
Improving Healthcare through Human City Interaction
Tim Woolliscroft
1
and Simon Polovina
2
1
Sheffield Business School, Business Operation Systems, Sheffield Hallam University, Sheffield, U.K.
2
Conceptual Structures Research Group, Communication and Computing Research Centre, Cultural Communication and
Computing Research Institute (C3RI)| Department of Computing, Sheffield Hallam University, Sheffield, U.K.
Keywords:
Agents, Cyber-physical Systems, Healthcare, Human City Interaction, Human Computer Interaction, Internet
of Things, Smart Cities, Smart Communities, Structuration Theory.
Abstract:
The study of information technology has given insufficient focus to a) the structural factors and b) the com-
munity perspective. As information systems become increasingly integrated with human systems these wider
influences are more important than ever. Human city interaction concepts including their interplay with cyber-
physical systems and social computing are appropriated to healthcare. Through Structuration Theory, insights
are given into how healthcare through the human city interaction lens can most effectively be improved.
1 INTRODUCTION
This paper explores how the concept of human com-
puter interaction and its notions of social comput-
ing and cyber-physical systems can improve the ef-
ficiency of healthcare. Human city interaction moves
the conceptual basis of human computer interaction
from the micro, individual user scale towards a macro,
city wide scale. As such it can also impact healthcare
practices given they are inherently community-based.
As NHS digitisation continues to meet resistance,
we argue that greater focus needs to be given to the
social aspects involved. Indeed, two-thirds of poten-
tial health information systems have not yet materi-
alised (House of Commons, 2013; Waterson, 2014).
We postulate that a greater focus on the structural fac-
tors might have had a different result.
The paper is laid out as follows: Structuration
Theory is used to appropriate human city interaction
concepts to healthcare. Based on this approach, the
human social challenges are highlighted and the re-
search gap addressed including the system design is-
sues. The paper concludes with the insights that hu-
man city interaction can bring to improving health-
care.
2 STRUCTURATION
Structuration Theory is a theory of agency and struc-
ture to help understand how people behave (Giddens,
1984). Agency and structure is the extent to which
people are free independent agents or are agents
whose behaviour is socially determined. Structuration
Theory emphasises the role of everyday social prac-
tice in consistently recreating social structure (Jones
and Karsten, 2008). Structuration Theory is often ar-
gued as relevant to dealing with ‘wicked’ unstructured
problems in the public sector (van Veenstra et al.,
2014).
Structuration Theory has frequently been applied
to information systems research to help understand
the relationship between information systems and
the people using them including the surrounding so-
cial context and social processes (Jones and Karsten,
2008; Checkland and Holwell, 1997). The need for
this approach is evident from the seismic impact that
information technology is already having on human
computer interaction by extending it beyond individ-
ual users interacting with individual computers to-
wards interaction between many people and many
computers across the internet.
3 HUMAN CITY INTERACTION
The idea of human city interaction emerges from
smart cities literature, connecting it to cyber-physical
systems and the internet of things (Naphade et al.,
2011; Jin et al., 2014). Human city interaction is
distinct from the idea of the smart city, in that the
smart city describes the urban environment whereas
172
Woolliscroft, T. and Polovina, S.
Improving Healthcare through Human City Interaction.
DOI: 10.5220/0006368401720177
In Proceedings of the 19th International Conference on Enterprise Information Systems (ICEIS 2017) - Volume 3, pages 172-177
ISBN: 978-989-758-249-3
Copyright © 2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

we define the concept of human city interaction as the
complex web of human computer interaction in the
smart city environment. Smartness is proportional to
the increased awareness that these digital technolo-
gies bring in as they extract this information from the
physical environment (Gurgen et al., 2013). Human
city interaction emphasises the complex web of hu-
man computer interaction in the smart city environ-
ment. Over the next few subsections we outline sev-
eral key important concepts the building blocks of hu-
man city interaction and its relevance to healthcare.
