
A Left-Right-Asymmetric Pedaling Machine for Medical
Rehabilitation of Lower Limbs
Milun Liu
1
, Fajian Wu
1
, Jinhua She
1, 2, 3
, Hiroshi Hashimoto
4
and Min Wu
2, 3
1
Graduate School of Bionics, Computer and Media Sciences, Tokyo University of Technology,
Hachioji, Tokyo 192-0982, Japan
2
School of Automation, China University of Geosciences, Wuhan, Hubei 430074, China
3
Hubei Key Laboratory of Advanced Control and Intelligent Automation for Complex Systems,
Wuhan, Hubei 430074, China
4
Master Program of Innovation for Design & Engineering, Advanced Institute of Industrial Technology Shinagawa-ku,
Tokyo 140-0011, Japan
Keywords: EMG Sensor, Left-Right Asymmetry, Lower-Limb Rehabilitation, Human Centered, Pedaling Machine.
Abstract: This paper explains a pedaling machine of a left-right-asymmetric type for lower-limb rehabilitation. Since
most commercially available machines for the rehabilitation of lower limbs are symmetric, people with
lower-limb injuries have to adapt themselves to the machines to do exercises. To solve this problem, we
have been developing a new kind of pedaling machine that can easily be used to adapt the requirements for
left-right asymmetry of lower limbs. Main points in the design of a prototype of a half model for one leg of
the machine are summarized. Preliminary tests with a tread force sensor and some electromyogram (EMG)
sensors are carried out and are showed the feasibility of the machine.
1 INTRODUCTION
Maintaining or improving walking ability is
essential to ensure a person’s mental and physical
soundness. However, many people cannot walk
normally due to diseases and/or injuries of lower
limbs, brain damage, or aging. Lower-limb
rehabilitation is an important way to regain the
ability of walking. According to statistics, the
number of people in Japan who are issued a
certification of needed long-term care or a
certification of needed support has been rapidly
increasing in the last decade, and the number of
people was 5.457 million in 2012 (Ministry of
Health, Labour and Welfare, Japan, 2016). As
shown in the same report, there will be more than
one third of the Japanese to become the elderly in
2035. A large number of people who need
rehabilitation will cost large manpower to take care
of them. And the increasing number of people who
need rehabilitation will become to a serious social
problem in the near future. So, developing
rehabilitation machines to help people to train their
walking muscles not only has a positive influence on
people’s physiology and psychology, but also
contributes to the whole society.
Nowadays, a great number of rehabilitation
machines, which are mainly remodelled from
training machines, are often used in rehabilitation.
However, those machines have some problems, such
as bisymmetric pedaling, fixed structure of machines
(for example, Anzai, 2014). Since all those machines
are machine-centered, they are hard to meet all kinds
of requirements of users for the rehabilitation of
lower limbs. They not only may lead to tremendous
pain for users, but also may lead to the degradation
of motivation for rehabilitation. In order to solve
above problems, it is necessary to develop a truly
effective machine for rehabilitation.
Riding a bicycle is effective to train walking
muscles, but it is not suitable for a user with lower-
limb injury. To complete a training task, a user with
different degrees of damage in left and right legs
subconsciously uses the powerful leg with a great
effort. This causes great inadequacy in rehabilitation.
We designed a new type of an asymmetric
pedaling machine for lower-limb rehabilitation and
built a prototype of a half model for one leg to solve
the above mentioned problems (She et al., 2016,
2017a, 2017b). Unlike other ones, it is a human-
652
Liu, M., Wu, F., She, J., Hashimoto, H. and Wu, M.
A Left-Right-Asymmetric Pedaling Machine for Medical Rehabilitation of Lower Limbs.
DOI: 10.5220/0006471306520657
In Proceedings of the 14th International Conference on Informatics in Control, Automation and Robotics (ICINCO 2017) - Volume 1, pages 652-657
ISBN: 978-989-758-263-9
Copyright © 2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
centered machine that the structure of the machine is
easy to be adjusted to suit the different requirements
for the lower-limb injuries. The left and right
pedaling loads and strokes can also be adjusted
independently. In order to obtain information about
rehabilitation, we built a measuring system to carry
out the interaction between exercises and the
computer-based supervision (She et al., 2017a).
