
“Change the Changeable” Framework
for Implementation Research in Health
Mikiko Oono
1,2
, Yoshifumi Nishida
1,2
, Koji Kitamura
1,2
, Asako Kanezaki
1
,
and Tatsuhiro Yamanaka
3,2
1
Artificial Intelligence Research Center, National Institute of Advanced Industrial Science and Technology, Tokyo, Japan
2
Safe Kids Japan, Tokyo, Japan
3
Ryokuen Children’s Clinic, Kanagawa, Japan
Keywords: Health Education, Active Learning, Participation, Injury Prevention.
Abstract: In recent years, a “participatory” system of community members and researchers has become a key factor to
obtaining the best outcomes to create a better world. The authors previously suggested the problem structure
change theory to find how to address social issues. In this paper, we suggest the “change the changeable
framework” with three approaches for community-based program implementation: 1) Share the value of the
change the changeable, 2) Systematize the process of a problem structure change, and 3) Build a sustainable
system and discuss a case study based on the framework. In the case study, we conducted a safety education
curriculum for injury prevention that consisted of what is injury prevention, playground safety, indoor safety,
and photovoice project. We introduce an injury surveillance system and a risk recognition system as new tools
for the collaboration of human intelligence and artificial intelligence.
1 INTRODUCTION
In recent years, a “participatory” system of
community members and researchers has become a
key factor to obtaining the best outcomes to create a
better world. For example, in the field of service
design, designers have taken a co-design or co-
creation approach to develop new products based on
people’s needs. Co-design is defined as the creativity
of designers and non-designers working together
from the beginning of the development process
(Sanders, 2008). In the field of engineering, a living
lab is a new research approach for making
innovations happen. In living labs, users are involved
in developing, creating, prototyping, validating, and
testing new products, services, or technologies in a
real-life setting (Schuurman, 2011, 2016). In the
public health field, the community-based
participatory research (CBPR) approach has been
widely used to eliminate health disparities. In CBPR,
community members affected by a health issue are
actively involved as a partner in all phases of research
(Minkler, 2004; Wallerstein, 2010).
Co-design, living labs, and CBPR might seem
unrelated, but they use the same approach to reach
their goals. To the authors, it seems that a boundary
between professionals and nonprofessionals has
become unclear in many fields. The key is that all
powers, which include knowledge, skills, and life
experiences that people have regardless of their
expertise, should be recognized and wisely used to
make innovations happen or to find how to address
social issues. In this study, we defined a participatory
system as a group of assets that functions together to
achieve particular goals. The examples of these assets
are not only people who are multidisciplinary
professionals and nonprofessionals, including parents
and children, but also community resources such as
hospitals, schools, and daycare centers.
The authors previously suggested the problem
structure change theory to find how to address social
issues, as shown in Figure 1 (Nishida, 2017). This
theory has three variables: variable A, which is what
we want to change, variable B, which is what we can
change, and variable C, which is what we cannot
change or is difficult to change. Social problems often
seem rigid and unchangeable because they are
discussed based on the relation between variable A
and variable C. By adding operational variable B
(changeable things) to a problem structure, the
structure is transformed to one that can be changed.
Oono, M., Nishida, Y., Kitamura, K., Kanezaki, A. and Yamanaka, T.
“Change the Changeable” Framework for Implementation Research in Health.
DOI: 10.5220/0006691303610368
In Proceedings of the 10th International Conference on Computer Supported Education (CSEDU 2018), pages 361-368
ISBN: 978-989-758-291-2
Copyright
c
2019 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
361

In this paper, we apply this structure to a particular
social issue, which is improving people’s health by
preventing injuries.
Figure 1: Problem structure change theory.
From the perspective of the problem structure
change theory, co-design, living lab, and CBPR fields
face unique limitations for addressing social issues.
