
Emergency Medical Service Reference Model for Low Impact and
High Frequent Disaster in Indonesia
Nur Budi Mulyono, Akbar Adhi Utama, Noorhan Firdaus Pambudi, Marina Natalia Tampubolon,
Niken Larasati and Layung Anindya Prasetyanti
Institut Teknologi Bandung
nurbudi@sbm-itb.ac.id
Keywords: healthcare aid, disaster, emergency medical service.
Abstract: Located in archipelago and intersection of 3 tectonic plates, Indonesia susceptible to the low impact and high
frequency types of disaster such as flood, fire, landslides etc. These disaster types unexpectedly create more
economic losses and disturb stability of social and economic order since less preparation and lack of reference
model. One of the important humanitarian aid of catastrophic event like disaster is healthcare distribution
system. This study aims to find out an appropriate emergency medical service (EMS) model for developing
country like Indonesia considering nature of low impact and high frequency disaster. The EMS has two
famous reference model: Anglo American and Franco German with the difference in the flow of medical
doctor, ambulance, medical equipment, and the use of medicine. We conduct a deductive assessment of those
two reference model and create recommendation of suitable EMS model for developing countries like
Indonesia. The disaster’s stakeholder such as National Board of Disaster Countermeasure (BNPB), Indonesian
Red Cross (PMI), hospital and any other organizations involved in health care aids services can take benefit
of our recommendation.
1 INTRODUCTION
As the world has been witnessing an improvement of
life quality, the importance of emergency medical
service for emergency, disaster, and catastrophic
conditions is getting more recognition nowadays.
Disasters, both natural and manmade disasters, have
high dependency on emergency medical services.
Therefore, humanitarian logistics covering logistics
aid for vulnerable people, in which disaster healthcare
is included (Tomasini and Wasenhove, 2009; Kovacs
and Spens, 2007), also had been gaining considerable
attention.
As a result, there has been needs for emergency
medical service as well as humanitarian aid logistics
for events of disaster. While
humanitarian logistics could partly rely on social and
volunteer activities, emergency medical service fully
rely on the involvement of local government or the
municipals. Therefore, building reliable emergency
medical service to response immediate disaster is a
must for the citizen, rather than rely on the one
operated by volunteers.
Being an archipelago, between two oceans, on
intersection of three tectonic plates, and lying right on
equator, makes Indonesia vulnerable to disasters.
Java Island as the most inhabited island in Indonesia,
bear the risk of both natural and manmade disasters,
especially the small scaled ones.
This research aims to develop emergency medical
service for disasters in Indonesia
considering currently exist response system for
disaster mitigation. As reference model, we will refer
to the two previously mentioned basic model of
emergency medical service.
2 LITERATURE REVIEW
A supply chain is essentially a network consisting of
suppliers, manufacturers, distributors, retailers and
customers that manage material flows, information
flows and financial flows (Wassenhove, 2005). The
36
Mulyono, N., Utama, A., Pambudi, N., Tampubolon, M., Larasati, N. and Prasetyanti, L.
Emergency Medical Service Reference Model for Low Impact and High Frequent Disaster in Indonesia.
In Proceedings of the 2nd International Conference on Sociology Education (ICSE 2017) - Volume 2, pages 36-40
ISBN: 978-989-758-316-2
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

difference between supply chain in business context
and supply chain in disaster will face uncertainty, like
when, where, what, how much, where from and how
many times to procure and distribute to disaster area.
2.1 Humanitarian Supply Chain
Humanitarian supply chains provide the response to
disasters. The definition of humanitarian supply chain
is derived from the definition of basic supply chain,
“a set of approaches utilized to efficiently integrate
suppliers, warehouses, and stores, so that
merchandise is produced and distributed at the right
quantities, to the right locations, and at the right time;
in order to minimize system wide costs while
satisfying service level requirements”. This concept
can be used in the humanitarian supply chain when
applied in the disaster relief and excluding the term
“customer” or “store” (Yadav and Barve, 2015)
Thomas and Kopczak (2005) from The Fritz Institute
define there are seven activities include in the
humanitarian supply chain, such as preparation,
planning, procurement, transportation, storage,
tracking and custom clearance. Supply chain in
humanitarian needs to be flexible and able to respond
quickly to unpredictable events effectively (between
life and death) and efficiently (treating great number
of victims) under heavy budget constraints (Heasilp
et al, 2010; Costa et al, 2012).