This paper summarizes the main points in the
design of the machine. The results of preliminary
tests using a force sensor and some electromyogram
(EMG) sensors are presented to show the validity of
the pedaling machine for lower-limb rehabilitation.
2 KEY POINTS IN DESIGN OF
ASYMMETRIC PEDALING
MACHINE
Pedaling is widely used in training the walking
muscles. There are basically two kinds of pedaling:
rotational and linear. Since a linear type can easily
be used to design a left-right-asymmetrical
mechanism, we used it to build a new type of a
pedaling
machine to suit different requirements for
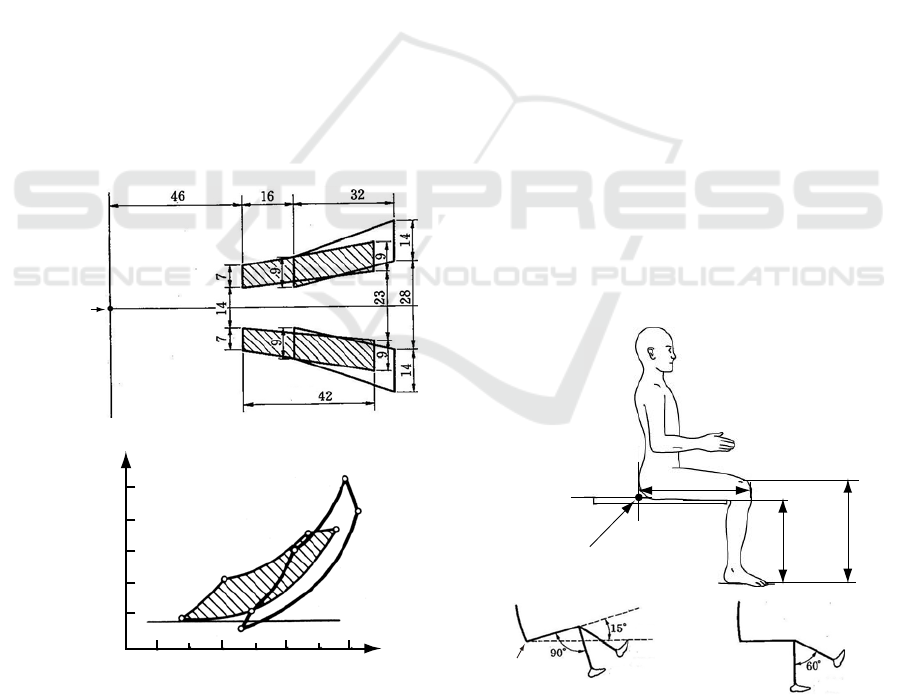
Figure 1: Optimal pedaling region. (a) Top view and (b)
Side view (Upper case: heel; lower case: toe) (Sato, 1994;
She et al., 2017b).
lower-limb injuries.
To design a pedaling machine, first, we need to
determine the specifications of the mechanism.
As the first step, we selected a pedaling load for
a leg-extension force. According to Sato (1994), the
maximum of the average leg-extension force of one
leg for 20-year-old man is about 2900 N. It
decreases with aging from 20s, and the force of
people in 60s is only about 50% of that of their 20s.
Considering that people who need rehabilitation
have very weak legs, we chose the maximum
pedaling load to be
N. 2000
max
P
(1)
Then, we determined the range of an adjusting
angle for the pedaling machine. There is an optimal
pedaling region for a normal person (Figure 1), and
the definitions are given in Figure 2. The angle
between the femur and the lower leg is in the range
[15
o
, 90
o
] when the knee is at the closest position to
the body, and [30
o
, 90
o
] when the knee at the farthest
position from the body. Considering that a person
who needs rehabilitation may not sit and/or pedal as
a normal person does, we chose the angle to be
]90 ,0[
(2)
so that it can provides a larger region than the
optimal one does to satisfy the different
requirements for users. Based on a preliminary test,
we chose the length of stroke of the linear pedaling
mechanism to be
mm. 150
L
(3)
Figure 2: Definitions (Sato, 1994; She et al., 2017b).
