
Comparison of Ureum Plasma Level between Controlled Type 2
Diabetes Mellitus and Uncontrolled Type 2 Diabetes Mellitus
Maya Savira
1*
, Rusdiana
2
, Sry Suryani Widjaja
2
, M. Syahputra
2
1
Departement of Physiology,Medical Faculty, Universitas Sumatera Utara, Jl. dr. Mansur no.5, Medan, Indonesia
2
Departement of Biochemistry, Medical Faculty, Universitas Sumatera Utara, Jl. dr. Mansur no.5, Medan, Indonesia
Keywords Diabetes Mellitus, Type 2 Diabetes Mellitus, Ureum, Ureum Plasma
Abstract Diabetes mellitus is characterized by chronic hyperglycemia, Diabetes mellitus is associated with absolute or
relative deficiencies in insulin secretion, insulin action or both. Diabetic nephropathy occur in approximately
in one third type 2 diabetic patients which are uncontrolled. In diabetic nephropathy, bio-markers such as
serum urea and creatinine are known to be raised with hyperglycemia and usually correlate with severity of
kidney damage. Urea and creatinine are good indicators of a normal functioning kidney and increase in the
serum are indications of kidney dysfunction. Objective of this study is to compare ureum plasma level between
controlled type 2 diabetes mellitus (CT2DM) and uncontrolled type 2 diabetes mellitus (UCT2DM). This
study is descriptive analytic research method with across-sectional design. It involved 40 patients, sample
population is all of type 2 diabetic patients in the Primary Health Care in Binjai city of North Sumatera
Indonesia in accordance with the inclusion criteria. Subjects devided into two groups each group consisted of
20subjects the two groups are UCT2DM patients and CT2DM. Estimation of ureum level was done by the
modified Berthelot’s method with spectrophotometry. t-test was used to compare the ureum level. The
average ureum level of the UCT2DM patients is 28.05 mg/dl, the CT2DM patients is 27.58 mg/dl. This study
showed that there was significant difference between CT2DM and UCT2DM (p<0.005). This findings
showed that good control of blood glucose level is absolute requirement to prevent progressive renal
impairment.
1 INTRODUCTION
Diabetes mellitus (DM) is classified based on chronic
hyperglycemia the increasing of blood glucose level
that is caused by missarrengement in metabolism of
fat, carbohydrate, and protein. DM is connected
relatively or absolutely with decreasing in insulin
secretion or/ and insulin action (Kanwar et al., 2015).
DM affects above 170 million people in the world and
keep increasing up to 370 million in 2030 according
to the World Health Organization (WHO) (Wild et
al.,2004., Mehta , 2006). At the present time, around
217 million people live with DM, above 350 million
people will live in that condition by 2030 (Smyth and
Heron, 2006., Yach et al.,2006). The data from
regional International Diabetes Federation (IDF)
demontrates that Southeast Asia ranked second in the
world 3 and the number of diabetics in Indonesia was
ranked seventh in the world in 2013 (Riskesdas ,
2013).
Type 1 diabetes mellitus (T1DM)and type 2
diabetes mellitus (T2DM) are clear diseases due to
either disfunction of pancreatic to synthesize insulin
or ineffectiveness of insulin maintaining blood
glucose level that is still in the physiologic range
(Karla , 2012).
The risk factors for T2DM are obesity,
poor diet, sedentary lifestyle, increased age, family
history and metabolic syndrome (Kasper et al., 2005).
Diabetic nephropathy occur on the order of one third
T2DM patients which are uncontrolled (Rehman et
al., 2005). Diabetic nephropathy is classified based on
albuminuria above 300 mg/24-hour urine collection
and disfunction of renal as shown by the increasing of
creatinine serum level and urea serum level. Diabetic
nephropathy Clinically, is diagnosed based on
proteinuria and, decresing of glomerular function rate
(GFR), (Melmed, 2016).
In diabetic nephropathy,
bio-markers like serum urea and creatinine are known
to be increased with hyperglycemia and usually
associate with severity of kidney damage (Melmed,
2016., Zimmet et al., 2001).The good indicators to
determine weather kidney is in normal function are
urea serum level and creatinine serum level. The
Savira, M., Rusdiana, ., Widjaja, S. and Syahputra, M.
Comparison of Ureum Plasma Level between Controlled Type 2 Diabetes Mellitus and Uncontrolled Type 2 Diabetes Mellitus.