3.1 Smart Communities
A smart community brings together the interplay of
the cyber, physical, and social worlds; within this en-
vironment humans and physical things will interact
with each other through ubiquitous networks (Xia and
Ma, 2011). The combination of a focus on human in-
teractions and a connection with cyber-physical sys-
tems connects the concept of human city interaction
with the concept of smart community (Li et al., 2011;
Xia and Ma, 2011). These communities are also con-
nected with social computing and finding solutions to
societal problems including healthcare.
3.2 Social Computing
Social computing includes human social dynamics
connected to ICT technologies, with theoretical un-
derpinnings in both computational and social sciences
(Wang et al., 2007). Although the idea is usually as-
sociated with social media the origin of the term can
be traced back to the 1940’s to a paper by Vannevar
Bush that predicted many changes that have now be-
come reality, such as computer-supported collabora-
tion (Wang et al., 2007). There are specific exam-
ples of some of the components of social computing
including blogs, wikis, social bookmarking, peer-to-
peer networks, open source communities, photo and
video sharing communities, and online business net-
works (Parameswaran and Whinston, 2007). Social
computing is shifting computing to the edge of the
network where individuals with relatively low techni-
cal skills can apply their creativity and work collec-
tively with others (Wang et al., 2007; Parameswaran
and Whinston, 2007).
3.3 Web 2.0
Definitions of Web 2.0 are very similar to that of so-
cial computing. Both emphasise collaboration and
the ability of users to interact with each other. Web
2.0 includes features that enable collaboration includ-
ing well-known examples such as wikis and blogs
(Aghaei et al., 2012). The collaborative nature of
Web 2.0 has been emphasised by the phrase pro-
sumers, which emphasises that users of 2.0 are both
consumers of it and producers of it (Lupton, 2015).
The key difference between Web 2.0 and social com-
puting however is the emergence of terms including
Web 3.0 and Web 4.0. As such, Web 2.0 is becoming
associated with a point in time that we are moving
beyond (Aghaei et al., 2012).
3.4 Medicine 2.0 and Health 2.0
The terms Medicine 2.0 and Health 2.0 have been
coined to describe the application of Web 2.0 to the
healthcare arena. Some however have gone further
than this and suggest a movement towards a different
more equal relationship between patients and health-
care professionals (Bos et al., 2008). Given the col-
laborative nature of the Web’s evolution, information
technology will change healthcare significantly; Web
2.0 technology in the form of Medicine 2.0 will im-
pact on all areas of medical practice (Hughes et al.,
2008). Similarly, Health 2.0 is shaping health care
with Web 2.0 tools with the result being a whole new
way of involving consumers in the health care system
including the transition towards participatory health-
care (Belt et al., 2010; Bos et al., 2008). Collabora-
tion, participation, openness and change are common
themes in the Health 2.0 literature (Belt et al., 2010;
Eysenbach, 2008). These ideas of collaboration and
change are key components of effective human city
interaction.
3.5 Collaborative Intelligence
Collaboration is a central theme in social computing,
Web 2.0 and Medicine 2.0 literature. The term collab-
orative intelligence however builds on this and sug-
gests a shift into a deeper form of collaboration that is
often referred to as collective or collaborative intelli-
gence. Collaborative intelligence has the potential to
result in positive change, extending into a claim that
mass collaboration changes everything (Tapscott and
Williams, 2008).
3.6 Collective Intelligence
There is a subtle distinction between collective or col-
laborative intelligence. Collaborative intelligence is a
system where each person or machine interacts au-
tonomously as part of decision making network. Col-
lective intelligence takes this idea a step further with
Improving Healthcare through Human City Interaction
173

a shift in power from the individual to the collec-
tive. Collective intelligence is not a new idea, but
it has received a new meaning through the emer-
gence of Web 2.0 applications (Leimeister, 2010).
This new meaning depicts the ability for people digi-
tally connected by the internet collectively to create
knowledge. There have been instances of amateur
knowledge surpassing professional knowledge, and
Wikipedia is given as the most recognised example of
this (Surowiecki, 2005; Boulos and Wheeler, 2007).