Max:
Max:
Seat reference
point
a
d
b
e
A
B
E
D
Distance forward of
seat reference point [cm]
Distance below
seat reference point [cm]
Floor
(a)
(b)
Height of
knee
Hip-knee
distance
Seat reference
point
Height of
seat
Horizontal line
Near high point
Near low point
Far high poin
t
Far low point
Seat reference
point
A Left-Right-Asymmetric Pedaling Machine for Medical Rehabilitation of Lower Limbs
653
Lef
t
lateral view Frontal view Photo (
r
igh
t
lateral view)
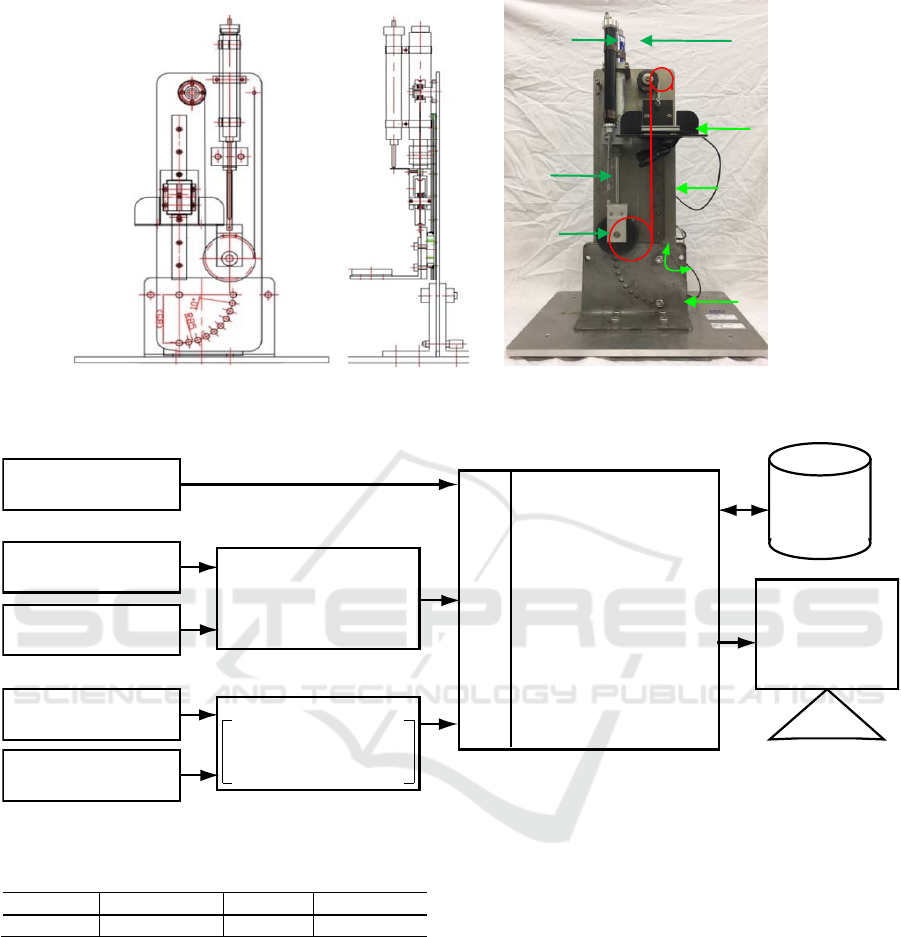
Figure 3: Prototype of pedaling machine for one leg.
Figure 4: Measuring system (She et al., 2017).
Table 1: Parameters of oil damper, KINECHECK Super K.
Model Overall len
g
th Stroke Force ran
g
e
5001-31-4 356 mm 102 mm 23 ~ 5440 N
2 PEDALING MACHINE AND
MEASURING SYSTEM
We selected components to build a pedaling
machine that satisfies (1)-(3).
