
Empowerment of PKK Team as Caregiver for Stroke Patient in
PB Selayang II Urban Village, Medan Selayang Sub-district
Haflin Soraya Hutagalung
1
, Irina Kemala Nasution
1
, Nenni Dwi Aprianti Lubis
2*
1
Neurology Department; Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia
2
Nutrition Department; Faculty of Medicine, Universitas Sumatera Utara, Medan, Indonesia
Keywords: Stroke, Caregiver
Abstract: As one of the degeneratives disease with high disability consequences, stroke with all of its consequences
will give physical, psychiatric and social burden on the patients, family and caregiver. One of the efforts to
lessen the burden is behavioral intervention of the support system in didactic discourse and workshop of
taking care post stroke patients at home. We use Wilcoxon Signed Rank bivariate test of several nursing
domain which evaluated pre and post test, such as bathing, oral hygiene, wound prevention, dressing and
feeding which giving changes that clinically and statistically significant (p < 0.01).
1 INTRODUCTION
Stroke is one of the non-contagious diseases that
causes death and disability with 7% on the diagnosis
of health workers (Riskesdas, 2013). The data
obtained in the research shows the hemiparesis
sinistra disability as many as 134 people (23.8%)
and right hemiparesis 133 people (23.7%) (Rambe et
al., 2012). This shows the high rate of post-stroke
disability is still a problem even after the patient is
treated at home (Nasution, 2007), (Misbach and
Jannis, 2011).
Family has a vital role in primary support in
terms of maintaining post-stroke health care during
recovery and rehabilitation periods, where the
absence of this support can result in significantly
reduced recovery (Julianti, 2013). Not only in terms
of health, the incidence of stroke that affects family
member also provides psychosocial effect for patient
and family and caregiver. In general, post-stroke
caregiver people have poor quality of life compared
to the general population, which is due to
depression, anxiety, limitations in social relation,
general health and even higher mortality (Rigby,
2009). The purpose of this community service
activity is to increase public knowledge, especially
cadres and Family Empowerment and Family
Welfare Movement Team (TP PKK) about stroke so
that it can act as a caregiver for stroke patients. The
knowledge and skills gained during this activity are
expected to be transmitted to other community
members.
2 METHODS
This activity was conducted by 3 lecturers and this is
an affiliation activity between Neurology
Department and Nutrition Department, Faculty of
Medicine, Universitas Sumatera Utara (USU) and
PB Selayang II Urban Village, Medan Selayang
Sub-District of assisted by students of Faculty of
Medicine USU. The method of service is carried out
by providing counseling and training to respondents
(i.e. cadres and TP PKK) of PB Selayang II Sub-
District of Medan Selayang, where the service is
also in line with the work program of group 4 (Pokja
4) TP PKK which is managing health program,
environmental sustainability and healthy planning.
The event was held at hall in Medan Selayang
and attended by 25 respondents. Generally, activities
were divided into 2 stages. Stage I (Counseling) was
conducted with a lecture system on the basic concept
of independent stroke nursing effectively. Prior to
the lecture, the respondents were asked to complete
a self-assessment questionnaire in the form of pre-
test before lecture and post-test after lecture. Stage II
(Training) was done by improving the skills of the
respondents as caregiver, especially in self-care. In
this stage II activity, the team was assisted in
Hutagalung, H., Nasution, I. and Lubis, N.
Empowerment of PKK Team as Caregiver for Stroke Patient in PB Selayang II Urban Village, Medan Selayang Sub-district.
DOI: 10.5220/0010073604670471
In Proceedings of the International Conference of Science, Technology, Engineering, Environmental and Ramification Researches (ICOSTEERR 2018) - Research in Industry 4.0, pages
467-471
ISBN: 978-989-758-449-7
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
467
training using standard patient acting as stroke (role-
play workshop).
Counseling and training materials include the
role of general stroke caregiver to basic training on
self-care, such as bathing, feeding and toileting. At
the end of the training period, it is expected that
respondents who have undergone training can
become skilled cadres who can care for stroke
patients independently and even become trainers of
trainers (TOT) by providing knowledge
dissemination of care that has been obtained in
surrounding communities.
