
The Relationship between Exhaled Carbon Monoxide Test and Peak
Expiratory Flow Rate in Smokers and Non-smokers
N. N. Soeroso
1*
, T. K. Intan
2
, M. Ichwan
3
, S. P. Tarigan
1
and A. S. Wahyuni
4
1
Department of Pulmonology and Respiratory Medicine, Faculty of Medicine, Universitas Sumatera Utara,
Universitas Sumatera Utara Hospital, Jl. Dr. Mansyur No. 66 Medan 20154, Sumatera Utara, Indonesia
2
Department of Anatomy Pathology, Faculty of Medicine, Universitas Sumatera Utara,
Jl. Dr. Mansyur No. 5 Medan 20155, Sumatera Utara, Indonesia
3
Department of Pharmacology, Faculty of Medicine, Universitas Sumatera Utara,
Jl. Dr. Mansyur No. 5 Medan 20155, Sumatera Utara, Indonesia
4
Department of Community Medicine, Faculty of Medicine, Universitas Sumatera Utara,
Jl. Dr. Mansyur No. 5 Medan 20155, Sumatera Utara, Indonesia
Keywords: Carbon Monoxide, Exhaled Carbon Monoxide Test, Peak Expiratory Flow, Smoker, Non-smokers.
Abstract: Cigarettes are one of the health problems in the community with an estimated 5 million people die every year.
CO concentration in expiratory air is a reliable indicator of blood COHb levels. Aim of this study is to
investigate the relationship between exhaled carbon monoxide test and PEFR in smokers and non-smokers.
Design of this study was a cross-sectional. Fourty one subjects who were recruited by a consecutive sampling
technique. The measurement of nicotine dependence rate was conducted by using Fagerstrom Tolerance
Questionnaire (mFTQ). The expiratory CO levels were examined using piCO Smokerlyzer. Statistical
analysis was done with logistic regression test and Spearman’s correlation test by using software EpiInfo 7.0.
Patients who had a risk of decreasing PEFR was found in men, aged >30 years, worked as an employee or
entrepreneur, smokers, and had an expiratory CO level >5 ppm (p<0.05). It is also found that the higher CO
levels in the body, the lower the percentage of an individual’s PEFR; however, this correlation was not
statistically significant. Furthermore, there was a significant relationship between sex, age, occupation,
smoking status, and CO levels with PEFR values.
1 INTRODUCTION
Cigarettes are one of the causes of public health
problems with an estimated mortality of 5 million
people every year (WHO, 2006). More than 3000
journals and research published since the 1970s have
shown the dangers of smoking to human health.
Ironically, since 1998 to date, Indonesia still occupies
the fifth rank for the most cigarette consumption and
the third largest number of smokers in the world. The
number of smokers in Indonesia continues to increase
in line with an increasing population (Achadi,
Soerojo & Barber, 2005).
WHO reported that 15 billion cigarettes are
consumed every year. A WHO report in 2011
mentioned that China was listed as a country with the
most cigarette consumption in the world (WHO,
2011). On the other hand, data in Indonesia showed
that 67% of men were smokers, and 57% of them
were daily smokers. The highest percentage of female
smokers in the world was recorded in Nauru (50%)
and Austria (48%) (WHO, 2015).
The most widely known components of cigarette
smoke are tar, nicotine, carbon monoxide (CO), and
other substances (Hoffman, 2001). When cigarette
smoke passes through the airways, 4000 chemical
substances including carbon monoxide will be
absorbed through the lungs, will enter the
bloodstream, and will bind to hemoglobin to form
carboxyhemoglobin (COHb) in which its levels in the
blood can be measured as an absorption marker of
cigarette smoke (Kumar, 2010; Kendrick, 2010). CO
concentration in expiratory air is a reliable indicator
of blood CoHb levels (Jarvis, 1986). The purpose of
this study was to investigate the relationship between
expiratory air CO and APE in healthy smokers and
non-smokers.
Soeroso, N., Intan, T., Ichwan, M., Tarigan, S. and Wahyuni, A.
The Relationship between Exhaled Carbon Monoxide Test and Peak Expiratory Flow Rate in Smokers and Non-smokers.
DOI: 10.5220/0010081306350638
In Proceedings of the International Conference of Science, Technology, Engineering, Environmental and Ramification Researches (ICOSTEERR 2018) - Research in Industry 4.0, pages
635-638
ISBN: 978-989-758-449-7
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
635
2 METHODS
Subjects of this research were 41 subjects consisting
of smokers and non-smokers and aged >20 years. The
smoking status was documented through interviews.
An individual is categorized as an active smoker if he
has a smoking history of ≥100 cigarettes throughout
his life (Ryan, 2012). Merc Phillips Respironics was
used to examine the Peak Expiratory Flow Rate
(PEFR). The interpretation used Pneumobile Project
table. piCO Smokerlyzer was used to examine
exhaled carbonmonoxide test and the interpretation
used smokerlyzer® chart.