In relation to healthcare, collective intelligence
can improve evidence based medicine by drawing
on a larger knowledge base (Tapscott and Williams,
2008). Online networks enrich and contextu-
alise health information and reduce misinformation
(Aghaei et al., 2012; Boulos and Wheeler, 2007;
Hughes et al., 2008). Similarly, collective intelli-
gence might be the solution to concerns about health
information quality. As thousands of bloggers ex-
change ideas daily they are effectively acting as filters
for information-overloaded Web surfers (Boulos and
Wheeler, 2007).
Mass participation is central to the ideas of social
computing and collective intelligence. This assump-
tion is however subject to criticism. In reality only a
small proportion of users may actually be active pro-
ducers (Dijck and Nieborg, 2009). Also, mass partic-
ipation must ensure that the individual is not hypno-
tised by the crowd (Le Bon, 1897).
3.7 Web 4.0
The Web is evolving far beyond Web 2.0 to Web 4.0
(Aghaei et al., 2012; Patel, 2013; Choudhury, 2014).
Web 4.0 is described as the symbiotic Web in which
the human mind and machines can interact symbiot-
ically, including Medicine 4.0 and its links to human
city interaction (Choudhury, 2014; Naphade et al.,
2011; Roche and Rajabifard, 2012).
4 HUMAN-SOCIAL CHALLENGE
Certain social system problems are ill formulated,
have many different clients or agencies with conflict-
ing values, and have been referred to as ‘wicked prob-
lems’ (Churchman, 1967; Rittel and Webber, 1973).
Health services (in particular cancer services) are
such a wicked problem (Ferlie, 2013). Human city
interaction and its interplay with cyber-physical sys-
tems realises the collaborative user interactions that
are similarly of benefit to healthcare (Xia and Ma,
2011; Cockerham, 2005). The wicked problems how-
ever present number of human social challenges that
can be usefully considered by referring to the theory
of structurisation that we met earlier.
4.1 Structuration and Wicked Problems
Structuration Theory connects directly to the idea
of addressing wicked problems (van Veenstra et al.,
2014). Structuation uses the term routinization to de-
scribe the idea of structure being continuously pro-
duced and reproduced through action. Through re-
peated actions a social order is established and certain
patterns of behaviour and ways of engaging in tasks
become institutionalised (Giddens, 1984). From rou-
tinization in healthcare we might conclude that there
are necessary structural constraints upon both patients
and professionals that might be preventing them from
moving towards a perfectly collaborative position.
Medicine 2.0 introduced the idea of including
patients and professionals working more closely to-
gether, but routinization may still be evident in the
cyber-physical models of healthcare. It has been as-
sumed that patients will simply behave as required for
the efficiency gains from healthcare cyber-physical
systems to be achieved (Broy et al., 2012). How-
ever, for the efficiency to be harnessed a wide variety
of complex social factors need to be considered in-
cluding psychological factors linked to human inter-
actions and lifestyle habits that have developed over
time. This assertion is supported elsewhere, as health
lifestyles are not the uncoordinated behaviours of dis-
connected individuals, but are routines linked to inter-
actions within groups (Cockerham, 2005).
After IT systems have been adopted, they need to
be assimilated to change existing work practices. Un-
til this has happened productivity may decline and if
innovation is not successfully assimilated they could
be worse off as previous successful routines will have
been lost (Setia et al., 2011). Further support arises
from social constraints, both in relation to cyber-
physical systems and IT artefacts that are shaped
by messy processes. Rather they are influenced by
the social system they are embedded in. Further-
more cyber-physical systems are particularly uncon-
trollable due to feed- back loops and the behaviour
of some parts of the system being difficult to predict
(Beverungen, 2013).