The collected data will be analyzed using
Wilcoxon Signed Rank test. The Wilcoxon test is
used to analyze pairs of observed results from two
different whether or not data. Wilcoxon test is used
only for the type of interval or ratio data, and the
data is not normally distributed. The normality test
shows that knowledge and skill variables have
p<0.05, which means that all of the variables are not
normally distributed so that the data analysis is
feasible using the Wilcoxon test
3 RESULTS
Based on the characteristic variables of respondents,
as many as 25 respondents (100%) were women
with an average age of 43 years (age range 18-65
years). The occupation of most respondents was
housewife as many as 18 person (72%), 4 person
(16%) was self employed (2%) and enterpriser was
2 person (8%) and civil servant was 1 people (4%).
Referring to the lattest education, most of the
respondents were graduated from senior high school
as many as 22 person (88%), 2 person (8%) were
graduated from higher education (D3/ S1) and 1
person was graduated from elementary school (4%).
Marital status showed 20 respondents (80%) were
married, 4 respondents (16%) were unmarried and
one respondent (4%) had widow status. The average
number of children owned by total respondents was
as much as 2 people (range 0-6 people).
In terms of knowledge and information about
stroke, as many as 21 respondents (84%) did not
have a family who suffered a stroke, while as many
as 4 people (16%) had a family who had been
encountering or ever had encountered stroke. As
many as 20 people (80%) had heard or had learned
information about stroke, while 5 people (20%) had
not known or never know information about stroke.
Meanwhile, when viewed formal training aspect, as
many as 24 people (96%) had never received general
care training and stroke treatment, while 1
respondent (4%) had ever attended the training.
In the bivariate test, based on pre-test result, it
was found that the highest level of respondent
knowledge before given the extension was in fair
category as many as 13 people (52%), and in good
category as many as 12 people (38%). This shows
that the knowledge level of respondents as caregiver
in stroke sufferer still in fair category. Meanwhile,
after the post-test, the same results were obtained,
the highest level of knowledge of the respondents
after given extension was in fair category as many
as 13 people (52%), and in the good category as
many as 12 people (38%). Furthermore from the
analysis results obtained Z score of 0.001 with a p
value of 1,000 (p>0.05), so it was decided that there
is no difference in the level of knowledge of
respondents as caregivers in stroke patients before
and after given counseling (Table 1).
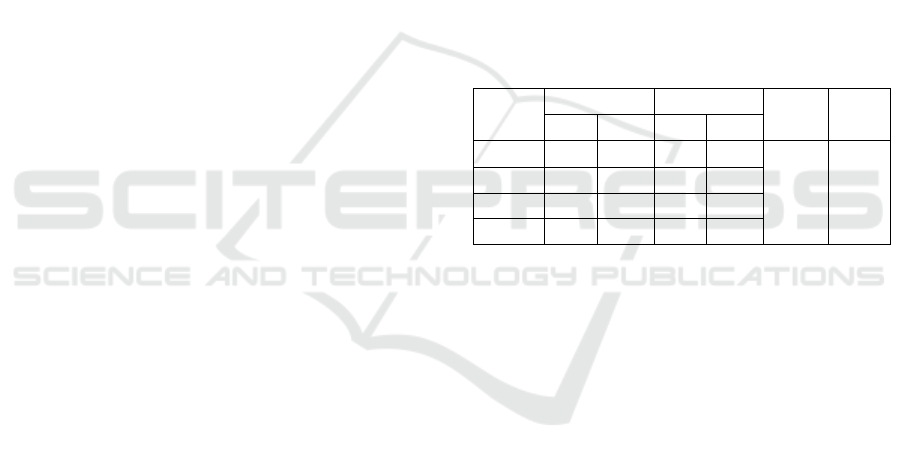
Table 1: Knowledge level of respondents before and after
counseling
Know-
ledge
Pre-test Post-test Z-
score
p-
value
n % n %
Good 12 48 12 48
0.001
1.000
Fair 13 52 13 52
Poor 0 0 0 0
Total 25 100 25 100
Based on pre-test results obtained that all
respondents (100%) failed in the skill of bathing
procedure to the stroke patients. This shows that all
respondents were not skilled in bathing stroke
patients. Meanwhile, after the post-test, the results
obtained were different i.e, all respondents (100%)
were succeeded in the skill of bathing the stroke
patient. Furthermore from the analysis results
obtained Z score of -4.243 with a value of p value of
0.001 (p<0.05), so it was decided there is a
difference in the skills of respondents in the
procedure of bathing stroke patients before and after
training (Table 2).