DOI: 10.5220/0010077105250527
In Proceedings of the International Conference of Science, Technology, Engineering, Environmental and Ramification Researches (ICOSTEERR 2018) - Research in Industry 4.0, pages
525-527
ISBN: 978-989-758-449-7
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
525
increasing of these serum indicates dysfunction of the
kidney (Kamal, 2014).
Blood tests for Blood Urea
Nitrogen (BUN) which is a major nitrogenous end
product of protein and amino acid catabolism and
creatinine which is a breakdown product of creatine
phosphate in muscle are excreted by kidneys are used
routinely instead of urine analysis whish is
discomforting for patients (Kamal, 2014., Gowda et
al, 2010). The aim of this study is to compare ureum
plasma level between controlled type 2 diabetes
mellitus (CT2DM) and uncontrolled type 2 diabetes
mellitus (UCT2DM).
2 METHODS
This is a descriptive analytic research study with
cross-sectional design. 40 patients included,in this
research consecutive sampling method used to enroll
the subjects, population of the sample is all of the
patients in the Primary Health Care in Binjai city of
North Sumatera Indonesia that is diagnosed as type 2
diabetes mellitus then the subjects divided in to two
groups the first one is the group of UCT2DM 20
subjects and the second one is the group of CT2DM
included 20 subjects, it separated based on clinincal
laboratory test of Hba1c. the value of Hba1c 6.5-8%
was classified as CT2DM and the value of Hba1c >
8% was classified as UCT2DM. The inclusion criteria
were, aged > 40 years old, have a will to join this
research and cooperative and exclusion criteria were,
in the middle of cancer and diuretic therapy.The
approval of this research was obtained from Health
Research Ethical Committee, Medical Faculty of
University Sumatera Utara /H.Adam Malik General
Hospital number 591/TGL/KEPK FK USU-RSUP
HAM 2018. We examined each sample by their
weight, height, abdominal circumstance, blood
pressure,and we did the clinical laboratory tests such
as fasting blood sugar levels and Hba1c and ureum
plasma levels as well by using secondary data, we
estimated the ureum levels by Berthelot’s method
that is modified. We collected plasma using standart
protocol with EDTA then we add urease and
incubated for 20 minutes in 37
0
C then we add reagen
1 and 2, incubated for next 20 minutes in 37
0
C and
we did the spectrophotometry with wavelength
546±548 nm. The measurement of Hba1c was done
in Thamrin clinical laboratory. The informed consent
were given to all subjects. The data were analyzed
using T-Test and p value<0.005 was considered as
significant.
3 RESULT AND DISCUSSION
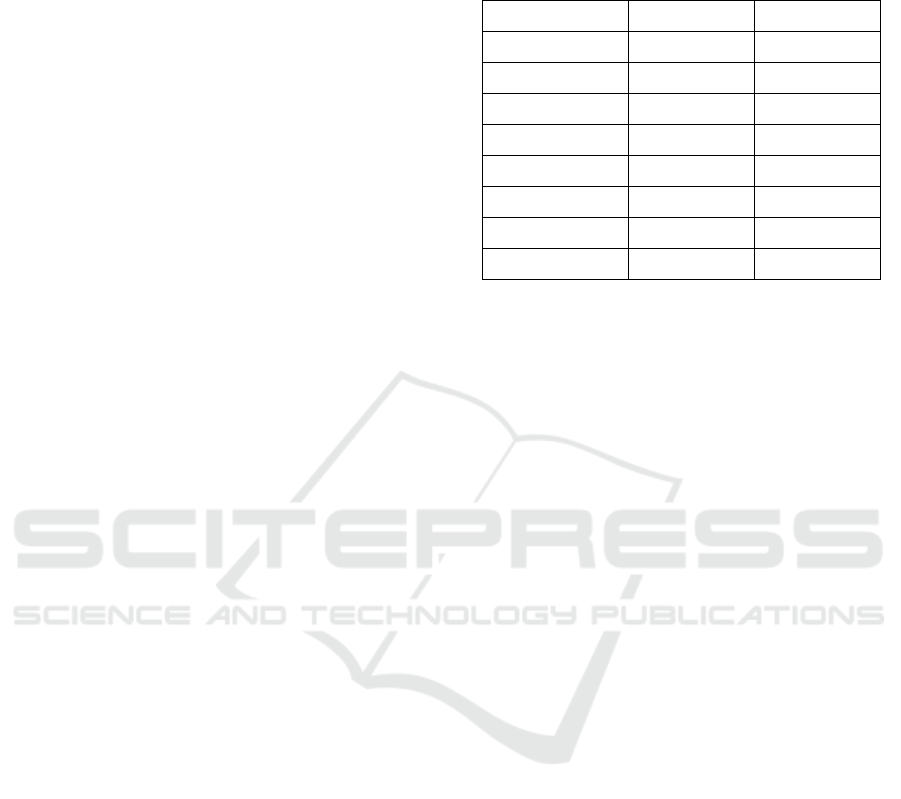
Table 1. Baseline characteristic of 40 subjects.