Data analysis of the relationship between CO
levels and PEFR in healthy smokers and non-smokers
used the Spearman’s correlation test. On the other
hand, factors influencing PEFR was analyzed with a
logistic regression test. Data were analyzed using Epi
Info software. This study used an informed consent
and was approved by the Health Ethics Commission.
3 RESULTS
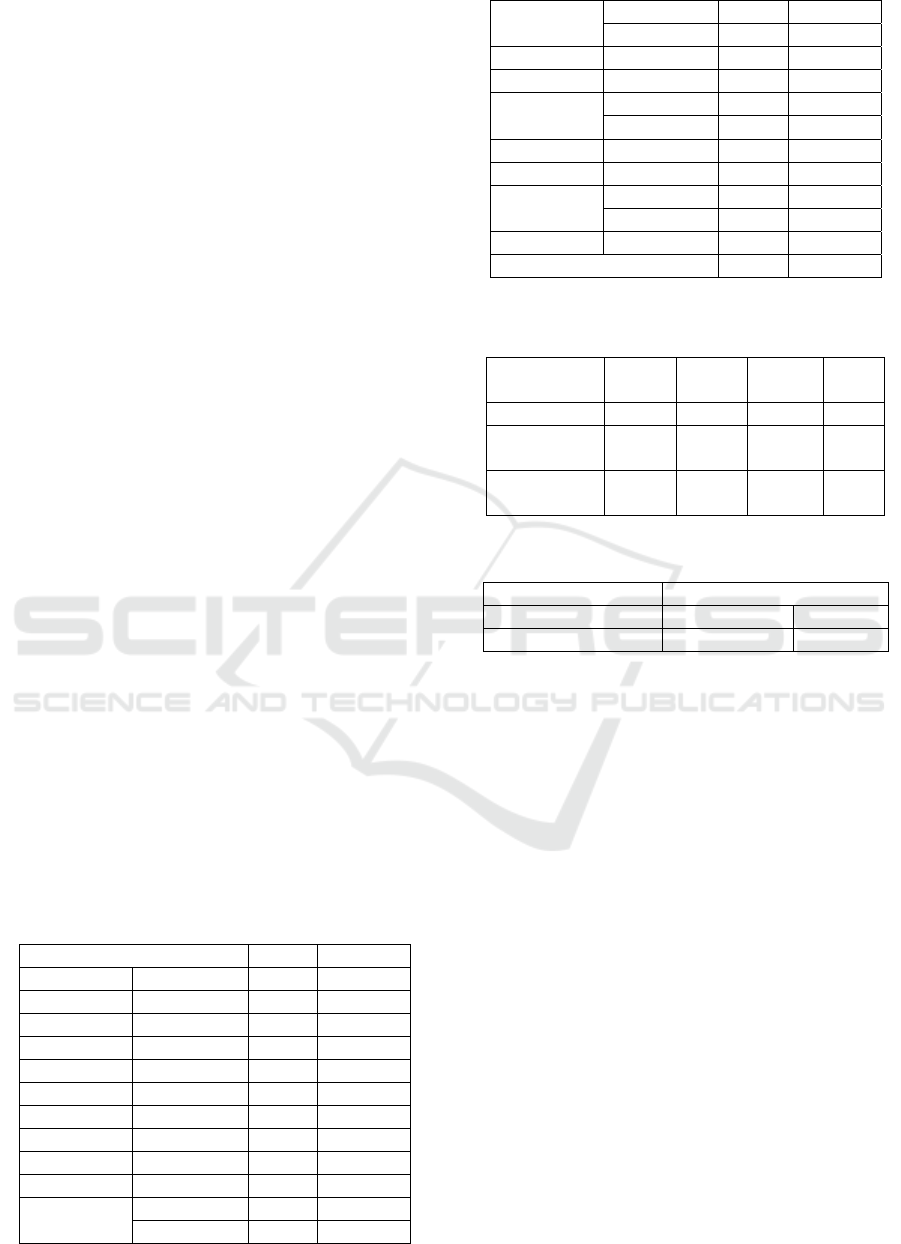
As shown in Table 1, the results showed that men
were most often found in the study with
approximately 63.4%, aged ≤30 years was around
46.3%, and smokers was around 51.2%. The PEFR
examination results with the value of 251-500 was
about 51.2%. Table 2 shows the correlation between
CO levels and PEFR in which the higher CO levels in
the body, the lower the percentage of an individual’s
PEFR although this result was not statistically
significant. Table 4 shows a significant relationship
between sex, age, occupation, smoking status, and
CO levels with PEFR values. Patients who had a risk
of decreasing PEFR were male, aged above 30 years
old, worked as an employee or an entrepreneur,
smoker, and CO level was more than 5.