Based on pre-test results obtained that almost all
respondents (84.0%) failed in the skills of oral
procedures for cleaning stroke patients. This shows
that there were still many respondents who were not
skilled in cleaning the mouth of stroke patients.
Meanwhile, after the post-test obtained different
results, as many as (88.0%) of respondents
succeeded in the oral procedure of cleaning the
mouth of stroke patients. Furthermore from the
analysis results obtained Z score of -4.243 with a
value of p value of 0.001 (p<0.05), so there were
differences in the skills of respondents in the oral
ICOSTEERR 2018 - International Conference of Science, Technology, Engineering, Environmental and Ramification Researches
468
procedure of cleaning stroke patients before andafter
training (Table 3). Based on pre-test results obtained
that all respondents (100%) failed in skills or
procedures to prevent injury in people with stroke.
This shows that all respondents were not at all
skilled in preventing the occurrence of injuries in
people with stroke. Meanwhile, after post-test, there
were different results, all respondents (100%)
succeeded in skill of injury prevention procedure of
stroke patient. Furthermore from the analysis results
obtained Z score of -4.583 with a value of p value of
0.001 (p<0.05), so it was decided there was a
difference in the skills of respondents in the
procedure to prevent injury in stroke patients before
and after training (Table 2).
Based on pre-test results obtained that all
respondents (100%) failed in the skill of dressing
procedures in patients with stroke. This shows that
all respondents were not at all skilled in putting
clothes on stroke patients. Meanwhile, after the post-
test, there were different results, all respondents
(100%) succeeded in the skills of dressing procedure
in stroke patients. Furthermore, from the analysis
results obtained Z score of -5,000 with a value of p
value of 0.001 (p<0.05), so it was decided there was
a difference in the skills of respondents in the
procedure of dressing on stroke patients before and
after training (Table 2).
Based on pre-test results obtained that most
respondents (60.0%) failed in the of wearing
trousers procedure on stroke patients. This shows
that there were still many respondents who were not
skilled in putting pants on stroke patients.
Meanwhile, after the post-test, there were different
results, all respondents (100%) succeeded in the skill
of putting the pants on the stroke patient.
Furthermore from the analysis results obtained Z
score of -3.873 with a value of p value of 0.001
(p<0.05), so it was decided there was a difference in
the skills of respondents in the procedure of putting
pants on stroke patients before and after training
(Table 2).
Based on pre-test results obtained that almost all
respondents (96.0%) failed in the skills of giving
food an beverage procedure to stroke patient. This
shows that there were still many respondents who
were not skilled in giving food and beverage to
stroke patients. Meanwhile, after the post-test, there
were different results (80.0%) of respondents
succeeded in the skill of giving food and beverage
to stroke patient. Furthermore from the analysis
results obtained Z score of -4.359 with a value of p
value of 0.001 (p <0.05), so it was decided there was
a difference in the skills of respondents in the giving
food to stroke patients before and after training
(Table 2).
