
Problems of Health Services in the Border Areas and the Efforts to
Overcome
Ratna Dwi Wulandari
Facult
y
o
f
Public Health, Universitas
A
irlan
g
a,
M
ul
y
ore
j
o, Suraba
y
a, Indonesia
Keywords: Health problems in border area, People mobility, Improve health service.
Abstract: Frontier areas have specific characteristics due to the impact of different environmental conditions,
e.g. the distance away from the centre of government and geographical conditions that tend to be
difficult. The easy movement of people from one region to another has an impact on the rapid
transmission of disease. Therefore the health care system in border areas requires specific handling
because it involves two or more districts. This research study was conducted to identify health service
problems in the border areas in East Java, so then a recommendation can be made to improve the
appropriate health service system. This research is a descriptive research study with a cross-sectional
design. The location of the study was in four of the outermost regencies in the East Java Province. The
results of the research indicate that some of the problems identified are the high utilisation of cross-
border health services that has an impact on the incomplete health services provided to the community,
and that there is no inter-region case reporting mechanism. Some efforts that can be undertaken to
improve the health care systems in border areas include developing cooperation for better coordination
in the case of inter-regional population mobility, standardised service procedures and reporting
recording systems, and floating surveillance networks.
1 INTRODUCTION
Indonesia is one of the largest countries in Southeast
Asia, with an area of 5,180,053 km
2
. It consists of a
total land area of 1,922,570 km
2
, and an area of
3,257,483 km
2
of sea, which is divided into 34
provinces. Since 1999 with the enactment of Law
number 22/1999 on Regional Government, and also
Law number 25/1999 on Fiscal Balance between
Central and Regional Governments, the Indonesian
government embraces the decentralisation system by
granting state authority to the district/city
governments.
The government of Indonesia has stipulated that
the implementation of health services in border areas
and isolated, vulnerable and municipal islands is the
duty and responsibility of the district health
authorities. Each district must prepare adequate
health resources in order to be able to properly carry
out the health services in those areas.
People living in rural and remote areas,
including those living in border areas, face
challenges in accessing appropriate health services
(Bourke, et al., 2011). Border areas have their own
problems and peculiarities (Gogoi, et al., 2009). The
public health situation in the border area is actually
similar to other regions, but they have different
characteristics as a result of different environmental
conditions. The environmental conditions that make
the public health situation in the border area
different from elsewhere is related to accessibility.
The border area is a long distance from downtown.
The long distance has several consequences, such as
the number of human resources, the health worker
and health facilities being limited, access to health
care facilities especially secondary and tertiary
health care facilities becoming more difficult, and
the referral time becoming longer. Klobuchar (2014)
state that patients in rural areas with serious
conditions such as heart disease and cancer must
travel longer distances than patients in urban areas to
see specialists. Almost all border areas are in rural,
so this kind of difficulty is also faced by people in
the border areas.
In some areas, the distance or travel time to
another city centre is faster than to the centre of the
city of origin. This causes people to prefer to seek
treatment at health facilities in other districts /cities
that are nearby. Similarly, in the referral process, the
First Level Health Facility (FKTP) prefers to refer
patients to other district / city hospitals.
Community mobility between regions also
affects the public health situation in the border areas.
The easy movement of people from one region to
another has an impact on the rapid transmission of
disease.
Wulandari, R.
Problems of Health Services in the Border Areas and the Efforts to Overcome.
In Proceedings of the 4th Annual Meeting of the Indonesian Health Economics Association (INAHEA 2017), pages 277-281
ISBN: 978-989-758-335-3
Copyright © 2018 by SCITEPRESS – Science and Technology Publications, Lda. All rights reser ved
277

Thus, the public health status in a region is not
only determined by the performance of health
services in the area, but also is strongly influenced
by the situation in other areas, especially the
immediately adjacent areas. Therefore, health
problems in adjacent areas or regions need joint,
integrated and coordinated management by
involving the relevant sectors so that the existing
problems can be resolved optimally.