Table 1: Characteristics of subjects
Variable n %
Sex Male 26 63.4
Female 15 36.6
Age ≤30 years 19 46.3
31-40 13 31.7
41-50 2 4.9
51-60 2 4.9
>60 5 12.2
Occupation Student 19 46.3
Employee 5 12.2
Entrepreneur 17 41.5
Smoking
status
Smoker 21 51.2
Non-smoker 20 48.8
CO level
(ppm)
0-5 23 56.1
6-10 10 24.4
11-20 3 7.3
>20 5 12.2
PEFR
percentage
0-29.9 % 0 0.0
30-59.9%
5 12.2
60-79.9 % 13 31.7
≥80% 23 56.1
PEFR
values
0-250 7 17.1
251-500 21 51.2
>500 13 31.7
Total 41 100.0
Table 2: Correlation between CO and PEFR
Mean
SD Median
Min-
Max
CO level 8.34 8.7 5 2-35
PEFR
percentage 76.2
15.8
80
34.5-
120
PEFR values 403.7
127.2 370
180-
600
Table 3: PEFR Percentage
PEFR Percentage
p-value r
Kadar CO 0.106 -0.26
Spearman’s Correlation test
4 DISCUSSION
According to Riskesdas in 2010, the highest
percentage of smokers was found in the age group of
45-54 years with 38.2%, followed by the age group of
25-34 years (Riskesdas, 2010). In this study, the
dominant age was <30 years with 46.3%. The
findings of this study indicate a significant
relationship between sex, age, occupation, smoking
status, and CO levels with PEFR values. Based on the
existing literature, age can affect the absorption
process and CO elimination through the diffusion
path barrier in the lungs. Thus, the addition of age will
make the air barrier in the lungs become.
The recommendation of the European Respiratory
Society (ERS) consensus stated that expiratory CO
levels in non-smokers were <4 ppm (Tonnesen,
2007). The results of the present study were also in
accordance with the study of (Middleton, 2000)
which determined CO ≤6 ppm as the limit for non-
smokers
ICOSTEERR 2018 - International Conference of Science, Technology, Engineering, Environmental and Ramification Researches
636
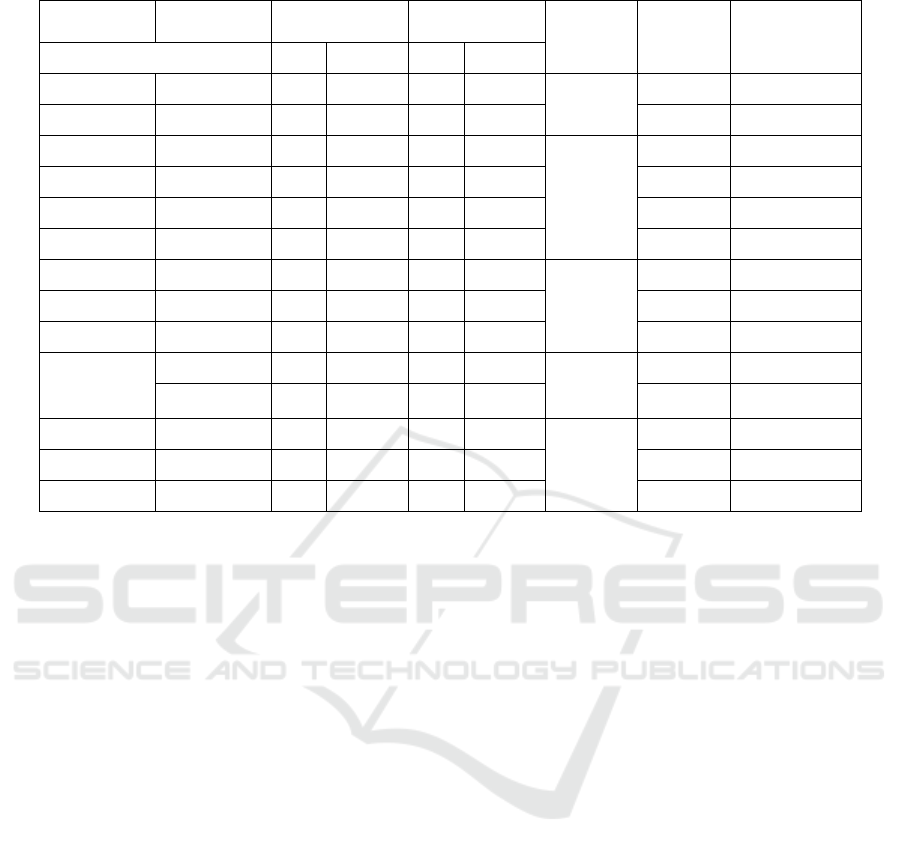
Table 4: Factors influencing PEFR
(Middleton, 2000). The literature stated that the daily
number of cigarettes consumed can affect the
expiratory CO levels in smokers with estimated CO
levels of 15-34 ppm if smoking 20 cigarettes/day
which will increase to 25-60 ppm if smoking 40
cigarettes/day (Kendrick, 2010).
