficient
understanding of the Dutch language and are aged
above 60 years. All participants give their informed
consent prior to participation. Concerning sample size
the aim of this cross-sectional cohort study is to
include 75 older adults. The participants are asked to
use the application at least three months.
2.2 Measurements
Considering the maturity of the technology and the
aim of the technology the first evaluation of the
GezelschApp focus on the endpoints: Usability,
acceptance and possible working mechanisms
(DeChant et al., 1996)(Jansen-Kosterink et al., 2016).
During the 3 months evaluation of this application the
usability, end-user acceptance, level of experienced
loneliness and quality of life are assessed. Pre- and
post-test participants are asked to complete
questionnaires to assess the level of experienced
loneliness and quality of life. The questionnaires
concerning usability, end-user acceptance are only
competed by the participants post-test.
2.2.1 Usability
The usability of the application is assessed with the
System Usability Scale (Brooke, 1995). The SUS
presented ten statements about the perceived usability
of the application. Participants could indicate on a 0
to 4 scale to what extent the presented statements
were true for them. To obtain the final SUS score, the
sum of the participants’ answers was multiplied by
2.5. The SUS score ranges from 0 to 100 (low and
high usability, respectively). The English version of
the SUS was translated into Dutch, as there was no
validated Dutch version available.
2.2.2 End-user Acceptance
End-user acceptance of this application was assessed
by means of a questionnaire with summated rating
scales, based upon the Technology Acceptance
Model (TAM) (Davis, 1989). TAM originates from
the 1980s and has been used numerous times to assess
and explain the acceptance of new technology. We
ICT4AWE 2018 - 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health
144

expanded TAM with factors that have been found to
shape the user experience of mHealth technology:
Enjoyment (Crutzen et al., 2011), aesthetics (Baumel
and Muench, 2016), control (Hawkins et al., 2010),
and trust in the technology (Van Velsen et al., 2016).
We hypothesize that these factors affect the core
factors of TAM that explain the intention to use
(perceived usefulness and ease of use).
2.2.3 Loneliness
The De Jong Gierveld loneliness scale (DJGLS) is
frequently used and developed in the mid-1980s in
the Netherlands (de Jong-Gierveld and Kamphuls,
1985). The DJGLS is composed of eleven items, six
negatively formulated and five positively formulated,
with the three response categories (“no,” “more or
less,” and “yes”). The total scale score is the sum of
the item scores, ranging from 0 (not lonely) to 11
(extremely lonely). A score of three or higher is an
indication of loneliness (van Tilburg and de Jong
Gierveld, 1999).
2.2.4 Quality of Life
Quality of life is measured by the 12-item Short Form
questionnaire version 1 (SF-12v1) (Ware et al.,
1996). The SF-12 is a generic instrument including 12
items measuring health related quality of life
(HRQoL). Six items are summed into a physical
component summary (PCS) and six items are
summed into a mental component summary (MCS).
The total score for both scales ranges from 0 to 100,
with a higher number indicating higher quality of life.
2.2.5 Focus Groups
Next to the quantitative data, qualitative data
concerning the added value of this application for
older adults are collected during focus groups. These
focus groups with 6-10 users of the application are
planned at the end of the intervention period of three
months. Next to these focus groups, one focus group
was organized at the beginning of the intervention
period to assess the preliminary experience of the
participants with the application.
2.3 Data Analysis
All outcome measures will be inspected for normal
distribution of data using corresponding histogram
plots including normal curves and normal probability
plots prior to selection of appropriate statistical tests.
Descriptive statistical methods will be applied for
each of the outcome measures (demographic
characteristics, usability, end-user acceptance, level
of experienced loneliness and quality of life).
Presentation of data will be done by calculation of
mean ± standard deviation (SD), or median with
range. To assess the improvement level of
experienced loneliness and quality of life (pre-test
versus post-test) a paired student t-test will be
performed or its non-parametric equivalent. For
statistical analysis, the level for significance will be
set at α < 0.05.
3 RESULTS
The evaluation of the GezelschApp started summer
2017 and is still ongoing. Until the beginning to
December 2017 users of the application will be asked
to participate in this study. Therefore all pre-test
assessed will be finished in the first week of
December. The post-test assessments are planned in
the last week of February 2018. For this reason, the
results that can be present in this paper are limited to
preliminary results and therefore focus on the
demographic of the current participants of the study
and the outcome of the first focus group.