Health services in border areas require specific
treatment because they involve two or more districts.
Several important issues related to health services in
the border areas are services to the poor, the
continuity of care between different treating
professionals and organisations (Commission Of
The European Communities, 2008), referral health
services, infectious diseases, the adequacy of health
personnel and the handling of outbreaks and
disasters. The spread of infectious diseases does not
recognise geographic region. Many diseases are
transmitted through both animals and humans.
Along with the easier access between, the spread of
diseases between regions is also increasing, for both
old and new diseases. The era of globalisation and
technological progress has also accelerated the
transmission of disease without recognising
geographical and administrative boundaries. Several
diseases which often become a problem because of
the speed their transmission includes TB, Malaria,
AIDS, and other related immunisation diseases
(Kamel, 1997
a
). Kamel (1997
a
) also state that
borders are crucial entry point for communicable
disease which, if it not properly managed, would
affect the community health status.
The previous research by Bourke, et al., (2011)
has develop six key concept as a framework of rural
and remote: (i) geographic isolation, (ii) the rural
locale, (iii) health responses in rural locales, (iv)
broader health systems, (v) broader social structures,
and (vi) power relations at all levels. These six
matters are interrelated in raising public health
issues in the border region. That is why public health
problems in the border area seem more complex
than health problems in other regions. On this basis,
it is important to identify what health problems are
happening in the border areas, as well as what
efforts can be made to strengthen the health care
systems in border areas.
2 METHOD
This research is descriptive because it was done to
obtain the best description of health problems in the
border area, with a cross-sectional design. The data
collection was conducted in 2015 in 4 of the
outermost regencies in the East Java Province;
Ngawi, Bojonegoro, Sumenep and Banyuwangi
districts. The respondents consisted of two groups;
community and health personnel. Communities as
respondents are the people who live in the outer
regions bordering other areas. For each district, 100
community respondents were drawn, so there was a
total of 400 respondents in the 4 cities. Data from
the community was collected by using a structured
questionnaire to describe the utilisation of cross-
border health care facilities. The officers consisted
of a midwife from Polindes in the border area, a
Puskesmas officer in the border area, and staff from
the District Health Office. For the health officer
respondents, data collection was done through a
Focus Group Discussion (FGD). FGDs were
conducted once in each area, so there were 4 repeats
of the FGD. FGDs were conducted to discuss the
findings from the results of the community surveys,
so that further health problems and solutions could
be identified.
3 RESULT AND DISCUSSION
A border area is a meeting area of two or more
regions with different administrative authorities, i.e.
between district and inter-provincial boundaries.
Each region has the authority to regulate its own
territory in accordance with their respective policies
on the basis of the real needs of the community. The
identification of various health problems in the
border areas is important in order to improve the
health care system for people living in there so that
their health status will be better. In addition, good
handling of the health care systems in border areas
can also prevent the expansion of health problems.
The special characteristic often encountered in
the border area is the great distance from the city
centre. The city centre is usually identical to the
central government. Therefore one of the limitations
faced by people living in border areas is that it is
more difficult to access government services located
in the city centre, such as local public hospitals. For
people living in border areas, sometimes access to
health facilities in their area is more difficult due to
the longer distances involved than to other area
health facilities. The impact of this condition is the
occurrence of cross-border health utilisation. This
means that residents of district A go to district B, or
vice versa. Table 1 represent the results of the
INAHEA 2017 - 4th Annual Meeting of the Indonesian Health Economics Association
278
survey of 400 residents living in the border area on
the utilisation of cross-border health facilities.