An oil damper, KINECHECK Super K (Meiyu
Aimatic Co. Ltd., Japan) (Table 1), was selected to
produce a pedaling load. It has the longest stroke
and produces the largest damping force in small-size
oil dampers. The maximum force is more than twice
of
max
P
in (1), but the stroke is about half of
L
in
(3). So, we designed a pulley mechanism to enlarge
the stroke two times and to reduce the force to half.
A prototype of the machine for one leg was built
(Figure 3). And an inclined angle of the adjusting
part was designed to be changed from 0
o
to 90
o
to
ensure (2).
As shown in Figure 3, an inclined panel is fixed
to the base by two bolts. The angle from 0
o
to 90
o
is
equally divided by 10
o
. Resetting and fastening the
bolt turn the inclined panel at a desired angle to suit
a user’s need. The pedal is directly connected to the
oil damper by a steel-wire rope in a pulley
mechanism. The pedaling force is manually adjusted
by turning a nob on the oil damper. The user pushes
Tread force sensor
(LPR-C-1KNS15)
Displacement sensor
(DTS-A-100)
Heart rate meter
(neo HR-40)
Compact recording system
(EDX-10A)
Wireless EMG sensor
(SX230-1000)
9-axes wireless
motion sensor
Wireless set
Transmitter (PH8310)
Amplifier (PH8320)
Data receiver (PH8020)
Data base
Interface
PC
(Windows 8.1)
Display
Hinge joint
Displacement
sensor
Oil damper
Pedal
Pulley
mechanism
Guide rail
Inclined
panel
Base
Adjusting bolt
ICINCO 2017 - 14th International Conference on Informatics in Control, Automation and Robotics
654
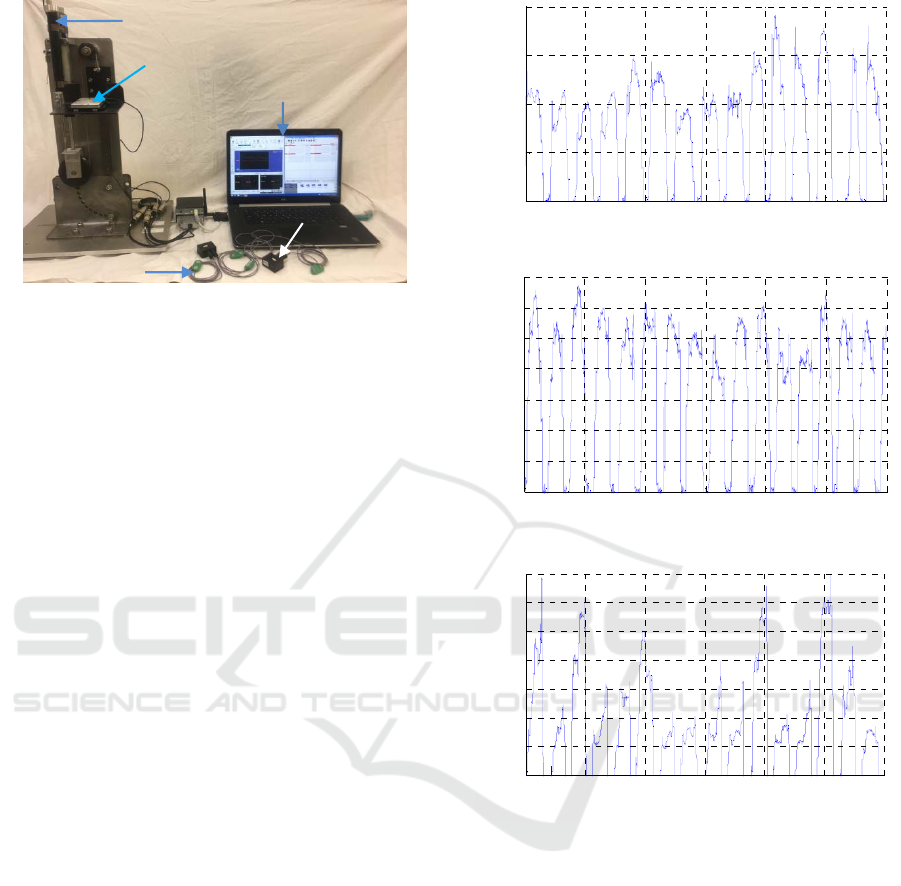
Figure 5: A photo of components of measuring system.
the pedal down in a linear motion for exercise. The
pedal returns back to the up position by elasticity
produced by the oil damper.