3.1 Participants
At this moment, (November 2017) 23 users (2 male
and 21 female) were willing to participate in this
study. All participants met the predefined inclusion
criteria. The mean age was 72,9 years (range 60-91).
Concerning the living situation, 17% of the
participants are living together with a partner or
spouse and 83% of the participants are living alone.
All participants are community-dwelling older adults
and were retired or un-employed.
3.2 Experienced Loneliness
All participants (n=23) complete the De Jong
Gierveld loneliness scale. The average score on this
scale was 4,9 (SD 3,7). This score correspondents to
moderate loneliness. Focussing on the subscales of
the DJGLS pre-test the participants score on average
3,3 (SD 2,2) on the emotional loneliness subscale
(maximum score is 6) and 1,6 (SD 1,9) on the social
loneliness subscale (maximum score is 5). Focus on
the individual date 30% of the participants experience
no loneliness, 52% of the participants experience
moderate loneliness, 9% of the participants
experience severe loneliness and also 9% experience
very severe loneliness.
The GezelschApp
145
3.3 Results of the First Focus Group
At the end of august 2017, a first focus group was
organized. The aim of the focus group was to assess
the first experience of the users with the application
and to see whether redesign of the application or part
of the application was necessary. In total 10 users (5
male and 5 female) of the application participated in
this focus group. The age of these participants was
between 63 and 80 years old.
Table 1 provides an overview of the positive
points and points for improvement of the application
form the first focus group. Overall, the participants
rate the application with a 6+ [range 4-7]. “I am
positive, a seven, the application is good and of
course the application will improve after this
meeting”.
Table 1: Overview of the general experience with the
GezelschApp.
Positive points
- The development of the application; “as
I am looking for company.”
- Nice and safe way to find new friends.
- I like the tips and possibility to find
information about social activities in my
neighborhood.
- The inbox. “I always visit my inbox, to
see i
f
there are new messa
g
es”
Points for improvement:
- Various technical improvements are
needed (such as deleting messages) to
increase to level of ease of use of the
application.
- Clear guidelines for the set-up of the user
account, similarity in the information of
every user.
- Openness of the users and willingness to
start new friendship by using the
application. “I am a little bit frustrated
about the users that provided just a little
bit of personal information. Maybe they
are afraid, some resistance to open up.”
- More specific information about the
activities.
- The opportunity to create new activities
by the users, without interference of the
coach.
Overall, the participants like the feature to make new
friends the most. This feature was rated as the most
interested feature. On place two of interested features,
was the ability to send and receive messages and on
place three of interested features, was the feature that
provides tips to increase the number of social
activities and social interactions.
4 CONCLUSIONS
Although the evaluation of the technology-supported
health intervention to reduce social isolation and
loneliness in older adults is still running, the first
focus group with users highlight the need of the
current application to make new friends in a save
manner and to participate in social activities. Based
on the outcome of the focus group the application is
improved. As example, the information feature is
changed in a bulletin board feature. This is a more
dynamic feature were coaches can create new
activities as requested by the users. Next to this, the
role of the coach is improved. As the use of the
application demands to change the social worker’s
working methods. The need to be proactive and send
users messages and tips to increase the use of the
application by the users is unusual.
The GezelschApp divers from existing
applications to reduce social isolation and loneliness
in older adults. The GezelschApp is by the initial
screen of the social worker a secure and save (online)
environment. Next to this, an active coach helps the
users to participate in activities and close (online)
friendships. Based on profile information and user
data this coach sends personal messages and tips
focussing on social activities, healthy and active
ageing and the use of the application.
Considering the maturity of the technology and
the aim of the technology the first evaluation of the
GezelschApp focus on the endpoints: Usability,
acceptance and possible working mechanisms. After
this first evaluation, the added value of the
GezelschApp can be accessed within an evaluation
focussing on effectiveness or social impacts.
Considering the uptake of mobile phones by
older adults, mHealth intervention, such as
GezelfschApp, provide opportunities for increased
uptake of technology-supported health interventions
to address and reduce social isolation and loneliness
in older adults.
ICT4AWE 2018 - 4th International Conference on Information and Communication Technologies for Ageing Well and e-Health
146

ACKNOWLEDGEMENTS
Special thanks go to employees and volunteers of
Alifa and the developers of 8TING. The
GezelschApp is part of the 8TING ICT Platform. This
work was funded by the Municipality of Enschede.