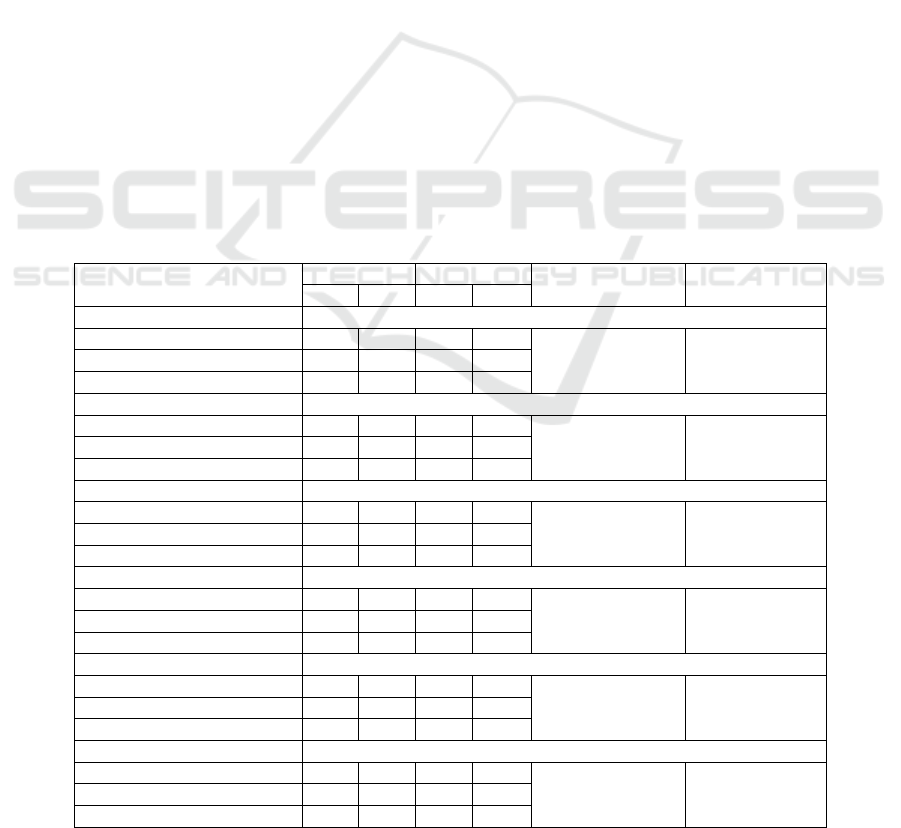
Table 2: Skill procedure of bathing stroke patients in respondents before and after training.
Skill variables Pre-test Post-test Z-score p-value
n % n %
Bathin
g
p
rocedure
Success 0 0 18 72
-4.243
0.001
Fail 25 100 7 28
Total 25 100 25 100
Mouth Cleansing
Success 4 16 22 88
-4.243
0.001
Fail 21 84 3 12
Total 25 100 25 100
Injury prevention procedure
Success 0 0 21 84
-4.583
0.001
Fail 25 100 4 21
Total 25 100 25 100
Dressin
g
p
rocedure
Success 0 0 25 100
-5.000
0.001
Fail 25 100 0 0
25 100 25 100
Puttin
g
p
ants
p
rocedure
Success 10 40 25 100
-3.873
0.001
Fail 15 60 0 0
Total 25 100 25 100
Giving food and beverage
Success 1 4 20 80
-4.359
0.001
Fail 24 96 5 20
Total 25 100 25 100
Empowerment of PKK Team as Caregiver for Stroke Patient in PB Selayang II Urban Village, Medan Selayang Sub-district
469

Based on pre-test results obtained that all
respondents (100%) failed in skills or procedures to
prevent injury in people with stroke. This shows that
all respondents were not at all skilled in preventing
the occurrence of injuries in people with stroke.
Meanwhile, after post-test, there were different
results, all respondents (100%) succeeded in skill of
injury prevention procedure of stroke patient.
Furthermore from the analysis results obtained Z
score of -4.583 with a value of p value of 0.001
(p<0.05), so it was decided there was a difference in
the skills of respondents in the procedure to prevent
injury in stroke patients before and after training
(Table 2).
Based on pre-test results obtained that all
respondents (100%) failed in the skill of dressing
procedures in patients with stroke. This shows that
all respondents were not at all skilled in putting
clothes on stroke patients. Meanwhile, after the post-
test, there were different results, all respondents
(100%) succeeded in the skills of dressing procedure
in stroke patients. Furthermore, from the analysis
results obtained Z score of -5,000 with a value of p
value of 0.001 (p<0.05), so it was decided there was
a difference in the skills of respondents in the
procedure of dressing on stroke patients before and
after training (Table 2).
Based on pre-test results obtained that most
respondents (60.0%) failed in the of wearing
trousers procedure on stroke patients. This shows
that there were still many respondents who were not
skilled in putting pants on stroke patients.
Meanwhile, after the post-test, there were different
results, all respondents (100%) succeeded in the skill
of putting the pants on the stroke patient.
Furthermore from the analysis results obtained Z
score of -3.873 with a value of p value of 0.001
(p<0.05), so it was decided there was a difference in
the skills of respondents in the procedure of putting
pants on stroke patients before and after training
(Table 2).
