
Cylous Ascites in Gynaecology Malignancy
Deri Edianto
1
, Isnayu Jurimal
1
and Muhammad Rizki Yaznil
1
1
Department of Obstetrics and Gynecology, Universitas Sumatera Utara, Medan, Indonesia
Keywords: Chylous Ascites, Lymph Nodes, Malignancy, Paracentesis.
Abstract: Chylous ascites is ascites caused by leakage of lymphatic fluid which contain lipid to peritoneal cavity and a
rare malignancy complication. Chylous ascites was reported in 1 from 2000 cases in 20 years. We report a
59 years old housewife, para 3, who was admitted to emergency unit Adam Malik General Hospital with
abdominal enlargement. She has been experiencing this in the last 2 months ago. The signs and symptoms
were nausea, vomiting, loss of appetite. She was diagnosed with carcinoma of the cervix stage II B on
October 2016 and received chemoradiation (external beam radiotherapy 28x, chemotherapy 6x,
brachytherapy 6x) in other hospital. The general findings were within normal limit. BMI was 15.82 kg/m
2
(underweight). On physical examination, head, neck, and chest within normal findings. Abdominal findings
were enlargement, distension, shifting dullness, no mass was palpable. The cervix looks fibrotic and no
residual mass visible. Laboratory findings are thrombocytosis (629.000/mm
3
), hypoalbuminemia (2,7 g/dL),
blood urea was within normal value, creatinine was 1,58 mg/dL. Electrolyte values were within normal
except hyponatremia (132 mEq/L). Chest X-ray examination was atelectasis at right middle lung. CT scan
finding suggested metastatic process in the liver. The patient was diagnosed with cervical cancer II B post
chemoradiotherapy metastasize to the liver, massive ascites and hypoalbuminemia. Abdominal Paracentesis
findings were 4000 ml of white milky fluid and the levels of triglycerides in the ascitic content were 1057
mg/dl. As a conclusion, chylous ascites is very rare with malignancy and cirrhosis are the main causes.
Diagnosis of chylous ascites is paracentesis with increased triglyceride levels and the management mainly
conservative.
1 INTRODUCTION
Ascites is a collection of fluid in peritoneum space.
This condition happens when there is excessive fluid
production and inadequate absorption. Ascites is one
of many malignancy complications. Four in five
patients with malignancy ascites were caused by
ovarian cancer, gastrointestinal, breast, pulmonary,
uterine, and cervical cancer. Patients with malignant
ascites have poor prognosis with life expectancy
only 1-4 months and five years survival rate is
48,7% (Damodar and Rao, 2011)
Chylous ascites is caused by leakage of
lymphatic fluid that contains lipid to peritoneal
space. Chylous ascites can be caused by surgical
trauma to lymphatic vessels, tuberculosis, cirrhosis,
lymphoma, radiotherapy, and direct lymphatic
metastases. Reported incidence of chylous ascites is
1 from 20.000 cases in 20 years. The incidence
predicted to be increasing because of increasing life
expectancy in cancer patients and increasing
aggressive cardiothoracic and abdominal
intervention (surgery). Al-Busafi found that chylous
ascites incident were 1 in 11.589 cases in 2013.(Al-
Busafi et al., 2014) So it is still a very rare
complication of malignancy or its treatments.
Treatment of chylous ascites is still
controversial. It can be standard conservative
treatment or surgery for unresponsive
patients.(Solmaz et al., 2015)
2 CASE REPORT
Mrs.N, 59 years old, P3A1, housewife, who was
admitted to emergency unit Adam Malik general
hospital on June 12
th
, 2017 with an abdominal
enlargement. She has been experiencing this
condition in the last 2 months. The signs and
symptoms were nausea, vomiting, history loss of
Edianto, D., Jurimal, I. and Yaznil, M.
Cylous Ascites in Gynaecology Malignancy.