UCT2DM CT2DM
A
g
e
(y
o
)
56.2±9.2 60.6±7.3
BMI (kg/m2) 26.5±3.5 25.7±4.1
waist size
(
cm
)
92.4±5.2 93.1±9.0
FBS
(
m
g
/dl
)
219.1±92.4 155.6±45.2
Hba1C (%) 9.7±1.0 8.0±1.8
Ureum
(
m
g
/dl
)
28.05±7.45 27.58±7.20
S
y
stole
(
mmH
g)
124.9±18.2 144±30.6
Diatole(mmHg) 77.6±7.3 89.1±17.3
Between 40 patients of T2DM, the male were 30.4%
and the female were 69.6%. Baseline characteristic of
the samples are shown in table 1. In this research the
average age of the uncontrolled T2DM patients is
56.2 years old, the controlled T2DM patients is 60.6
years old. The average BMI of the uncontrolled
T2DM patients is 26.5 kg/m
2
, the controlled T2DM
patients is 25.7 kg/m
2
. The average waist size of the
uncontrolled T2DM patients is 92.4 cm, the
controlled T2DM patients is 93.1cm. The average
FBS of the uncontrolled T2DM patients is 291.1
mg/dl, the controlled T2DM patients is 155.6 mg/dl.
The average Hba1C of the uncontrolled T2DM
patients is 9.7%, the controlled T2DM patients is
8.0%. The average ureum level of the uncontrolled
T2DM patients is 28.05 mg/dl, the controlled T2DM
patients is 27.58 mg/dl. The average systole of the
uncontrolled T2DM patients is 124.9 mmHg, the
controlled T2DM patients is 144mmHg. The average
diastole of the uncontrolled T2DM patients is 77.6
mmHg, the controlled T2DM patients is 89.1 mmHg.
All of the group samples showed the above normal of
ureum levels, which the normal value is 7-20mg/dl.
We have already known that the ureum plasma value
demonstrated the function of the renal. The aim of
this study is to compare ureum plasma level between
CT2DM and UCT2DM. So we used the T-test
statistical analysis to analyze the value of both groups
sample. This study showed that there was significant
difference between CT2DM and UCT2DM
(p<0.005). When there is a damage in kidney or it
does not work properly an increase in urea level will
be seen. Increasing of blood sugar level followed by
increasing blood urea level clearly indicates that there
is a damage in the kidney. Research conducted by
Anjaneyulu et al., 2004 had found that increase urea
and serum creatinine in diabetic rats indicates
ICOSTEERR 2018 - International Conference of Science, Technology, Engineering, Environmental and Ramification Researches
526

progressive renal damage (Anjaneyulu et al., 2004).
In our study, the increasing in serum urea levels
associated with the severity of diabetes, this finding
is in accordance with the fact that serum creatinine
and urea are used as important markers of Glomerular
Filtration Rate (GFR) (Deepa et al., 2011). Our study
is inline as well with the study that was conducted by
Sugam S et al that found that diabetic patients have
higher serum urea in compare to non-diabetic
patients. They reported that 18 out of 103 diabetes
samples have high urea level. An another study also
showed that the increase in mean values of serum urea
136.03 ± SD 74.6 mg/dl in kidney disease patients
with Diabetes mellitus (Mittal et al, 2010). The
increasing levels of serum urea is one of the
important measures of a damage in glomerular which
can, in no way be reversed by intensive treatment plan
of lowering glucose level in diabetic patients. The
only way to control the progressiveness of glomerular
damage and thereby increasing levels of serum urea
is the early detection and intervention.