Perhaps more significant than the issue of integrat-
ing patients into a new health system based on human
city interaction are the cultural factors that impact
on the behaviour of healthcare professionals. Resis-
tance to change and conformity to routinization may
emerge from the desire to hang onto power and sta-
tus linked to current structures, reinforced by the per-
ception that change is just part of the government’s
ICEIS 2017 - 19th International Conference on Enterprise Information Systems
174

agenda to cut services or it might be based on uncon-
scious ideas about how things have always been done.
5 ADDRESSING THE GAP
Failure to consider wider structural factors in infor-
mation technology, health and health economics re-
search is far from superficial oversight. This goes
right to the heart of the philosophical assumptions of
most researchers in these fields. Health economics
has remained insulated from theoretical debates that
have taken place in other areas of the social sciences
(Rickles et al., 2007; Lessard, 2007; Giddings, 2006).
Helpfully though, Structuration Theory has been in-
terrelated with other approaches, including a useful
study where this theory meets actor-network theory
(Greenhalgh and Stones, 2010).
Whatever the merits and demerits of the various
approaches, in the realm of healthcare technology
there is rarely sufficient consideration of social con-
text. As we’ve previously stated, information tech-
nology has evolved far beyond a system of individ-
ual people interacting with individual computers; it
is now increasingly a complex Web of many peo-
ple interacting with a complex Web of digital devices
through the internet. Structuration Theory and hu-
man city interaction at least provides a fulcrum for
improving healthcare given its community-oriented
approach. Human agent collectives are described
as systems where people routinely collaborate with
autonomous software (Jennings et al., 2014). That
work highlights flexible social interactions between
humans and the computers as they engage in synergis-
tic human computer collaboration, neatly fitting with
the idea of human city interaction. This area how-
ever has also been under-researched; although some
research domains are beginning to explore aspects of
this area, none are dealing with it in its totality (Jen-
nings et al., 2014). Perhaps the time to emphasise
the community context in human-computer interac-
tion and the consequent effects on the associated tech-
nologies as we have described has arrived.
5.1 Design Issues
Human city interaction raises the challenge of influ-
encing human behaviour and the use of design as a
tool (Naphade et al., 2011). Given that human city
interaction includes a complex Web of interactions
between people as well as machines, system design
in this area is not straightforward. Most current sys-
tems assume altruistic and benevolent behaviour from
users and fail to consider behavioural issues such as
the need to provide other pertinent aspects such as in-
centives in a collective context (Jennings et al., 2014).
The ethical issue of accountability also emerges from
the fact that the systems at times instruct us and at
other times are instructed by us, thus heightening the
potential tension between the human and computer
agents in the collective (Jennings et al., 2014). Enter-
prise Architecture however might be a useful frame-
work to help overcome some of these design chal-
lenges. It offers a perspective that holistically brings
together the myriad human and technological agents
needed to fulfil the collective purpose of the city,
including its provision of healthcare (van der Weel,
2017).
In linking the ideas of design to Structuration The-
ory for healthcare efficiency the process of design
needs to be applied akin to the complex web of city
structures. As people are as much the fabric of a city
as the technology, a change programme would involve
the people in designing the information technology
rather than changing peoples’ behaviour to fit it. At
the same time, at a higher layer of conceptualisation
the people as well as the technology should be con-
sidered as components that need to be factored into
the system design.
Our approach is represented in Figure 1. Essen-
tially, this figure depicts the concepts and their direct
and indirect relationships from human city interaction
to improving healthcare.
6 CONCLUSION
The appropriation of human city interaction to health-
care could improve its efficiency. Ideally, it would
address the present healthcare information systems
failures as illustrated at the beginning of this paper
(House of Commons, 2013; Waterson, 2014). It is not
however that simple and difficulties can be expected
along the way. Introducing the technology that could
enable the improvements as we’ve described are as
likely to reduce efficiency as to increase it especially
at least in the short term. At least as much attention is
needed in creating the human conditions as the tech-
nology.