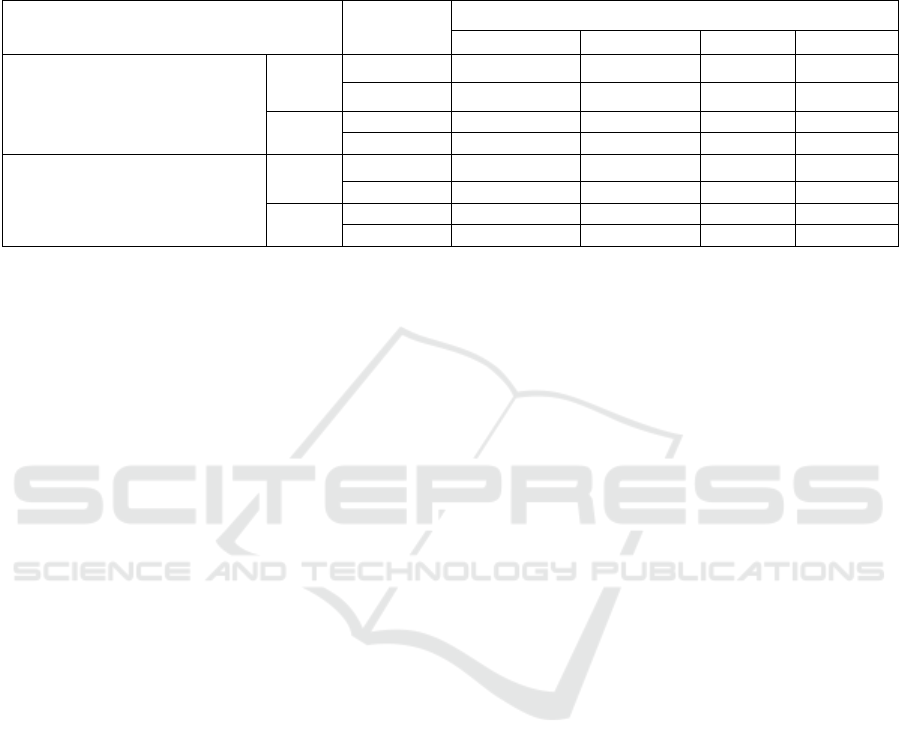
Table 1. Utilisation of cross border health facilities by communities in border areas in the Banyuwangi, Bojonegoro, Ngawi
and Sumenep districts, 2015
Utilisation of cross border health facilities Frequency
District
Ban
y
uwan
g
iBo
j
one
g
oro
Ngawi
Sumene
p
Prefer to seek treatment at health
facilities in other districts
No
n 89 81 6 33
% 89,0 81,0 6,0 33,0
Yes
n 11 19 94 67
% 11,0 19,0 94,0 67,0
People from other areas who
seek treatment at health facilities
in this area
No
n 72 82 55 99
% 72,0 82,0 55,0 99,0
Yes
n 28 18 45 1
% 28,0 18,0 45,0 1,0
Based on Table 1, it can be seen that there are
residents who prefer to seek treatment at health
facilities in other districts, mostly in Ngawi. The
next order is in the Sumenep, Bojonegoro and
Banyuwangi districts. This is because the distance is
closer. For the case of residents from other areas
who seek treatment in other health facilities, this is
the most widely available in the district of Ngawi.
Next is in Banyuwangi, Trenggalek, Bojonegoro and
Sumenep districts. In Ngawi district, people living in
Kendal district are closer to Magetan district with
only about 20 minutes' travel time. Meanwhile,
people living in the Mantingan sub-district are closer
to the Sragen district. For reasons of close proximity
and easier access, this is also the reason why many
Ngawi people are treated in other districts.
The same condition also occurred in Sumenep.
For people living in Pragaan sub-district, they prefer
to go to Pamekasan because it is closer and there is
easier access. In addition, there is a growing image
in Sumenep society that the health service in
Pamekasan is better, mainly because of its more
complete health personnel. This results in the
community going to Puskesmas Pragaan. If referred
to the hospital, they prefer to go to Pamekasan rather
than to Sumenep. As for the Sumenep people who
are in the archipelago, they tend to seek out the
nearest health services. For example, the
examination of Hajj health is closer to the Bali
island than to Sumenep. In Bojonegoro District,
Puskesmas, which borders with the Cepu district,
sometimes prefers to refer patients to hospitals in
Cepu rather than to hospitals in Bojonegoro because
of the proximity to the house. Before Padangan
Hospital was established, 40% of Padangan residents
preferred to go to Cepu. But now the condition is
turning, as the Cepu people prefer treatment at
Padangan Hospital.