REFERENCES
Baumel, A. & Muench, f. 2016. Heuristic Evaluation of
Ehealth Interventions: Establishing Standards That
Relate to the Therapeutic Process Perspective. JMIR
Mental Health, 3, e5.
Brooke, J. 1995. SUS - a quick and dirty usability scale. In:
JORDAN, P. W., THOMA, B. & WEERDMEESTER,
B. A. (eds.) Usability Evaluation in Industry. Lodon:
Taylor & Francis.
Chen, Y. R. & Schulz, P. J. 2016. The Effect of Information
Communication Technology Interventions on
Reducing Social Isolation in the Elderly: A Systematic
Review. J Med Internet Res, 18, e18.
Chipps, J., Jarvis, M. A. & Ramlall, S. 2017. The
effectiveness of e-Interventions on reducing social
isolation in older persons: A systematic review of
systematic reviews. J Telemed Telecare, 23, 817-827.
Crutzen, R., CYR, D. & De Vries, N. K. 2011. Bringing
Loyalty to E-health: Theory Validation Using Three
Internet-Delivered Interventions. Journal of Medical
Internet Research, 13, e73.
Davis, F. D. 1989. Perceived usefulness, perceived ease of
use, and user acceptance of information technology.
MIS Q., 13, 319-340.
De Jong-Gierveld, J. & Kamphuls, F. 1985. The
Development of a Rasch-Type Loneliness Scale.
Applied Psychological Measurement, 9, 289-299.
De Jong Gierveld, J., Van Tilburg, T. & Dykstra, P. A.
2006. Loneliness and Social Isolation. In: Vangelisti,
A. L. & Perlman, D. (eds.) The Cambridge Handbook
of Personal Relationships. Cambridge: Cambridge
University Press.
Dechant, H. K., Tohme, W. G., Mun, S. K., Hayes, W. S. &
SCHULMAN, K. A. 1996. Health systems evaluation
of telemedicine: a staged approach. Telemed J, 2, 303-
12.
Dickens, A. P., Richards, S. H., Greaves, C. J. &
CAMPBELL, J. L. 2011. Interventions targeting social
isolation in older people: a systematic review. BMC
Public Health, 11, 647.
Dykstra, P. A. 2009. Older adult loneliness: myths and
realities. European Journal of Ageing, 6, 91.
Ekeland, A. G., Bowes, A. & Flottorp, S. 2010.
Effectiveness of telemedicine: a systematic review of
reviews. Int J Med Inform, 79, 736-71.
Gardiner, C., Geldenhuys, G. & Gott, M. 2016.
Interventions to reduce social isolation and loneliness
among older people: an integrative review. Health Soc
Care Community.
Hawkins, R. P., Han, J.-Y., Pingree, S., Shaw, B. R., Baker,
T. B. & Roberts, L. J. 2010. Interactivity and presence
of three eHealth interventions. Computers in human
behavior, 26, 1081-1088.
Jansen-Kosterink, S., Vollenbroek-Hutten, M. & Hermens,
H. A renewed framework for the evaluation of
telemedicine. 8th International Conference on eHealth,
Telemedicine, and Social Medicine: eTELEMED (Vol.
2016). 2016 Venice, Italy: .
Kairy, D., Lehoux, P., Vincent, C. & Visintin, M. 2009. A
systematic review of clinical outcomes, clinical
process, healthcare utilization and costs associated with
telerehabilitation. Disabil Rehabil, 31, 427-47.
Leigh-Hunt, N., Bagguley, D., Bash, K., Turner, V.,
Turnbull, S., Valtorta, N. & Caan, W. 2017. An
overview of systematic reviews on the public health
consequences of social isolation and loneliness. Public
Health, 152, 157-171.
Van Tilburg, T. G. & De Jong Gierveld, J. 1999. [Reference
standards for the loneliness scale]. Tijdschr Gerontol
Geriatr, 30, 158-63.
Van Velsen, L., Wildevuur, S., Flierman, I., Van Schooten,
B., Tabak, M. & Hermens, H. 2016. Trust in
telemedicine portals for rehabilitation care: an
exploratory focus group study with patients and
healthcare professionals. BMC Medical Informatics
and Decision Making, 16, 1-12.
Ware, J., Jr., Kosinski, M. & Keller, S. D. 1996. A 12-Item
Short-Form Health Survey: construction of scales and
preliminary tests of reliability and validity. Med Care,
34, 220-33.
The GezelschApp
147