DOI: 10.5220/0010070504330435
In Proceedings of the International Conference of Science, Technology, Engineering, Environmental and Ramification Researches (ICOSTEERR 2018) - Research in Industry 4.0, pages
433-435
ISBN: 978-989-758-449-7
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
433
appetite, history of weight loss. There were no
abdominal pain, vaginal bleeding and discharge. She
was diagnosed with carcinoma of the cervix stage II
B on October 2016 and received chemoradiation
(external beam radiotherapy 28x, chemotherapy 6x,
brachytherapy 6x) in other hospital, last procedure in
February 2017. Menarche at the age of 14 years old
with regular 28 - 30 days cycle, lasting for 5 – 7
days. Menopause at 54 years old.
Vital sign was normal. BMI was 15.82 kg/m
2
(underweight). On physical examination, head, neck,
and chest were normal. Abdominal were
enlargement, distension, shifting dullness (+), no
mass was palpable. The bowel sound was present
and revealed normal. The inspection showed fibrotic
cervix. In vaginal examination there were palpated
fibrotic cervix, normal uterine size, no locoregional
residual mass.
Full blood count was normal except
thrombocytosis (629 000/mm
3
). Liver function test
was normal. The patient was hypoalbuminemia with
serum albumin level 2,7 g/dL. Blood urea was
normal, creatinine was 1,58 mg/dL. Electrolyte
values were normal except slight hyponatremia (132
mEq/L). Chest X-ray examination was plate-like
atelectasis at right middle lung. CT scan findings
were multiple metastatic nodule in the liver, bilateral
pleural effusion and ascites, bilateral kidney atrophy,
especially the left kidney.
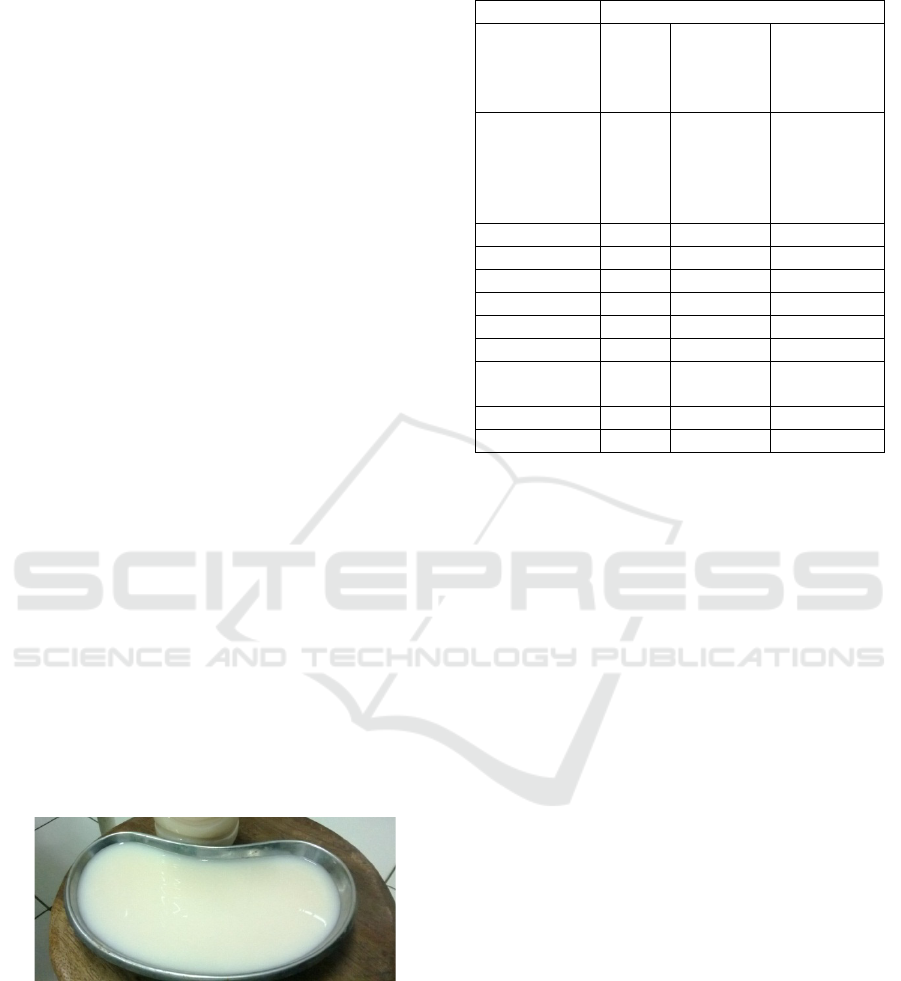
Paracentesis findings were 4000 ml of white
solid-fluid from ascitic patient (Figure 1). The
patient was treated with intraperitoneal
chemotherapy with cisplatin 100 mg in normal
saline 2 litres. Cytologic result was metastatic
carcinoma. Analysis of peritoneal fluid were in
Table 1.