Social theory including Structuration Theory as
we have highlighted can highlight the social issues
that need to be considered to achieve the necessary
efficiency improvements. The ideas of routinization
and structural influences contained within Structura-
tion Theory we suggest contain insights that can make
efficiency improvement more likely. In short, greater
consideration of the structural factors that impact on
how people interact with each other and with the com-
Improving Healthcare through Human City Interaction
175
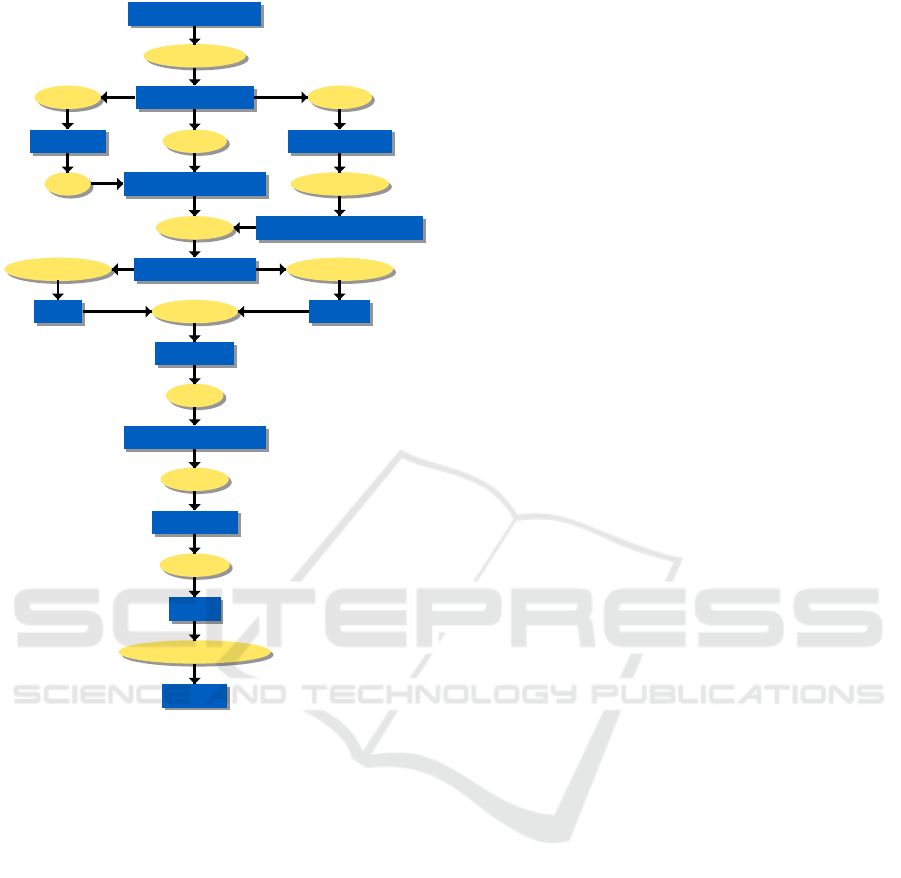
rely−on
Web/Medicine/Health: 2.0−4.0
presents
Smart Cities
situated−in
manifested−by
applied−by
Smart Communities
Social Computing
Cyber−Physical Systems
characterised−by
is−component−of
characterised−by
resulting−in
Insights
Routinization
appropriated−to−improving
Agency Structure
Human City Interaction
Heathcare
Structuration Theory
Human−Social Challenge
explained−by
to−address
characterised−by
Research Gap
applied−by
Figure 1: From Human City Interaction to Healthcare.
puting power that is increasingly interwoven into the
fabric akin to that of a smart city.
We have only ‘scratched the surface’ so to speak
of the complex social analysis that is required, and
we are not suggesting that Structuration Theory is
the only theory that can help understand this issue.
Rather, this theory articulates the probable challenges
and the ways to address them in the effective human-
computer interactions for improving healthcare.
REFERENCES
Aghaei, S., Nematbakhsh, M. A., and Farsani, H. K. (2012).