4 CONCLUSION
The major cause of renal morbidity and mortalityis
DM, and diabetic nephropathy is one of the major
cause of chronic kidney failure. One of the indicator
that is widely used to examine the renal function
failure is blood urea and creatinine levels, it is simple
and useful biomarkers that can be a predictor test to
examine kidney functions (nephropathy) in DM
patients. Blood glucose levels that is in good control
helps to preventthe progressiveness of renal
impairment and one of major cause of chronic renal
failure which is diabetic nephropathy. The good
control of blood glucose level is the most important
requirement in preventing the progressiveness of
renal impairment. In order to monitor the control of
blood glucose level along with blood sugar blood urea
can also be important parameter as we found that
there is strong correlation of blood sugar and urea
level.
ACKNOWLEDGEMENT
The authors gratefully acknowledge that the present
research is supported by Ministry of Research and
Technology and Higher Education Republic
Indonesia, under research grant TALENTA USU of
Year 2018.
REFERENCES
Anderson, D., 2005. Harrison’s principles of internal
medicine.Neurology, 64(8), pp.1488-1489.
Anjaneyulu, M. and Chopra, K., 2004. Quercetin, an anti-
oxidant bioflavonoid, attenuates diabetic nephropathy
in rats.Clinical and Experimental pharmacology and
physiology, 31(4), pp.244-248.
Deepa, K., Manjunatha, G.B.K., Oinam, S.D., Devaki,
R.N., Bhavna, N., Asha, P. and Naureen, A., 2011.
Serum urea, creatinine in relation to fasting plasma
glucose levels in type 2 diabetic patients. International
journal of Pharmacy and Biological sciences, 1(3),
pp.279-283.
Gowda, S., Desai, P.B., Kulkarni, S.S., Hull, V.V., Math,
A.A. and Vernekar, S.N., 2010. Markers of renal
function tests.North American journal of medical
sciences, 2(4), p.170.
Kalra, S.P., 2012. A case for new therapy for diabetes, is it
leptin?. Indian journal of endocrinology and
metabolism,16(Suppl 3), p.S525.
Kamal, A., 2014. Estimation of blood urea (BUN) and
serum creatinine level in patients of renal
disorder. Indian J Fundam Appl Life Sci, 4(4), pp.199-
202.
Kanwar, G., Jain, N., Sharma, N., Shekhawat, M., Ahmed,
J. and Kabra, R., 2015. Significance of serum urea and
creatinine levels in type 2 diabetic patients. IOSR J
Dent Med Sci, 14(8), pp.65-7.
Kementrian Kesehatan, R.I., 2013. Riset kesehatan dasar
(Riskesdas) 2013. Jakarta: Badan Penelitian dan
Pengembangan Kesehatan.
Mehta, R.S., Karki, P. and Sharma, S.K., 2006. Risk
factors, associated health problems, reasons for
admission and knowledge profile of diabetes patients
admitted in BPKIHS.Kathmandu University Medical
Journal, 4(1), pp.11-13.
Melmed, S., 2016. Williams textbook of endocrinology.
Elsevier Health Sciences.
Mittal, A., Sathian, B., Kumar, A., Chandrasekharan, N.
and Sunka, A., 2010. Diabetes mellitus as a potential
risk factor for renal disease among Nepalese: A hospital
based case control study. Nepal journal of
epidemiology, 1(1), pp.22-25.
Rehman, G., Khan, S.A. and Hamayun, M., 2005. Studies
on diabetic nephropathy and secondary diseases in type
2 diabetes. Int. J. Diab. Dev. Ctries, 25, pp.25-29.
Smyth, S. and Heron, A., 2006. Diabetes and obesity: the
twin epidemics. Nature medicine, 12(1), p.75.
Wild, S., Roglic, G., Green, A., Sicree, R. and King, H.,
2004. Global prevalence of diabetes: estimates for the
year 2000 and projections for 2030. Diabetes
care, 27(5), pp.1047-1053.
Yach, D., Stuckler, D. and Brownell, K.D., 2006.
Epidemiologic and economic consequences of the
global epidemics of obesity and diabetes. Nature
medicine, 12(1), p.62.
Zimmet, P., Alberti, K.G.M.M. and Shaw, J., 2001. Global
and societal implications of the diabetes
epidemic. Nature,414(6865), p.782.
Comparison of Ureum Plasma Level between Controlled Type 2 Diabetes Mellitus and Uncontrolled Type 2 Diabetes Mellitus
527