In the field of co-design and living labs, B variables
are often already fixed in the first place because most
professional people are knowledgeable about the
latest technologies. Their primary interest is to
implement such technologies, but they often lack an
impact evaluation of how a society changes after the
technology is implemented in a community. On the
other hand, in the field of CBPR, public health
professionals always start with health issues, which
are the A variables (things to be changed), and they
try to translate what science says about appropriate
behaviours through education. In comparison with
engineers, health professionals are generally not
eager to apply new technologies, such as artificial
intelligence (AI) and the Internet of Things (IoT), and
they tend to practice health education in the
traditional way. It seems that researchers in co-design,
living lab, and CBPR fields have suffered from the A-
C structure on the left side of Figure 1 to obtain
ultimate outcomes.
To change the A-C structure, it is necessary 1) to
identify all the possible B variables and to understand
a precise problem structure by collaborating with
people across many different fields, and more
importantly, 2) to gain the power of B identification
by community members so that they can sustain a
healthy community by themselves.
Recently, information communication technology
(ICT) in education has rapidly become popular and
advanced. Rodriguez et al. used ICT as a tool for
elementary school education and implemented a
system to create a school network at the national level
in Panama (Rodriguez, 2009). Terton and White
developed a computer-based educational game for
children to promote physical and social engagement
and discussed the benefits of computer-based
educational gaming (Terton, 2014). In addition,
advanced technologies including IoT and AI are
currently available for community-based programs.
Those technologies can be used for changing A-C
structure and empowering community members.
In this paper, we first propose the “change the
changeable” framework by expanding the concept of
“participatory”. We present a children’s health
education project based on the framework. Then, we
discuss how a health problem structure can be
changed from the viewpoint of a sustainable school
system. Finally, we introduce a risk recognition
system that we developed as a future health education
tool.
2 “CHANGE THE
CHANGEABLE” FRAMEWORK
The three-step approach presented in this section
describes how to establish a strong community health
program in one’s community. The conceptual
framework of change the changeable is shown in
Figure 2.
The three steps are as follows:
1. Share the value of the change the changeable
framework with community members.
2. Systematize the process of a problem structure
change.
3. Build a sustainable system.
2.1 Step 1: Share the Value of Change
the Changeable with Community
Members
To change the A-C structure, it is necessary to
identify variable A as a target and possible B
variables through co-designing with community
members and other collaborators from various fields.
In public health, the following are critical for program
implementation: engaging all stakeholders,
developing a trusting relationship, and more
importantly, realizing that all stakeholders have their
own B’s.
In this step, the content-driven approach is key.
Most researchers are very likely to start with data
collection because the data indicate the direction of
their research. However, it is not easy for community
members to experience the value of data, and data
collection is usually a huge burden for a community.
CSEDU 2018 - 10th International Conference on Computer Supported Education
362
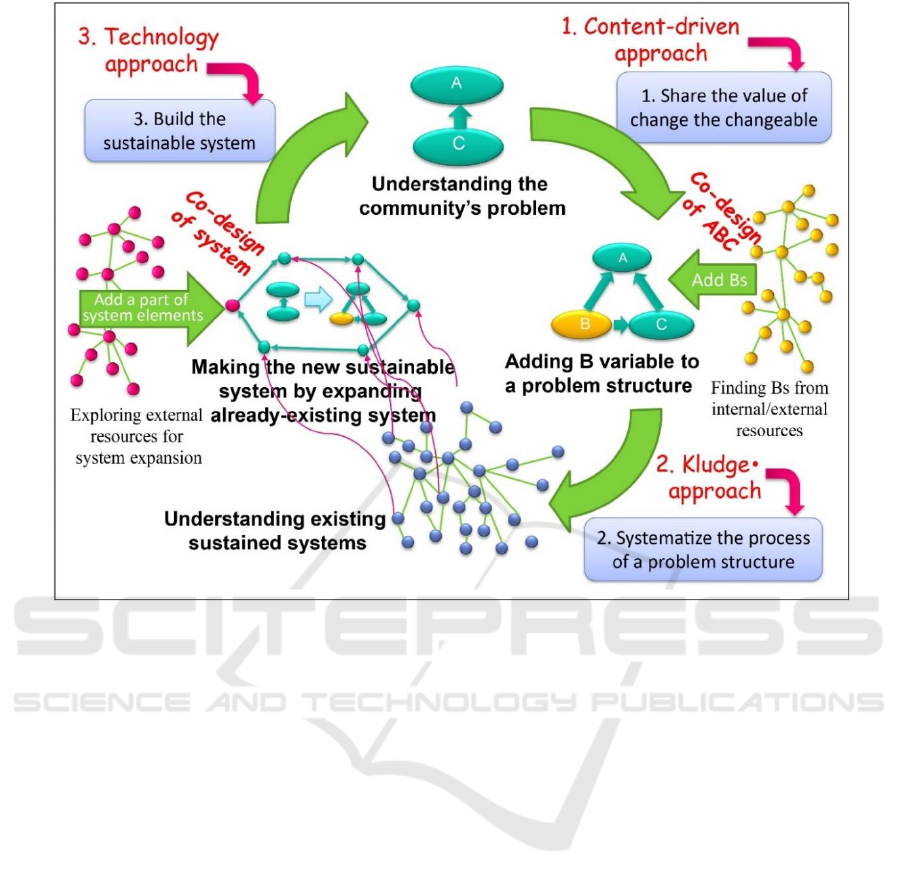
Figure 2: The change the changeable framework using the 1) content-driver approach, 2) kludge approach, and 3) technology-
use approaches.