Based on pre-test results obtained that almost all
respondents (96.0%) failed in the skills of giving
food an beverage procedure to stroke patient. This
shows that there were still many respondents who
were not skilled in giving food and beverage to
stroke patients. Meanwhile, after the post-test, there
were different results (80.0%) of respondents
succeeded in the skill of giving food and beverage
to stroke patient. Furthermore from the analysis
results obtained Z score of -4.359 with a value of p
value of 0.001 (p <0.05), so it was decided there was
a difference in the skills of respondents in the giving
food to stroke patients before and after training
(Table 2).
4 DISCUSSION
Intensive training of knowledge interventions to
post-stroke caregiver will provide a higher rate of
qualitative knowledge than control group (Bakas,
2009). Skills are skills in performing tasks that are
the result of training and education (Dunnette,
2006). (Evita, 2013) concluded that the standard
training of infant growth monitoring on Puskesmas’
cadres increases knowledge, skills and compliance
when compared to only the modules (Priyono,
2017). Priyono's research results also explain the
difference of knowledge and skills before and after
emergency education at the MANTAP agent
(community responsive) (Evita, 2013). This is the
reason why empowerment and training of families
and caregivers especially in post-stroke care is
essential because good knowledge and skills will not
only speed up the patient's recovery but also avoid
families and caregivers from burnout due to lack of
knowledge and skills.
5 CONCLUSIONS
Intervention of caregiver behavior and knowledge of
stroke in this study provide statistically significant
differences in caregiver skills in caring for post-
stroke patients, so further research is needed to
assess the effect of long-term intervention.
ACKNOWLEDGEMENTS
If any, this community service is funded by
Universitas Sumatera Utara through Non PNBP and
BPPTN USU T.A. 2018 grant with Letter of
Assignment no. 396/UN5.2.3.2.1/PPM/2018 dated
16 April 2016.
REFERENCES
Bakas, T., Farran, C.J., Austin, J.K., Given, B.A., Johnson,
E.A., Williams, L.S. 2009. Content Validity and
Satisfaction with A Stroke Caregiver Intervention
Program. J Nurs Scholarsh 41(4): 368 – 375.
Dunnette. 2006. Handbook of Industrial and Organizations
Psychology. New York: John Wiley and Sons.
ICOSTEERR 2018 - International Conference of Science, Technology, Engineering, Environmental and Ramification Researches
470

Evita, D., Mursyid, A., Siswati, T. 2013. Pelatihan
Meningkatkan Pengetahuan dan Keterampilan Kader
Puskesmas dalam Penerapan Standar Pementauan
Pertumbuhan Balita di kota Bitung. Jurnal Gizi dan
Dietetik Indonesia 1(1): 15 – 21.
Julianti, E. 2013. Pengalaman Caregiver dalam Merawat
Pasien Pasca Stroke di Rumah pada Wilayah Kerja
Puskesmas Benda Baru Kota Tangerang Selatan.
Skripsi FKIK UIN Syarif Hidayatullah: 19-129.
Misbach, J. dan Jannis, J. 2011. Diagnosis Stroke dalam
Misbach, J., Soertidewi, L., Jannis, J(ed). Stroke:
Aspek Diagnostik, Patofisiologi, Manajemen. Badan
Penerbit FKUI. Jakarta: 57-84
Nasution, D. 2007. Pidato Pengukuhan Jabatan Guru
Besar Tetap: Strategi Pencegahan Stroke Primer. USU
Press. Medan: 1-27.
Priyono, A.H. 2017. Perbedaan Pengetahuan Sebelum dan
Sesudah Pendidikan Kegawatdaruratan dan Analisis
Keterampilan pada Agen MANTAP di Desa Munca,
Pesawaran, Lampung. Skripsi FK Universitas
Lampung.
Rambe, A.S., Fithrie, A., Nasution, I., Tonam. 2012. Profil
Pasien Stroke pada 25 Rumah Sakit di Sumatera
Utara. Neurona. 30(2): 1-7.
Rigby, H., Gubitz, G., Philips, S. 2009. A Systematic
Review of Caregiver Burden Following Stroke.
International Journal of Stroke 4: 285-292.
Riskesdas. 2013. Riset Kesehatan Dasar Tahun 2013.
Badan Penelitian dan Pengembangan Kesehatan
Kementrian Kesehatan RI. Jakarta: 91-93.
Empowerment of PKK Team as Caregiver for Stroke Patient in PB Selayang II Urban Village, Medan Selayang Sub-district
471