Humanitarian supply chain consist of more than
just humanitarian organization. The list goes to
donors, aid agencies, NGOs, governments, the
military, logistic service providers and suppliers as
the main actors in HSC. (Sahebi et al, 2016).
2.2 Humanitarian Aid Logistic
Logistics is an important factor in humanitarian aid
operations, to the extent that logistics effort account
for 80 percent of disaster relief (Trunick, 2005;
Kovacs and Spens, 2007). Delivering humanitarian
aid needs to be in rapid response to serve the disaster
victims and minimizing the impacts.
Logistic operations in humanitarians is the
processes and systems involved in mobilizing people,
resources, skills and knowledge to help vulnerable
people affected by disaster (Wassenhove, 2006).
Humanitarian logistics is an umbrella term for a
mixed array of operations (Kovacs and Spens, 2007).
The Fritz Institute (2004) defined humanitarian
logistic as “tasks, all the process of planning,
implementing and controlling the efficient, cost-
effective flow and storage of goods and materials as
well as information, from the point of origin to the
point of consumption for the purpose of meeting the
beneficiary’s requirements and alleviate the suffering
of vulnerable people (Vitoriano et al, 2013)
The purpose of humanitarian aid logistic to aid
people in their survival. There are two main streams
of humanitarian logistics that can be distinguished
named as continuous aid work and disaster relief.
While the focus of disaster relief operations is to
design the transportation of first aid material, food,
equipment and rescue personnel from supply points
to a larger number of destination nodes
geographically scattered over the disaster region and
the evacuation transfer of people affected by the
disaster to the health care centers safely and very
rapidly (Barbarosoglu et al, 2002; Kovacs and Spens,
2007).
Humanitarian aid logistic focus on delivering
rescue team and goods. In disaster relief, the most
needed goods by disaster victims such as water,
medicine, chlorination tablets, tents, blankets and
protein biscuits for malnourished children (Dignan,
2005; Kovacs and Spens, 2007). The procurement
process of humanitarian aid including healthcare is
separated into three phases according to disaster life
cycle, preparedness, response and recovery.
Vaillancourt (2011) mentioned the first phase is
planning the emergencies and prepare the relevant
materials for different types of needs into kits. The
phase continue to deliver the goods to the people in
need, the second phase. This phase can be somewhat
challenging due to infrastructure and unpredictable
demand. In the response phase might focus on
different needs and thus there exists a multitude of
kits such as medical, educational, water and sanitation
and household. The last phase is aim to enables the
postponement of inventory allocations to specific
countries (Scholten et al, 2010).
To reduce the great number of victims, the
Emergency Medical Service (EMS) is employ during
the second phase of disaster, in the response phase.
EMS can be defined as “a comprehensive system
which provides the arrangements of personnel,
facilities and equipment for the effective, coordinated
and timely delivery of health and safety services to
victims of sudden illness or injury. (Al-Shaqsi, 2010).
EMS is really helpful and beneficial during the
disaster because it is an integral part of any effective
and functional health care system that serve medical
and trauma emergencies utilizing advanced clinical
technology. However, previous literature does not
discuss on the suitability assessment of using EMS
model as well as the applicability of EMS in
Indonesian context.
Emergency Medical Service Reference Model for Low Impact and High Frequent Disaster in Indonesia
37
3 REFERENCE MODEL
The methodology used in this study is exploratory
analysis employing qualitative and literature review
to generate reference model in providing Emergency
Medical Service during disaster. There are two well-
known model implemented in Emergency Medical
Services system, called as the Franco-German model
and the Anglo-American model. The Franco-German
model of EMS delivery is based on the “stay and
stabilize” philosophy (Huiyi, 2007). In the Franco-
German model, physicians and technology are sent to
the scene in the hope of providing a higher level of
emergency care before the patient’s arrival at the
hospital (Arnold, 1998). Figure 2 illustrates medical
service process of Franco-German model.