Therefore, a relatively easy and useful activity,
such as a one-hour workshop or a health education
class, should first be presented so that community
members can learn visible positive outcomes in return
for accepting a small change. Then, they realize
research participation is valuable.
2.2 Step 2: Systematize the Process of
Problem Structure Change
When community members see positive changes for
a particular issue and are ready to make other changes,
it is important to keep and sustain their ability to
change. For example, if community members decide
to implement a health education program at school,
many questions arise: e.g., who provides the classes,
when the program is offered, and who is in charge.
Therefore, step 2 is finding a way to systematize the
process of making changes while developing a
trusting relationship.
Creating a new system from no system or from an
existing system as an independent system is usually
difficult for a community. To overcome such a barrier,
the authors suggest the kludge approach. According
to the dictionary (Dictionary.com, 2017), kludge is
defined as “a software or hardware configuration that,
while inelegant, inefficient, clumsy, or patched
together, succeeds in solving a specific problem or
performing a particular task”. This tells us that it is
important to realize that addressing an issue is a
priority even if the performance is awkward.
Researchers need to find a system that is already
working in a community and expand that system.
Expanding a system could be easier than embedding
a new system in a community.
2.3 Step 3: Build a Sustainable System
When researchers successfully systematize the new
system by expanding the originally existing system, it
is still necessary to strengthen it. To do so,
technologies play a huge role because they can reduce
the task load and maximize the efficiency for work
(the technology-use approach). In reality, however,
many people tend to stay away from new
technologies rather than accept them. If people
understood that technologies can accelerate their
efforts to reach their goal, then they would be more
likely to accept them.
“Change the Changeable” Framework for Implementation Research in Health
363

3 CASE STUDY
In this section, we discuss a case study of injury
prevention education for children and its outcomes,
and then reflect it based on the three steps of the
framework.
3.1 Project Overview: Injury
Prevention Education Curriculum
A comprehensive safety education curriculum was
developed, implemented, and evaluated for 5
th
graders of Fujimidai Elementary School in Tokyo.
This school was certified as the International Safe
School (ISS) in 2016. ISS is a school that carries out
activities to promote school safety and is awarded by
the World Health Organization Collaborating Centre
on Community safety Promotion at the Karolinska
Institutet, Stockholm, Sweden (International Safe
Schools Certifying Centers, 2017). The school’s
teachers, students, and community members
collaborate each other to improve school environment
by identifying B variables and changing the
changeable. The safety education curriculum we
developed consisted of injury prevention
explanations, playground safety, indoor safety, a
photovoice project, and preventive action. Photovoice
is a qualitative community-based participatory
research method using photographs to reflect a
community’s strengths and concerns (Wang, 1997).
From the perspective of problem structure change
theory, B variables can be classified into three
categories, known as the 3E’s: Enforcement,
Environmental modification, and Education. To make
these traditional three E’s of injury prevention more
suitable for school children, we modified them to the
children’s three C’s: Creating rules, Changing the
environment, and Communicating to friends and
family. In the photovoice project, students were asked
to take pictures that showed risks as well as factors
promoting school safety. Then, they wrote how to
reduce the risk and to increase safety based on the
3C’s.
