Decision Making Support in the Scheduling of Chemotherapy Coping
with Quality of Care, Resources and Ethical Constraints
Christophe Ponsard
1
, Renaud De Landtsheer
1
, Yoann Guyot
1
,
Franc¸ois Roucoux
2
and Bernard Lambeau
3
1
CETIC Research Centre, Charleroi, Belgium
2
Grand H
ˆ
opital de Charleroi, Charleroi, Belgium
3
Enspirit, Sombreffe, Belgium
Keywords:
Clinical Pathway, On-line Scheduling, Oncology, Workflow Enactment, Constraint-Based Local Search,
Agent System.
Abstract:
The scheduling of clinical pathways such as oncological treatments involves a tricky decision process because
the therapeutic regimens require to respect strict timing constraints with possibly limited resources such as
beds and caregivers availability with an increasing number of patients. Such constraints must be met simul-
taneously for every patient treated at the same time, by making the best use of limited hospital resources.
The scheduling must also be robust in case of adverse events such as unexpected delays or partial treatment
deliveries due to their toxicity. In this paper, we show how such a decision process can be driven by care
quality indicators to ensure all the dimensions. We demonstrate how constraint-based local search techniques
can cope with real-world size chemotherapy pathways and efficiently adapt to changes. We also share some
ethical concerns about the way the objective function is expressed and more generally about how the tool
integrates in the medical decision process.
1 INTRODUCTION
In Western countries, due to progress in medical care
and ageing of the population, hospitals have to man-
age increasingly complex and multidisciplinary med-
ical procedures over a growing pool of patients. In
the worst case, this results in a decrease in the quality
of care received by patients, which does not always
match the recommended care process yet prescribed.
A survey of 30 pathologies ranging from osteoarthri-
tis to breast cancer, observed that, on average, half of
the patients received the recommended medical care
(McGlynn et al., 2003).
In order to reduce the variability in clinical pro-
cesses and improve the care quality, a level of stan-
dardisation was proposed through clinical pathways
(or care pathways). A clinical pathway is defined
as a multi-disciplinary specification of the treatment
process required by a group of patients presenting
the same medical condition with a predictable clini-
cal course (Campbell et al., 1998). It describes con-
crete treatment activities for patients having identical
diagnoses or receiving the same therapy.
This standardization results usually in less delays,
higher quality assurance and in reduced costs. As they
are strongly oriented on the process description, clin-
ical pathways also maintain a global view on the pa-
tients overall journey, instead of individual doctors
having a view exclusively limited to their medical
speciality (van Dam et al., 2013).
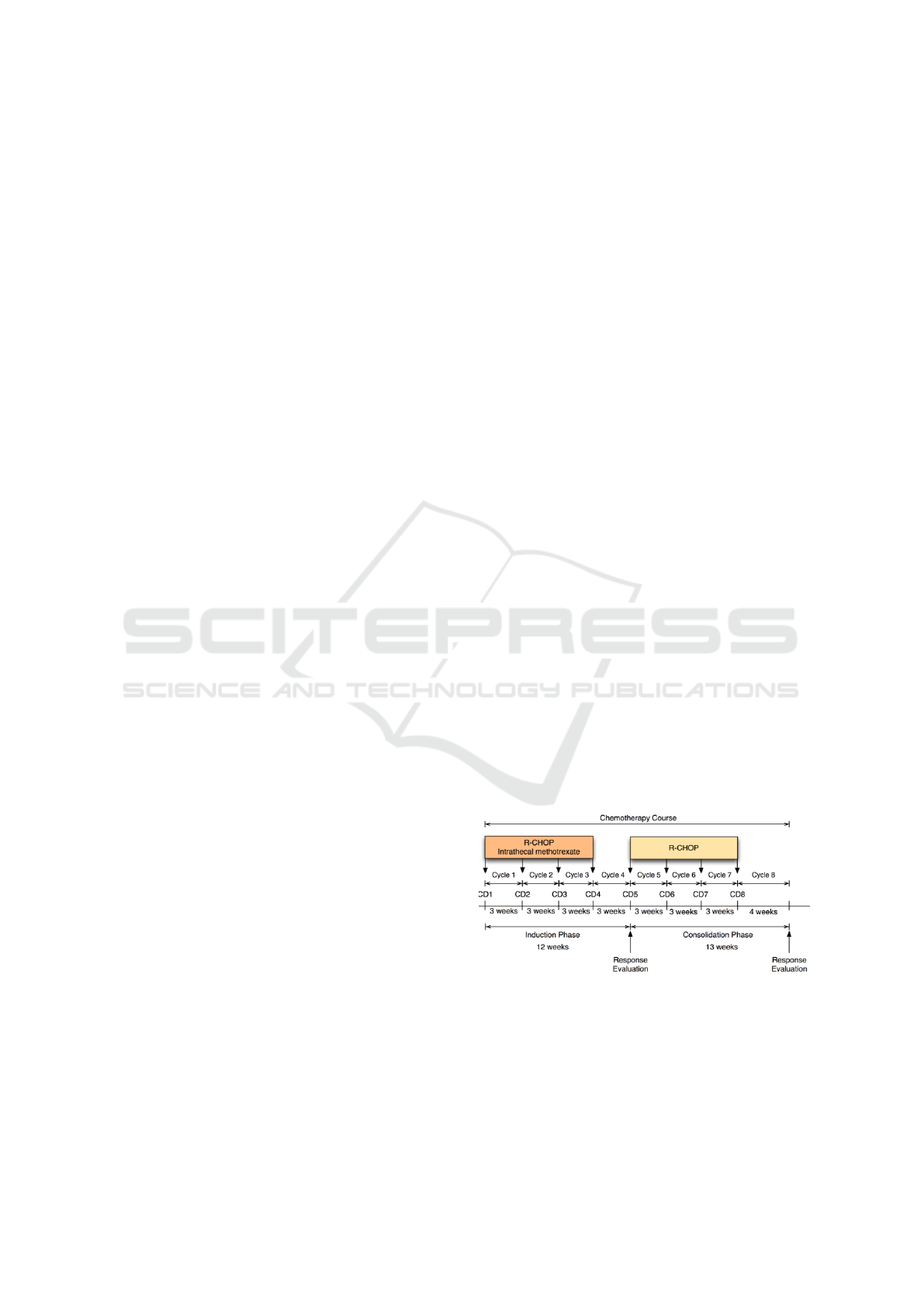
Figure 1: A typical chemotherapy workflow.