Figure 1: Chylous ascites
Table 1: Analysis of ascites fluid
3 DISCUSSION
Chylous ascites is a collection of lymphatic fluid
from peritoneal space with high triglycerides content
more than 110 mg/dL. Lymphatic system consists of
lymphatic fluid, lymphatic vessels, and bone
marrow. Thoracic duct is a point where there is a
transition and mixture of many chylomicrons and
less lymphatic fluid. If lymphatic fluid is above
cisterna chylous, it is called chylous and milky
because it contains high triglyceride. If the fluid is
located below the point of transition, it is known as
lymphatic where the triglyceride level is minimal
and it is clear or reddish.(Micha et al., 2012; Al-
Busafi et al., 2014)
Three basic mechanisms of chylous ascites are
primary fibrosis of lymphatic nodes caused by
obstruction of lymphatic drainage from gut to
chylous cisterna from sub serous lymphatic from
malignancy, lymphatic fluid exudation to peritoneal
space and direct lymphatic fluid leakage (lymph
peritoneal fistulae) caused by thoracic duct
obstruction.(Cárdenas and Chopra, 2002)
Chylous ascites can be caused by traumatic and
atraumatic. Atraumatic condition such as
malignancy, cirrhosis, mycobacterium infection, and
others.(Al-Busafi et al., 2014) Our patient was
diagnosed with cervical cancer stage II B. Ascites is
one of the complication of malignant process
(incidence up to 2%). The traumatic condition is
direct lymphatic trauma, one of which is due to
Colou
r
Milky white
Total
protein
1.34 g/dl Transudate
(< 3gr/dl)
Exudate (>
3
g
r/dl)
LDH 112 U/L Transudate
(< 200
U/L)
Exudate (>
200 U/L)
Glucose 147 m
g
/dl 55-140
p
H8 7-8
WBC 0.343 10
3
/uL
RBC 0.002 10
6
/uL
MN cell 91.3 %
PMN cell 8.7 %
Total
cholesterol
55 mg/dl < 200
Tri
g
l
y
ceride 1057 m
g
/dl 40-200
Albumin 0.5 g/dl 3.5-5.0
ICOSTEERR 2018 - International Conference of Science, Technology, Engineering, Environmental and Ramification Researches
434

radiotherapy. Hurst and Edward reported cases of
chylous ascites after radiotherapy. During the
explorative laparotomy, there is a damage of small
intestine and chylous leak.(Lentz et al., 1990) Our
patient was received chemoradiotherapy treatment
(external beam radiotherapy 28x, cisplatin
chemotherapy 6x and brachytherapy 6x).