3.2 Health Education Outcomes
Thirty-eight students took the curriculum. Students
presented 27 pictures from the viewpoints of the 3C’s.
As one example of promoting factors, a student took
a picture of a counseling room and said, “The state of
our mind affects injury risk. I feel safe when I consult
a school counselor.” For a risk factor, students
mentioned the risk of a fall by going up the stairs by
skipping every other step and the risk of a crossing
collision in front of a restroom when students run.
Examples of photovoice pictures are shown in Figure
3.
Students also developed a photo R-map (Figure
4). An R-map is a 4×4 matrix that shows risk levels
divided into two levels of frequency of occurrence on
the vertical axis and two levels of injury severity on
the horizontal axis. The R-map is widely used in
engineering fields for risk assessment. Students
placed their pictures based on their opinions about
injury frequency and severity. Sometimes they
relocated the pictures based on class discussion.
Figure 3: Examples of photovoice.
Figure 4: Photo R-map.
During the preventive action time, students
divided into three groups, one for each of the three
C’s, and discussed what they could do to improve
school safety. The first C group created new rules.
The second C group cleaned their classroom in places
where students might trip over an obstacle. Moreover,
for a place that was difficult for the students
CSEDU 2018 - 10th International Conference on Computer Supported Education
364
themselves to modify, they wrote a request letter that
stated where to modify and the reasons behind the
requests. This letter was given to the school principal.
The third C group created educational posters, and
some of them wrote a manuscript for a school
broadcast to promote safety behaviours schoolwide.
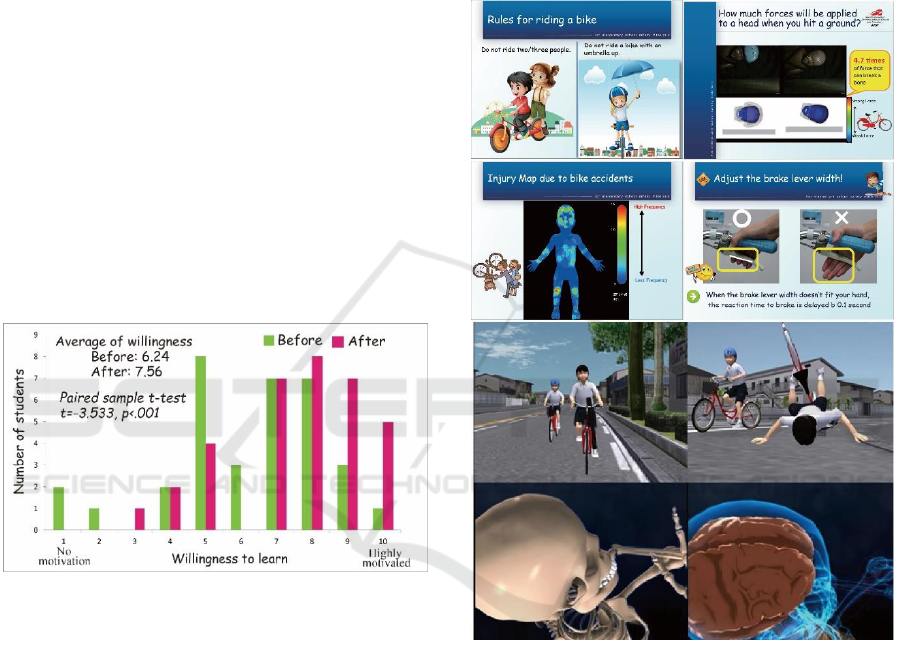
To evaluate the effectiveness of the project, we
conducted a survey asking students if they gained new
knowledge of injury prevention and if the curriculum
raised their willingness to learn more about injury
prevention. The willingness was asked on a scale of
one (low) to ten (high). The Wilcoxon signed-rank
test was used to determine its effectiveness.