The utilisation of cross-border health services, if
not managed properly, will be able to trigger the
emergence of several other problems. One of the
problems that can arise from the movement of these
patients is related to the problem of recording and
reporting health data. Biases on recording data occur
as a result of patents crossing border for hospital or
health care. Biased statistics misrepresent what is
needed and can affect the adequacy of health care
planning and delivery (Kamel, 1997
b
). Important
things for strengthening health services in border
areas are to create and manage mechanisms for
identifying and managing cross-border issues (NHS
Commissioning Board, 2013).
One of the important problems is related to
immunisation. Based on the results of Focus Group
Discussion (FGD) with health personnel in the
Ngawi District, it was found that there were
differences in the determination of immunisation
status between the Ngawi and Sragen regency. For
example, in the Ngawi disctrict, Tetanus Toxoids’
(TT) immunisation status is calculated based on
birth history, whereas in the Sragen regency, every
pregnant mother is given TT immunisation because
all pregnant women need TT.
Another problem identified from the FGD with
health personnel in Ngawi District is the occurrence
of loss control towards high risk pregnant women.
The antenatal care procedure (ANC) of Ngawi
Regency compared to Sragen is different. According
to resource individuals from Ngawi District, the
community considers the ANC service in Ngawi to
be more stringent, in the sense that more checks
have to be done, thus causing certain communities to
prefer ANC in more relaxed areas. In East Java,
Problems of Health Services in the Border Areas and the Efforts to Overcome
279

there is a policy of determining high-risk status by
using the Pudji Rochyati Score Card (In Indonesia:
Kartu Skor Puji Rochyati or KSPR), whereas in
Central Java Province, this does not exist. This is felt
by the people who live directly adjacent to the
Sragen regency who feels that in Sragen, the criteria
are looser. This has resulted in some pregnant
women who initially conducted a medical
examination in Ngawi District to have finally moved
to the Sragen regency. If the mother continues to get
health services in other districts, this makes the
recording continuity of antenatal care services in
Ngawi District disturbed. If this condition occurs in
high-risk pregnant women, it is feared that it could
endanger the health condition of the mother and
foetus, because the new health facility does not have
the history of pregnancy.
The phenomenon above illustrates that one of the
reasons for the change of health service from one
district to another is the patients desire to get a
simpler service procedure. Another reason is related
to the quality of service. The public tends to choose
a place of service which, according to him, is more
qualified, even if the location of the health care
facility is in another district. The results of this study
are in line with previous research that found those
cross-border health users are usually linked to
service quality issues (Rich and Merrick, 2006;
Dejun Su, et al, 2011).
Several other studies have found that the use of
cross-border health services is linked to the cost and
health insurance issues, such as Dejun Su, et al
(2011) and Miller and Thayer (2010). Dejun Su, et al
(2011) in his research at United Stated found that the
most significant predictors of health care utilization
across border were lack of health insurance coverage
and dissatisfaction with the quality of health care.
The results of Miller's study in Mexico also found
the same thing, the utilization of cross-border health
services was triggered by the lack of quality of
service, access difficulties, and low coverage of
health insurance in the region of origin (Miller and
Thayer, 2010).
The third problem is related to the recording and
reporting of health data. The health data recording
and reporting system is hierarchical. Recording and
reporting is done in stages, from the smallest service
unit to the centre. The Puskesmas (Public Health
Center) network consists of Polindes, Ponkesdes,
Puskesmas Pembantu, and other health care facilities
in the Puskesmas working area, reporting the results
of their activities to the Puskesmas. Furthermore, the
Puskesmas reports its data to the District Health
Office/City. District Health Offices conduct
recapitulation and forward the information to the
Provincial Health Office, and then from the
Provincial Health Office to the Ministry of Health.