The following points are considered in the
design of the measuring system:
It suitably stores measured data in a real-time
fashion.
It ensures easy access to measured data.
It displays measured data in a real-time
fashion, and easily switches the display to
interested data.
It is easy to synchronize data if needed.
A measuring system (Figures 4 and 5) was
constructed to collect data. The measuring system
consists of a heart rate meter (neo Hr-40) (NISSEI
Co. Ltd., Japan), a force sensor (LPR-C-1KNS15)
and a displacement sensor (DTS-A-100) (Kyowa
Electronic Instruments Co. Ltd., Japan), one set of
wireless EMG sensor (SX230-1000) and one set of
9-axes wireless motion sensor (XYZ geomagnetism,
XYZ acceleration, and XYZ angular acceleration)
(DKH, Japan).
The measuring system ensures the possibility of
interaction between exercises and computer-based
supervision and control of medical rehabilitation.
3 PRELIMINARY TESTS
Preliminary tests were carried out for the prototype
for three subjects. A subject sat on a fixed chair in
front of the prototype machine with a determined
distance. The inclined angle was set to be 20°, 50°,
and 70°; and the pedaling force was set from 0 to 60
N.
It was found that pedaling was carried out
smoothly and comfortably for the inclined angle of
50° among the three setting of 20°, 50°, and 70°.
(a)
(b)
(c)
Figure 6: Pedaling force for different inclined angles
[inclined angle: (a) 20º, (b) 50º, and (c) 70º].
Some typical time responses of pedaling force for
different inclined angles are shown in Figure 6. As
can be seen from the figure, the variation of the
pedaling force is the smallest for the inclined angle
of 50º among the three angles. This shows that it
was the easiest position for the user who pedaled the
machine, and it also shows that adjusting the
inclined angle of the pedaling machine can easily
satisfy the needs of individual requirements.
The muscles of quadriceps femoris, biceps
femoris, tibialis anterior, and soleus (Figures 7 and
8) are most closely related to walking. They were
measured in preliminary tests. The EMG signals of
those muscles were recorded.
0 10 20 30 40 50 60
0
20
40
60
80
Time [s]
Force [N]
0 10 20 30 40 50 60
0
10
20
30
40
50
60
70
Time [s]
Force [N]
0 10 20 30 40 50 60
0
10
20
30
40
50
60
70
Time [s]
Force [N]
Displacement sensor
Force sensor
Measuring screen
(PC)
EMG sensor
Wireless module
A Left-Right-Asymmetric Pedaling Machine for Medical Rehabilitation of Lower Limbs
655
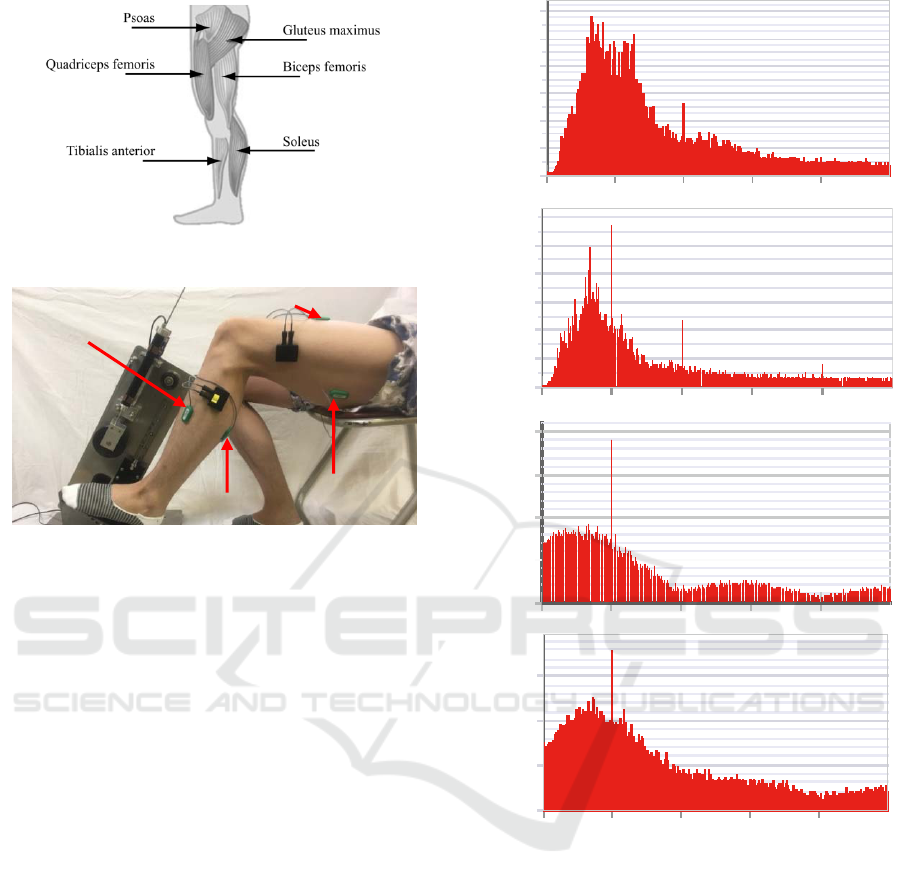
Figure 7: Walking muscles (She et al., 2006).
Figure 8: A photo of preliminary test with EMG sensor.