The evaluation survey results showed that 91% of
the students said that they gained new knowledge of
injury prevention. As examples of new knowledge,
students stated, “One’s state of mind and
environmental factors cause injury, much more than
what I expected” and “To prevent injuries, it’s critical
to consider one’s behaviours and environmental
conditions around us.” In addition, we found that the
willingness to learn was significantly increased from
6.24 on average to 7.56 (p = .001) (Figure 5).
Figure 5: Changes in students’ willingness to learn.
As a result of sending a request letter to the
principle, a tile floor at the entrance that caused slips
during rainy days was changed to non-slip floor tiles.
3.3 Change the Changeable
Perspectives of the Project
3.3.1 Sharing the Value of Change the
Changeable by using the
Content-Driven Approach
When this project had just started, we recommended
the school to start injury data collection to identify the
school’s injury risk. However, as discussed in
subsection 2.1, it just did not work out. Then we
learned that school teachers were very interested in
science-based tools for injury prevention education
because their expertise is not an injury prevention,
and it is hard for them to gather evidenced-based
injury prevention messages for students. Thus, we
developed educational materials by using our
expertise gave the materials to the teachers. A
snapshot of the materials is shown in Figure 6. By
collaborating with teachers to implement an effective
injury prevention class, we successfully built a
trusting relationship with the school teachers.
Figure 6: Snapshot of the class materials.
3.3.2 Systematization of a Problem
Structure Change by using the Kludge
Approach
When we discussed how to start a health education
curriculum, we found out that a unit for injury
prevention was required as a part of the health and
physical education (PE) curriculum for 5
th
graders.
Thus, we integrated the curriculum into the existing
PE class and taught it over a five-week period. The
PE teacher was in charge of playground safety, indoor
safety, and a part of the photovoice project, and we
took responsibility for an explanation of injury
prevention, the photovoice presentation, and the
“Change the Changeable” Framework for Implementation Research in Health
365
prevention action time. By integrating our education
system into the existing school curriculum system,
our developed injury prevention course has become a
required unit for 5
th
graders at Fujimidai Elementary
School.
3.3.3 Building the Sustainable System using
the Technology-Use Approach
One of the huge successes during collaborations for
the injury prevention class was that school teachers
started to understand the meaning of data and to want
to collect injury data at school. As a means of
developing effective and convincing class material
for students, the values of the data outweighed the
time and effort of data collection. This is where
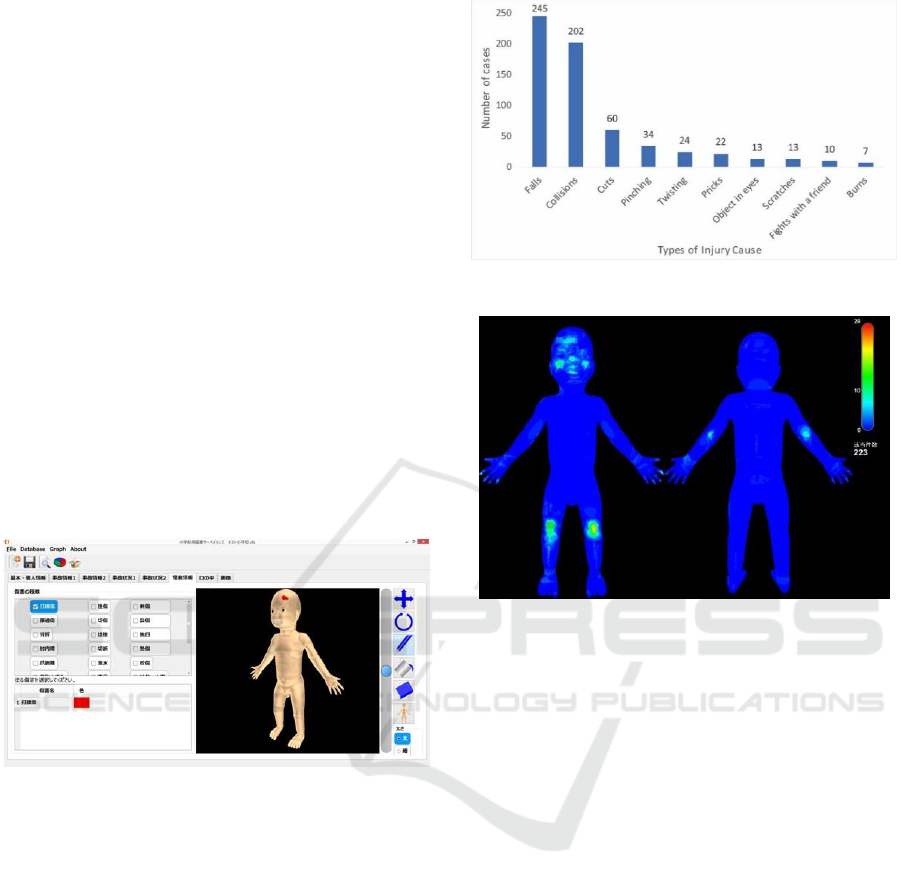
technologies came in. We developed an injury
surveillance system for schools. The system is
capable of collecting, aggregating, analysing, and
searching data of injuries. The system also has a
function called “Body-graphic Information System”
(“BIS”) that enables us to express, collect, retrieve,
and analyse external injury geometric data (Figure 7).