Several clinical findings are progressive and
abdominal distention (81% with pain) and
nonspecific pain (14%). Other symptoms are
dyspnoea, weight loss, anorexia, malaise,
steatorrhea, malnutrition, lymphatic enlargement,
and night sweat. Physical examination findings are
ascites, pleural effusion, lower extremity edema,
lymphadenopathy, cachexia, weight loss, and
hernia.(Cárdenas and Chopra, 2002; Steinemann et
al., 2011; Al-Busafi et al., 2014)
In laboratory findings, abdominal paracentesis is
the main diagnostic tools and very important for
evaluation and treatment.(Baiocchi et al., 2010; Al-
Busafi et al., 2014)
Chylous ascites is a milky-
appearing fluid with high levels of triglycerides that
are usually >110 mg/dl or > 1,2 mmol/l.(Steinemann
et al., 2011) Additional examinations are CT scan,
lymphoscintigraphy to detect abnormal lymphatic
drainage, laparoscopy and laparotomy. Abdominal
paracentesis from our patient were 4000 ml of milky
and cloudy fluid and levels of triglycerides in ascitic
fluid were 1057 mg/dl.
Conservative management of chylous ascites are
low-fat diet, decreasing intestine lymphatic drainage,
triglyceride lymphatic transport, Total Parenteral
Nutrition (TPN), somatostatin and abdominal
paracentesis to reduce the symptoms. Other therapy
for unresponsive cases are Trans-jugular Intrahepatic
Portosystemic Shunt (TIPS), angiography and
peritoneovenous shunt (Manolitsas et al., 2002; Al-
Busafi et al., 2014)
4 CONCLUSIONS
Chylous ascites is a kind of ascites that happened
very rarely. Malignancy and cirrhosis are the main
etiology for adult patient, while for children the
etiology usually congenital abnormalities and
trauma. The diagnostic of chylous ascites made with
analysis of triglycerides content of ascitic fluid from
paracentesis. The treatment of underlying disease is
the first important step to treat the patients.
Treatments such as low-fat diets, triglycerides
intake, paracentesis, TPN and somatostatin could be
considered. For refractory cases, we could use
Trans-jugular Intrahepatic Portosystemic Shunt
(TIPS), exploratory surgery and peritoneovenous
shunt.
REFERENCES
Al-Busafi, S. A. et al. (2014) ‘Chylous Ascites: Evaluation
and Management’, ISRN Hepatology. doi:
10.1155/2014/240473.
Baiocchi, G. et al. (2010) ‘Chylous ascites in gynecologic
malignancies: Cases report and literature review’,
Archives of Gynecology and Obstetrics. doi:
10.1007/s00404-009-1211-0.
Cárdenas, A. and Chopra, S. (2002) ‘Chylous ascites’, The
American Journal of Gastroenterology. doi:
10.1111/j.1572-0241.2002.05911.x.
Damodar, G. and Rao, A. (2011) ‘A rare clinical
presentation of Carcinoma Cervix - Ascites’, Indian
Journal of Pharmacy Practice, 4, pp. 57–60.
Lentz, S. S., Schray, M. F. and Wilson, T. O. (1990)
‘Chylous ascites after whole-abdomen irradiation for
gynecologic malignancy’, International Journal of
Radiation Oncology, Biology, Physics. doi:
10.1016/0360-3016(90)90554-W.
Manolitsas, T. P., Abdessalam, S. and Fowler, J. M.
(2002) ‘Chylous ascites following treatment for
gynecologic malignancies’, Gynecologic Oncology.
doi: 10.1006/gyno.2002.6754.
Micha, J. P. et al. (2012) ‘Recurrent lymphatic ascites in a
patient cured of cervical carcinoma’, Gynecologic
Oncology Reports. doi: 10.1016/j.gynor.2012.05.004.
Solmaz, U. et al. (2015) ‘Chylous ascites following
retroperitoneal lymphadenectomy in gynecologic
malignancies: Incidence, risk factors and
management’, International Journal of Surgery, (Part
A), pp. 88–93. doi: 10.1016/j.ijsu.2015.02.020.
Steinemann, D. C. et al. (2011) ‘Atraumatic chylous
ascites: Systematic review on symptoms and causes’,
Journal of the American College of Surgeons. doi:
10.1016/j.jamcollsurg.2011.01.010.
Cylous Ascites in Gynaecology Malignancy
435