Since the characteristics of the EMG signals can
mainly be observed in the frequency range of 50-150
Hz (Marras, 1992; De Luca, 2002), we chose the
sampling frequency to be 500 Hz. The FFT (fast
Fourier transformation) was used to those signals
(Figure 9). The figure shows that the EMG signals
were recorded properly.
On the other hand, as pointed out by Carlo J. De
Luca (2002), the amplitudes of the EMG signals are
stochastic (random) in nature, and can be reasonably
represented by a Gaussian distribution function. The
usable energy of the signal is in the frequency range
of [0, 200] Hz, with the dominant energy in the
range of [50, 100] Hz. The usable signals are viewed
as those with energy above the electrical noise level.
The noise is usually inherent noise in the electronics
components in the detection and recording
equipment, ambient noise, motion artifacts, and
inherent instability of the signal. The amplitude of
an ambient noise may be one to three times larger
than that of the EMG signals. It is clear from Figure
9 that big amplitudes of spectra at 50 Hz, 100 Hz,
and 200 Hz are considered to be the power noise and
its harmonics. How to abstract true characteristics of
the pedaling motion from the noisy EMG signals is
one of the main tasks in this study, and will be
investigated in the near future.
Figure 9: EMG signals of for Load 5 (60 N) and inclined
angle of 50º.
4 CONCLUSION
A left-right-asymmetric rehabilitation machine and a
measuring system were designed and used in this
study. Some preliminary tests showed that this
machine was suitable for people carrying out
exercise for their walking muscles, and was able to
answer the needs for people with lower-limb
asymmetry.
On the other hand, preliminary tests also showed
that, while the stroke was long enough for exercise,
the maximum pedaling load (1) was too large.
Experiments showed that setting the maximum
0
0.0002
0.0004
0.0006
0.0008
0.0010
0.0012
0
50 100 150 200
Amplitude spectrum
(Quadriceps femoris)
[Hz]
0
0.0001
0.0002
0.0003
0.0004
0.0005
0.0006
0 50 100 150 200
[Hz]
Amplitude spectrum
(Biceps femoris)
Amplitude spectrum
(Tibialis anterior)
0.0020
0.0015
0.0010
0.0005
0
0 50 100 150 200 [Hz]
0
0.0005
0.0015
0 50 100 150 200
Amplitude spectrum
(Soleus)
[Hz]
0.0010
Biceps femoris
Soleus
Tibialis anterior
Quadriceps femoris
ICINCO 2017 - 14th International Conference on Informatics in Control, Automation and Robotics
656

pedaling load to be 200 N would be large enough for
rehabilitation. The part of load generation is planned
to be rebuilt in the near future.