Figure 7: Injury surveillance software.
The injury education project has been conducted
since 2013, and Fujimidai Elementary School decided
to use the surveillance system at the end of their
school fiscal year. Between April 2014 and March
2017, 704 instances of injury were collected from the
school. As of April 3
rd
, 2017, the total number of
students enrolled in Fujimidai Elementary School was
302 children. As shown in Figure 8, the number one
cause of injury was falls (245 cases) followed by
collisions (202 cases), cuts (60 cases), and pinching
(34 cases).
Figure 9 shows the body parts that were injured
due to falls. A red area indicates a high frequency of
injury. The analysed data were integrated into the
health education class and helped students recognize
their own school’s problems.
Figure 8: Types of injury.
Figure 9: Fall injury analysis using BIS.
Moreover, we developed an injury recognition
system by using pictures of the photovoice project.
The system is based on the convolutional neural
network (CNN)-based model “RotationNet”
(Kanezaki, 2016; Savva, 2017). The system takes
multi-view images of an object as input and estimates
both the object’s pose and category. The method
treats the pose labels as latent variables, which are
optimized to self-align in an unsupervised manner
during training with an unaligned dataset.
Figure 10 shows the result of stair recognition.
The system automatically extracts view features (top
photo), and then chooses a specific viewpoint based
on the scores of the predicted category. Once the
system recognizes an object, it indicates possible
injuries that commonly occur in and around the
recognized object (bottom photo). Students used this
recognition system to discuss what preventive actions
can be taken to avoid injuries.
CSEDU 2018 - 10th International Conference on Computer Supported Education
366

Figure 10: Output of the risk recognition system.
4 DISCUSSION
Change the changeable framework suggested a way
of bridging the gap between community members and
researchers. Using three steps with three approaches
is critical to establishing a sustainable system. A
sustainable system combines the power that
community members have and the knowledge and
skills from external resources, and does not proceed
with the project based only on the researchers’
intentions. As in the definition of kludge, even though
researchers think that the way of proceeding on the
project may seem inefficient, ineffective, or clumsy,
whatever action acceptable to community members is
most important because this is how community
members keep participating in a project.
Moreover, carrying out the project according to
the community members’ desires helps them to enjoy
changing the changeable, and this is an invaluable
outcome for community-based programs. As
emphasized in subsection 2.1, starting with data
collection to develop a community-based
participatory system usually does not work.
Researchers need to convince community members
that starting a project is actually valuable to them even
though they need to undertake some tasks. So far, the
authors have successfully implemented community-
based health education programs at five schools,
including a middle school, by using the change the
changeable framework. In addition, community-wide
injury surveillances were started in two cities.
Our developed injury surveillance system and risk
recognition system helps people learn the injury risks
around them. Injury data collected from the
surveillance system (BIS) are integrated into class
material development to promote student learning
after the system was installed. Understanding injuries
occurred in their school using BIS and predicting
plausible injuries using the AI-based recognition
system brings home the fact that injuries can actually
occur to them. Injury data localization based on the
technologies is powerful to heighten the perception of
injury susceptibility. We developed these systems to
promote interactions between human intelligence and
artificial intelligence. Utilization of these systems is
one example of future injury education tools that will
connect people and people, communities and
communities, people and knowledge, and problems
and solutions.