On the other hand, the Anglo-American model is
based around “scoop and run” philosophy (Dick,
2003). Here, patients are brought to hospital-based
emergency departments so that they may be provided
a higher level of care (Arnold, 1998). Figure 3
illustrates medical service process of Anglo-
American model.
Arnold (1998) argued that most countries
develops new emergency care systems in recent years
following the Anglo-American model, as exemplified
by emergency medicine in the United States.
However, there is no comparative multinational
studies exist to demonstrate the superiority of one
model over the other. Critics have noted several
problems with the Franco-German model: Physicians
are not well trained, not well supervised, and not
subject to the same quality-assurance controls as
physicians in Anglo-American systems (Arnold,
1998).
This study focuses on the former two terminology
of emergency medical services model, Franco-
German model and Anglo-American model as their
applicability in developing countries like Indonesia.
Indonesian Ministry of Health had showed the list of
medicine in the condition of medical post during
disaster whether within or without physician in the
team through Regulation of
Indonesian Ministry of Health No. 059 Year
2011.
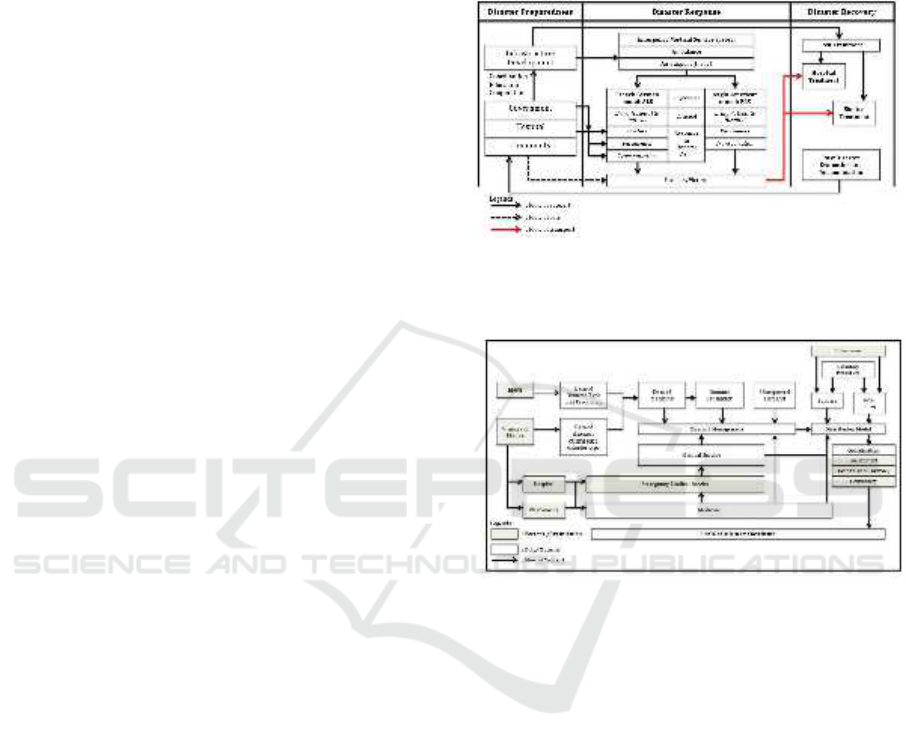
The proposed model of healthcare aid supply
chain during disaster in consideration of Emergency
Medical Services as the supporting part on the supply
chain can be seen in Figure 1.
Beside the model that provide the application of
Emergency Medical Services in healthcare aid supply
chain during disaster there also several aspects should
be considered to maintain better performance in the
supply chain. Those several aspects is described in
Figure 2 and can be seen in the following points:
Demand management;
Distribution model; and
Coordination.
Figure 1: The model of healthcare aid supply chain.
Based on disaster life cycle in which EMS
become main role in disaster response.