5 CONCLUSIONS
The study found that the higher the CO levels in the
body, the lower the percentage of a person’s PEFR;
however, it was not statistically significant. The
expiratory air CO levels in smokers were higher than
non-smokers. Patients who had a risk of decreasing
PEFR were found in male smokers aged above 30
years old who had expiratory CO levels greater than
5 ppm. However, the study had a limitation, namely
the lack of sample size.
FUNDING AND CONFLICT OF
INTERESTS
The authors received funding from TALENTA
research program of University of Sumatera Utara.
REFERENCES
Achadi A, Soerojo W & Barber S. The relevance and
prospects of advancing tobacco control in Indonesia.
Health Policy 2005;73(3):333-349.
Hoffman D, Hoffman I & El-Bayoumy K. The less harmfull
cigarette: a controversial issue. Chem Res Toxicol
2001;14(7):767-790.
Jarvis MJ, Belcher M, Vesey C, Hutchison DCS. Low cost
carbon monoxide monitors in smoking assessment.
Thorax 1986;41:886-7.
Kementerian Kesehatan RI. Riset Kesehatan Dasar :
RISKESDAS 2010. Badan Penelitian dan
Pengembangan Kesehatan. 2010.
Kendrick AH. Exhaled Carbon Monoxide Devices in
Smoking Cessation : Physiology, Controversies and
Equipment. The Buyers Guide to Respiratory Care
Product. [Online]. 2010 [cited 2010 April 11];
Available from: URL:http//
www.dev.ersnet.org/uploads/Document/e1/
WEB_CHEMIN_2567_1194523664.pdf.
Kumar R, Prakash S, Kushwah AS, Vijayan VK. Breath
Carbon Monoxide Concentration in Cigarette and Bidi
Smokers in India. The Indian Journal of Chest Diseases
& Allied Sciences 2010;52:19-24.
Middleton ET, Sci BM, Morice AH. Breath Carbon
Monoxide as an Indication of Smoking Habit. Chest
2000;117:758-63.
Ryan H, Trosclair A, Gfroerer J. Adult current smoking:
Differences in definitions and prevalence estimates-
Normal PEFR
(
≥80%
)
Low
PEFR
(
<80%
)
p-value OR 95%CI
n % n %
Sex Male
11 47.8
15 83.3
0.02
1 1
Female
12 52.2
3 16.7
0.18 0.04 - 0.80
A
g
e ≤30
y
ears
14 60.9
5 27.8
0.03
1 1
31-40
7 30.4
6 33.3
2.4 0.53 - 10.6
41-60
2 8.7
2 11.1
2.8 0.3 - 25.5
>60
0 0.0
5 27.8
NA NA
Occupation Student
15 65.2
4 22.2
0.01
1 1
Em
p
lo
y
ee
3 13.0
2 11.1
2.5 0.3 - 20.4
Entre
p
reneu
r
5 21.7
12 66.7
8.9 1.9 - 41.0
Smoking
status
Non-smoke
r
15 65.2
5 27.8
0.01
1 1
Smoke
r
8 34.8
13 72.2
4.8 1.27 - 18.6
CO level 0-5
17 73.9
6 33.3
0.01
1 1
6-10
2 8.7
8 44.4
11.3 1.8 - 69.07
>20
4 17.4
4 22.2
2.83 0.53-15.04
The Relationship between Exhaled Carbon Monoxide Test and Peak Expiratory Flow Rate in Smokers and Non-smokers
637

NHIS and NSDUH 2008. J Environ Public Health
2012:1-11.
Tonnesen P, Carrozzi L, Fagerstrom KO, Gralziou C, Ruiz
CJ, Nardini S, et al. Smoking cessation in patients with
respiratory diseases: a high priority integral component
of therapy. Eur Respir J 2007;29:390-417.
World Health Organization: The Facts About Smoking
and Health, May 30, 2006. Available from:
http://www.wpro.who.int/media_centre/fact_sheets/fs_
20060530.htm
World Health Organization 2011,’The Millenium
development goals for health’. viewed 01 December
2013 http://un.orgmdg-report-2011-english
World Health Organization 2015, ‘Cancer Control : A
Global snapshot in 2015’, viewed 2016,
www.who.int/cancer/cancer-snapshot-2015/en/
ICOSTEERR 2018 - International Conference of Science, Technology, Engineering, Environmental and Ramification Researches
638