So its nature is vertical. There is no routine reporting
mechanism that is horizontal (except for certain
cases), such as for Pulmonary TB and Dengue
Fever. As stated by the resource persons from
Sumenep District, TB already has a reporting format
across multiple regions.
To overcome this issue, the government should
ensure that arrangements are in place so that public
health bodies engage populations across the border
in discussions on quality and the changes to the
services provided. This is to ensure that there are
well-defined and clear protocols for managing
changes in where a patient is treated (NHS
Commissioning Board, 2013). Miller and Thayer
(2010) suggest that those problems can be solve
through innovations in cooperation projects on
health, the facilitation of health care access for at-
risk populations, and increased economic
opportunities in health care on both sides of the
border.
4 CONCLUSIONS
Environmental characteristics in the border areas
make these areas face several health problems. Some
of the public health problems occurs in the border
areas are the high population mobility, resulting in
statistical biased related to the recording of patient
health data. The consequences of this situation is
incomplete of monitoring health status that cause in
the emergence of other health problems, such as
misidentification of immunization status and
inaccuracy detection of risk factors for pregnancy,
One important step should be taken to reduce or
prevent the emergence of these problems is to build
cooperation between districts, so there is agreement
between two interdependent areas on the mechanism
of handling cross-border society problems.
ACKNOWLEDGEMENT
This research was supported by Research and
Development Agency of East Java Provincial
Government.
INAHEA 2017 - 4th Annual Meeting of the Indonesian Health Economics Association
280

REFERENCES
Anne, Yazbeck, M., 2016, Study On Cross-Border Health
Services: Potential Obstacles for Healthcare
Providers, European Commission - Erasmus
University, Rotterdam
Bourke, L., Humphreys, J., Wakerman, J., Taylor, J.,
2012, Understanding rural and remote health: A
framework for analysis in Australia, Health & Place,
Elsevier Journal, vol. 18 (496–503)
Commission of The European Communities, 2008, A
Community Framework On The Application Of
Patients' Rights In Cross-Border Healthcare,
Communication From The Commission, Brussels
Dejun Su, Richardson, C., Ming Wen, and Pagan J. A.,
2011, Cross-Border Utilization of Health Care:
Evidence from a Population-Based - Study in South
Texas, Health Research and Educational Trust, 46:3
DOI: 10.1111/j.1475-6773.2010.01220.x
Gogoi, J. K., Goswami, H., Borah, K. C., 2009, Problems
of Border Areas in North East India: Implications for
The Thirteenth Finance Commission, Project Report,
Department of Economics, Dibrugarh University,
Assam
Kamel, W. W., 1997
a
, Health in Borders Area, Global
Perspectives in Health – Vol 2, Tempe, Arizona
Kamel, W. W., 1997
b
, Health Dilemmas at the border – a
global challenge, World Health Forum, vol. 18 (9-16)
Klobuchair, A., 2014, Keeping Rural Communities
Healthy, Joint Economic Committee, United States
Miller, J., Thayer, 2010, Health Migration: Crossing
Borders for Affordable Health Care, Field Actions
Science Reports [Online], Special Issue 2 | 2010,
Online since 01 October 2010, connection on 30
September 2016. URL : http://factsreports.revues.org/
503
NHS Commissioning Board, 2013, Protocol for Cross-
Border Healthcare Services, Government regulation,
Department for Health and Social Services of the
Welsh Government
Rich, F. R., Merrick, K., R., 2007, Cross Border Health
Care in the European Union: Challenges and
Opportunities, 23 J. Contemp. Health L. & Pol'y 64
(2007), Available at: http://scholarship.law.edu/jchlp/
vol23/iss1/4
Problems of Health Services in the Border Areas and the Efforts to Overcome
281