Evolution of the world wide web: From web 1.0 to web
4.0. International Journal of Web & Semantic Technol-
ogy, 3(1):1. ID: 503.
Belt, T. H. V. D., Engelen, L. J., Berben, S. A., and
Schoonhoven, L. (2010). Definition of health 2.0 and
medicine 2.0: a systematic review. Journal of medical
Internet research, 12(2):1–14. ID: 507.
Beverungen, D. (2013). On the design of IT artifacts and the
emergence of business processes as organizational rou-
tines. ID: 529.
Bos, L., Marsh, A., Carroll, D., Gupta, S., and Rees, M.
(2008). Patient 2.0 empowerment. In SWWS, pages 164–
168. ID: 508.
Boulos, M. N. K. and Wheeler, S. (2007). The emerging
web 2.0 social software: an enabling suite of sociable
technologies in health and health care education1. Health
Information & Libraries Journal, 24(1):2–23. ID: 511.
Broy, M., Cengarle, M. V., and Geisberger, E. (2012).
Cyber-physical systems: imminent challenges. In Mon-
terey workshop, pages 1–28. Springer. ID: 517.
Checkland, P. and Holwell, S. (1997). Information, systems
and information systems: making sense of the field.
Choudhury, N. (2014). World wide web and its journey
from web 1.0 to web 4.0. International Journal of Com-
puter Science and Information Technologies, 5(6):8096–
8100. ID: 520.
Churchman, C. W. (1967). Guest editorial: Wicked prob-
lems.
Cockerham, W. C. (2005). Health lifestyle theory and the
convergence of agency and structure. Journal of health
and social behavior, 46(1):51–67. ID: 530.
Dijck, J. V. and Nieborg, D. (2009). Wikinomics and its
discontents: a critical analysis of web 2.0 business man-
ifestos. New media & society, 11(5):855–874. ID: 515.
Eysenbach, G. (2008). Medicine 2.0: social networking,
collaboration, participation, apomediation, and open-
ness. Journal of medical Internet research, 10(3):e22.
ID: 509.
Ferlie, E. (2013). Making Wicked Problems Governable?:
The Case of Managed Networks in Health Care. Oxford
University Press. ID: 185.
Giddens, A. (1984). The constitution of society: Outline of
the theory of structuration. Univ of California Press. ID:
532.
Giddings, L. S. (2006). Mixed-methods research posi-
tivism dressed in drag? Journal of research in nursing,
11(3):195–203. ID: 388.
Greenhalgh, T. and Stones, R. (2010). Theorising big it
programmes in healthcare: strong structuration theory
meets actor-network theory. Social science & medicine,
70(9):1285–1294. ID: 534.
Gurgen, L., Gunalp, O., Benazzouz, Y., and Gallissot, M.
(2013). Self-aware cyber-physical systems and applica-
tions in smart buildings and cities. In Proceedings of the
Conference on Design, Automation and Test in Europe,
pages 1149–1154. EDA Consortium. ID: 525.
House of Commons, T. (2013). The disman-
tled national programme for IT in the NHS.
https://www.publications.parliament.uk/pa/
cm201314/cmselect/cmpubacc/294/294.pdf.
Hughes, B., Joshi, I., and Wareham, J. (2008). Health 2.0
and medicine 2.0: tensions and controversies in the field.
Journal of medical Internet research, 10(3):e23.
Jennings, N. R., Moreau, L., Nicholson, D., Ramchurn,
S., Roberts, S., Rodden, T., and Rogers, A. (2014).
ICEIS 2017 - 19th International Conference on Enterprise Information Systems
176

Human-agent collectives. Communications of the ACM,
57(12):80–88. ID: 535.
Jin, J., Gubbi, J., Marusic, S., and Palaniswami, M. (2014).
An information framework for creating a smart city
through internet of things. IEEE Internet of Things Jour-
nal, 1(2):112–121. ID: 524.