To further verify the practicability of the
asymmetric pealing machine, we plan to test various
normal subjects for the comparison of individual
differences (males and females). Then we will
analysis the collected data and try to find a way to
carry out the control of medical rehabilitation. The
performance indexes used in (Smak et al., 1999;
Carpes et al., 2010) will be integrated to evaluate the
left-right-asymmetry and the effectiveness of
pedaling for rehabilitation.
ACKNOWLEDGEMENTS
The authors would like to thank Dr. Wangyong He
and Mr. Qi Shi for their contribution in this study.
This work was supported by Japan Society for the
Promotion of Science (JSPS) KAKENHI under
Grants 26350673 and 16H02883, by the National
Natural Science Foundation of China under Grants
61473313 and 61210011, by the Hubei Provincial
Natural Science Foundation of China under Grant
2015CFA010, and by the 111 Project, China under
Grant B17040.
REFERENCES
S. Anzai, 2014. Healthy Cycle: A Leg-Powered
Wheelchair from Japan Is Motivating the Disabled,
Highlighting Japan, no. 11, pp. 20-21. Available:
http://dwl.gov-online.go.jp/video/cao/dl/public_html/
gov/pdf/hlj/20141101/20-21.pdf
F. P. Carpes, C. B. Mota, and I. E. Faria, 2010. On the
bilateral asymmetry during running and cycling –--A
review considering leg preference, Physical Therapy
in Sport, no. 11, pp. 136-142.
C. J. De Luca, 2002. Surface Electromyography:
Detection and Recording, DelSys Incorporated,
Available: https://www.delsys.com/Attachments_pdf/
WP_SEMGintro.pdf
W. Marras, 1992. Selected Topics in Surface
Electromyography for Use in The Occupational
Setting: Expert Perspectives, U.S. Department of
Health and Human Services Public Health Service
Centers for Disease Control National Institute for
Occupational Safety and Health.
Ministry of Health, Labour and Welfare, Japan, 2016.
Annual Report on the Aging Society, Available:
http://www8.cao.go.jp/kourei/whitepaper/w-2015/
html/zenbun/s1_2_3.html (in Japanese), http://
www8.cao.go.jp/kourei/english/annualreport/2014/201
4pdf_e.html (in English)
M. Sato, 1994. Ningen Kougaku Kijun Suuchi Suushiki
Benran (Handbook of ergonomic standards, numerical
values, and formulas), Tokyo: Gihodo Shuppan Co.,
Ltd.
J. She, Y. Ohyama, and H. Kobayashi, 2006. Master-Slave
Electric Cart Control System for
Maintaining/Improving Physical Strength, IEEE Trans.
Robot., vol. 22, no. 3, pp. 481-490.
J. She, F. Wu, T. Mita, H. Hashimoto, and M. Wu, 2016.
Design of a New Human-Centered Rehabilitation Ma-
chine, Proc. 9th ACM Int. Conf. Pervasive
Technologies Related to Assistive Environments
(PETRA 2016), doi: 10.1145/2910674.2910684, Corfe,
Greece.
J. She, F. Wu, H. Hashimoto, T. Mita, and M. Wu, 2017a.
Design of a Bilaterally Asymmetric pedaling Machine
and its Measuring System for Medical Rehabilitation,
Proc. 1st Int. Conf. on Human Computer Interaction
Theory and Applications (HUCAPP 2017), Porto,
Portugal.
J. She, F. Wu, T. Mita, H. Hashimoto, M. Wu, and A. M.
Iliyasu, 2017b. Design of a New Lower-Limb
Rehabilitation Machine, Journal of Advanced
Computational Intelligence and Intelligent Informatics,
vol. 21, no. 3, pp. 409-416.
W. Smak, R. R. Neptune, and M. L. Hull, 1999. The
influence of pedaling rate on bilateral asymmetry in
cycling, J. Biomechanics, vol. 32, pp. 899-906.
A Left-Right-Asymmetric Pedaling Machine for Medical Rehabilitation of Lower Limbs
657