Figure 2: Aspects, participating parts, and material/data.
Flow of healthcare aid supply chain in Indonesia.
BNPB is acronym for National Board of Disaster,
Countermeasure which responsible to manage
disaster resilience and developed by Indonesian
Government.
3.1 Demand Management
This aspect will be focused on how the supply chain
fulfill the demand of healthcare services during
disaster. There will be a rapid increasing on demand
with limited supply of medicine, medical staff,
physician, and medical equipment’s. This aspects will
be affected by several consideration such as:
Disaster type and frequency
Disaster impact (risk and hazard)
Disaster to diseases mapping
Demand estimation
ICSE 2017 - 2nd International Conference on Sociology Education
38

3.2 Distribution Model
This aspect will be focused on how the healthcare aid
collected and disseminated to patients from disaster.
It will be started from funding, sourcing, making or
producing, up to delivering.
Funding means the activity will be about the
financial support to provide health care aid
during disaster.
Sourcing means the activity will be about the
vendor selection (i.e. hospital, pharmacies) to
provide medicine and medical staff to help
patients from disaster.
Make means the production processes of
medical service operation
Deliver means that the transportation or
mobilization processes of medicine and medical
services.
3.3 Coordination
This aspect will be focused on how the participating
parts on health care aid supply chain coordinated to
perform better medical services to patients from
disaster. There are several consideration such as:
Actors included hospital, pharmacies, medical
staff, government, community, and other parts
involved in disaster resilience especially in
providing health care aid.
Information to support demand estimation for
supplying medical services to patients from
disaster.
Infrastructure to support medical services
during disaster such as road and supporting part
(i.e. fire fighter forces, army forces).
Funding need coordination to avoid chaotic and
corrupted system during disaster.
Indonesian government already maintain the
system for management of medicine by published a
regulation to overcome all aspects that explained in
this study. Management of medicine based on the
Regulation of Ministry of Health
Number 059 , 2011 as below:
Requirement planning
Provision of drugs and medical supplies
Storage and distribution
Use and control
Recording, evaluating, and reporting
Destruction and disposal
Indonesian government also developed
several considerations regarding provision of drugs
and medical supplies also based on the Regulation of
Ministry of Health Number 059, 2011. The
considerations as follow:
Type of disaster
Disaster area and the number of affected victims
Current medical stock
3.4 Human Resource and
Transportation
Human resources such as doctors and/or paramedics
are needed in disaster responses phase. If the
Emergency Medical Service System adopt the
French-German model then doctors and paramedics
will be needed, otherwise if the Emergency Medical
Service System adopt the Anglo-American model
then only paramedics will be needed as main human
resources. In the transportation, ambulance will help
the doctors and/or paramedics to mobilize from
and/or to disaster area. In the several developed
countries, air support will provided by helicopter as
another transportation mode. In Figure 1 and 2 can be
concluded that in French-German model there is
possibility the number of doctors can be larger and
the number of transportation mode can be smaller,
meanwhile in Anglo-American model there is
possibility the number of doctors can be smaller and
the number of transportation mode can be larger.
3.5 Medicine and Medical Equipment
The information explained in the regulation is the list
of medicine supplies needed during disaster. The
regulation distinguish the list into two type such as:
list of medicine supplies for medical post without
physician or doctor and list of medicine supplies for
medical post with physician or doctor. There are two
possibilities why the regulation distinguish the list
into two terms. First, there is possibility that the
regulation already recognized both model in
Emergency Medical Service system. Second, there is
also possibility that the regulation realize that there is
some lack of physician in several medical post or
clinic in rural area. The regulation itself noted that the
information was adopted from a book entitled New
Emergency Health KITs published by WHO.
3.6 Assessment of Reference Model
There are three phases in current healthcare
distribution system during disaster in Indonesia.