5 CONCLUSIONS
We suggested the change the changeable framework
and discussed a health education program based on
the framework. Our previous experience of
implementing a community-based health program
showed three useful approaches for program
implementation: 1) content-driven approach, 2)
kludge approach, and 3) technology-use approach.
We conducted a case study of an injury prevention
education project that consisted of classroom lectures
and a photovoice project. During the photovoice
presentation class, students presented 27 pictures
from the viewpoints of the children’s 3C’s (Creating
rules, Changing the environment, and
Communicating to friends and family). They also
created photo R-maps using their photovoice pictures.
The project’s evaluation survey indicated that the
students’ willingness to learn about injury prevention
was significantly increased.
We hope that the change the changeable
framework will be applied to various community-
based programs and expand our knowledge of
implementation science.
ACKNOWLEDGEMENTS
This research is supported by the Strategic Basic
Research Program (CREST) from Japan Science and
Technology Agency, JST.
“Change the Changeable” Framework for Implementation Research in Health
367

REFERENCES
Dictionary.com., 2017. Definitions: kledge (Accessed 23
October 2017). Available from:
http://www.dictionary.com/browse/kludge.
International Safe Schools Certifying Centers., 2017.
History (Accessed 25 December 2017). Available from:
http://internationalsafeschool.com/history.html.
Kanezaki A., Matsushita Y., Nishida Y., 2016. Rotationnet:
Joint learning of object classification and viewpoint
estimation using un-aligned 3D object dataset. arXiv
preprint arXiv:1603.06208.
Minkler, M., 2004. Ethical challenges for the “outside”
research in community-based participatory research.
Health education & behavior. Vol.31, No.6, pp.684-
697.
Nishida, Y., Kitamura, K., Oono, M., Tamanaka, T., 2017.
Smart transfer of social problem into industry by linking
living data center with social function library: Case
study of toothbrush injury prevention. In Proc. Of 3
rd
IEEE annual international smart cities conference
(ISC2 2017).
Rodríguez, MA., Barrios, JDC, Schultz, ES., 2009. The use
of an innovation classroom: a perspective in the
introduction of ICT in elementary schools, In
Proceedings of the First International Conference on
Computer Supported Education, Vol.1, pp.173-180.
Sanders E.B.N., Stappers, P.J., 2008. Co-creation and new
landscapes of design. CoDesign, Vol.4, No.1, pp.8-19.
Savva, M., Yu, F., Su, H., Kanezaki, A., Furuya, T.,
Ohbuchi, R., et al., 2017. SHREC’17 Track Large-scale
3D share retrieval from ShapeNet Core55. (Accessed 23
October 2017). Available from:
https://shapenet.cs.stanford.edu/shrec17/shrec17shapen
et.pdf.
Schuurman, D., De Marez, L., Ballon, P., 2016. The impact
of living labs methodology on open innovation
contributions and outcomes. Technology Innovation
Management Review. Vol.6, No.1, pp.7-16.
Schuurman D. De Moor, K., De Marez, L., Evens T., 2011.
A living lab research approach for mobile TV.
Telematics and Informatics Vol.28, No.4, pp.271-282.
Terton, U., White, I., 2014. A computer-based educational
adventure challenging children to interact with the
natural environment through physical exploration and
experimentation. CSEDU 2014 In Proceedings of the 6
th
International Conference on Computer Supported
Education, Vol.3, pp.93-98.
Wallerstein, N., Duran, B., 2010. Community-based
participatory research contributions to intervention
research: the intersection of science and practice to
improve health equity. American Journal of public
health Vol.100 Suppl.1, pp.S40-46.
Wang, C. , Burris, M.A., 1997. Photovoice: concept,
methodology, use for participatory needs assessment.
Health education & behaviors, Vol.24, No.3, pp.369-
387.
CSEDU 2018 - 10th International Conference on Computer Supported Education
368