Jones, M. R. and Karsten, H. (2008). Giddens’s structura-
tion theory and information systems research. Mis Quar-
terly, 32(1):127–157. ID: 263.
Le Bon, G. (1897). The crowd: A study of the popular mind.
Fischer.
Leimeister, J. M. (2010). Collective intelligence. Business
& Information Systems Engineering, 2(4):245–248. ID:
510.
Lessard, C. (2007). Complexity and reflexivity: two impor-
tant issues for economic evaluation in health care. Social
science & medicine, 64(8):1754–1765. ID: 387.
Li, X., Lu, R., Liang, X., Shen, X., Chen, J., and Lin, X.
(2011). Smart community: an internet of things applica-
tion. Communications Magazine, IEEE, 49(11):68–75.
Lupton, D. (2015). Health promotion in the digital era:
a critical commentary. Health promotion international,
30(1):174–183. ID: 505; LR: 20150214; CI: (c) The Au-
thor 2014; JID: 9008939; OTO: NOTNLM; ppublish.
Naphade, M., Banavar, G., Harrison, C., Paraszczak, J., and
Morris, R. (2011). Smarter cities and their innovation
challenges. Computer, 44(6):32–39. ID: 521.
Parameswaran, M. and Whinston, A. B. (2007). Social
computing: An overview. Communications of the As-
sociation for Information Systems, 19(1):37. ID: 504.
Patel, K. (2013). Incremental journey for world wide web:
introduced with web 1.0 to recent web 5.0-a survey pa-
per. International Journal, 3(10). ID: 519.
Rickles, D., Hawe, P., and Shiell, A. (2007). A simple
guide to chaos and complexity. Journal of epidemiol-
ogy and community health, 61(11):933–937. ID: 189;
LR: 20140904; JID: 7909766; RF: 68; OID: NLM:
PMC2465602; ppublish.
Rittel, H. W. and Webber, M. M. (1973). Dilemmas in a
general theory of planning. Policy Sciences, 4(2):155–
169.
Roche, S. and Rajabifard, A. (2012). Sensing places’ life to
make city smarter. In Proceedings of the ACM SIGKDD
International Workshop on Urban Computing, UrbComp
’12, pages 41–46, New York, NY, USA. ACM.
Setia, P., Setia, M., Krishnan, R., and Sambamurthy, V.
(2011). The effects of the assimilation and use of it ap-
plications on financial performance in healthcare organi-
zations. Journal of the Association for Information Sys-
tems, 12(3):274. ID: 533.
Surowiecki, J. (2005). The wisdom of crowds :
why the many are smarter than the few. Abacus,
London. Includes bibliographical references.; ID:
44SHU
ALMA2127598670002501.
Tapscott, D. and Williams, A. D. (2008). Wikinomics: How
mass collaboration changes everything. Penguin. ID:
513.
van der Weel, H. (2017). A city trip to enterprise ar-
chitecture. www.linkedin.com/pulse/city-trip-
enterprise-architecture-harald-van- der-weel.
(Accessed on 01/26/2017).
van Veenstra, A. F., Melin, U., and Axelsson, K. (2014).
Theoretical and practical implications from the use of
structuration theory in public sector information systems
research. In The European Conference on Information
Systems (ECIS) 2014, Tel Aviv, Israel, June 9-11, 2014.
ID: 531.
Wang, F.-Y., Carley, K. M., Zeng, D., and Mao, W. (2007).
Social computing: From social informatics to social in-
telligence. IEEE Intelligent Systems, 22(2). ID: 502.
Waterson, P. (2014). Health information technology and
sociotechnical systems: A progress report on recent de-
velopments within the uk national health service (nhs).
Applied Ergonomics, 45(2):150–161.
Xia, F. and Ma, J. (2011). Building smart communities with
cyber-physical systems. In Proceedings of 1st interna-
tional symposium on From digital footprints to social and
community intelligence, pages 1–6. ACM. ID: 522.
Improving Healthcare through Human City Interaction
177