Firstly, the pharmaceutical and medical support
distribution phase from national buffer stock during
disaster. In this stage, all distribution will be
responsible by Indonesian Directorate General of
Pharmaceutical and Medical to support disaster
victims. Secondly, the distribution phase from
province to district. If the district has buffer stock and
receive support from other source, the distribution
can be proceed based on request from head of district
Emergency Medical Service Reference Model for Low Impact and High Frequent Disaster in Indonesia
39

public health care office. Thirdly, the distribution
process from district to remote hospital, field hospital,
Indonesian armed force healthcare facility and private
healthcare facility. In this phase, all medicine and
medical support distribution will handle by district
public health office to the healthcare unit based on the
data of victims and disease type.
The paramedic personnel will use stock card form
to record and control healthcare inventory during
emergency response. All healthcare inventory
received, usage and latest stock should report daily,
weekly and monthly. This report process will be
evaluate during disaster response phase.
4 CONCLUSIONS
Through limited resources of doctors and ambulance
or transportation modes, EMS will provide medical
services for low impact disaster such as fire and flood
effectively. The problem is there are no specific
model had been used of EMS in Indonesia. There are
two contrary model had been known by worldwide,
French-German model with the concept of ‘bring the
hospital to the patient’ and Anglo-American model
with the concept of ‘bring the patient to the hospital’.
This study provide the necessary information about
both of the model and contextualized to Indonesian
disaster management problems through healthcare
aid supply chain mapping. There is some aspects
should be considered to adopt the model in the future.
There are: (1) demand management; (2) distribution
model; and (3) coordination. By providing this model,
further research can be conducted by starting
considering to mapped cost effectiveness of the EMS
model implemented in Indonesia with consideration
of transportation cost, medicine price (this study
already provide the list of medicine needed with its
prices), and infrastructure condition in Indonesia. In
another perspectives, different research also can be
conducted to mapping the needs of preparing the
model to be implemented in Indonesia.
REFERENCES
Al-Shaqsi, S., 2010. Models of international emergency
medical service (EMS) systems. Oman medical
journal, 25(4), 320.
Healslip, G., Mangan, J., Lalwani, C. 2010. Modeling a
Humanitarian Supply Chain Using the Structured
Analysis and Design Technique (SADT). University of
Hull Logistics Institute. UK.
Kölsch, F., Fricke, K., Mahler, C., Damanhuri, E., 2005.
Stability of landfills – The Bandung disaster. In:
Proceedings of the 10th International Landfill
Symposium, Cagliari, Italy.
Kovacs, G., Spens, K.M., 2007. Humanitarian logistics in
disaster relief operations. International Journal of
Physical Distribution and Logistics Management 37 (2)
99 – 114.
Sahebi, I.G., Arab, A., Moghadam, R.S., 2016. Analyzing
the barriers to humanitarian supply chain management:
A case study of the Tehran Red Crescent Societies.
International Journal of Disaster Risk Reduction.
Scholten, K., Pamela Sharkey Scott, Brian Fynes. 2010.
"(Le)agility in humanitarian aid (NGO) supply chains."
International Journal of Physical Distribution and
Logistics Management 40 (8/9): 623-635.
Stout, J., Pepe, P. E., Mosesso, V. N. 2000. A Ll–Advanced
Life Support Vs Tiered-Response Ambulance Systems.
Prehospital Emergency Care, 4(1), 1-6.
Thomas, A.S., Kopczak, L.R. 2005. From Logistics to
Supply Chain Management: The Path Forward in the
Humanitarian Sector. Fritz Institute.
Vaillancourt, A. 2016. Kit management in humanitarian
supply chains. International Journal of Disaster Risk
Reduction.
Vitoriano et al. 2013. Decision Aid Models for Disaster
Management and Emergencies, Atlantis Computational
Intelligence Systems 7, Atlantis Press.
Wassehhove, LN. V. 2005. Humanitarian Aid Logistics:
supply chain management in high gear. Journal of the
Operational Research Society 57, 475-489.
Yadav, D.K., Barve, A. 2014. Analysis of critical success
factors of humanitarian supply chain: an application of
interpretive structural modelling. International Journal
of Disaster Risk Reduction 12, 213 - 225
ICSE 2017 - 2nd International Conference on Sociology Education
40