The use of clinical pathways have been reported
as successful in many therapies, such as arthroplasty
(Walter et al., 2007) and breast cancer (van Dam et al.,
2013). Clinical pathways in oncology involve a pre-
cise description of the therapeutic workflow and all
its ancillary activities. Such a partial workflow about
460
Ponsard, C., Landtsheer, R., Guyot, Y., Roucoux, F. and Lambeau, B.
Decision Making Support in the Scheduling of Chemotherapy Coping with Quality of Care, Resources and Ethical Constraints.
DOI: 10.5220/0006360504600470
In Proceedings of the 19th International Conference on Enterprise Information Systems (ICEIS 2017) - Volume 1, pages 460-470
ISBN: 978-989-758-247-9
Copyright © 2017 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
the chemotherapeutic aspect of a treatment is illus-
trated in Figure 1. Of course, implementing clinical
pathways requires involvement. A number of success
factors have been reported, like continued clinician
acceptance, top management support and a dedicated
team of case managers, nurses and paramedical pro-
fessionals (Choo, 2001).
On the IT side, the computerization of workflows,
guidelines, and care pathways is also reported as a
key step for process-oriented health information sys-
tems (Gooch and Roudsari, 2011). This allows these
processes to be managed by hospital information sys-
tems or in dedicated workflow management systems.
Such autonomous workflow management systems can
indeed use clinical workflows as a process model de-
scription (Mauro et al., 2010). A key component in
this evolution is to provide efficient tools to support
the scheduling of these workflows. While scheduling
the pathway of a single patient or scheduling the activ-
ities of a specific medical department are not that dif-
ficult, scheduling a large pool of patients in an hospi-
tal with limited resources raises a lot of trade-off con-
cerns (Marynissen and Demeulemeester, 2016). Ide-
ally, such concerns should not impact the quality of
care of individual patient. More, basic ethical princi-
ples state that every patient deserves optimal care re-
gardless of his medical condition or prognosis. Given
that the patients flow is continuous and that a number
of unforeseen events require postponing or adaptation
of treatment sessions, schedules need to be adjusted
on the go. These adjustments should of course com-
ply with already confirmed appointments. The ob-
served practice is that treatment scheduling still usu-
ally rely on human-operated manual tools such as
spreadsheets or scheduling templates (Ahmed et al.,
2011).
In this paper, we address the problem of schedul-
ing treatment appointments in clinical pathways. In
order to ensure care quality over a large pool of pa-
tients within available resources, we put care quality
indicators at the heart of the scheduling algorithms.
The latter are implemented using Constraint-Based
Local Search (CBLS), a technique known for its abil-
ity to scale on large scheduling problems (Van Hen-
tenryck and Michel, 2009). Our algorithms can
also efficiently provide new schedules in reaction to
changes in some patient constraints (on-line prob-
lems). In order to provide a concrete validation,
we have focused our efforts on the scheduling of
the chemotherapy part of oncological pathways and
more precisely on cancer chemotherapy (breast can-
cers, brain cancers, lymphoma ...) for which a key
treatment quality indicator called RDI (Relative Dose
Intensity) has been defined (Lyman, 2009). This case
study is relevant because proper enforcement of time
constraint is critical to maximize the chances of sur-
vival of the patients. The availability of the RDI for
these treatments, and its proven correlation with sur-
vival rates, enables us to quantify the enforcement of
time constraints, so that corrective actions might be
considered in case of a deviation.
This paper is organised as follows. In section 2,
we present domain background about chemotherapy
pathways and technical background on constraint-
based local search. Section 3 gives a clear statement
of the problem tackled in the paper. Section 4 dis-
cusses key design aspects of the solution while Sec-
tion 5 details its implementation. The validation is
carried out in Section 6 and relies on an environment
simulator. Related work is discussed in Section 7. Fi-
nally Section 8 concludes and highlights future work.
2 BACKGROUND
This section first presents the problem domain of
chemotherapy pathways before introducing local
search frameworks, and then focusing on the neces-
sary vocabulary of CBLS framework used in the re-
maining of the paper, based on the OscaR.cbls engine.
2.1 Chemotherapy Pathways
The typical workflow for a chemotherapy is a se-
quence of drugs deliveries or cures, typically adminis-
tered in day hospital. Each cure is followed by a rest-
ing period at home that lasts for a few days to a few
weeks. A minimal interval between cures is required
because chemotherapy drugs are toxic agents and the
body needs some time to recover between two drugs
deliveries. When following the ideal treatment proto-
col, the number of cancerous cells are progressively
reduced, hopefully to reach a full healing or cancer
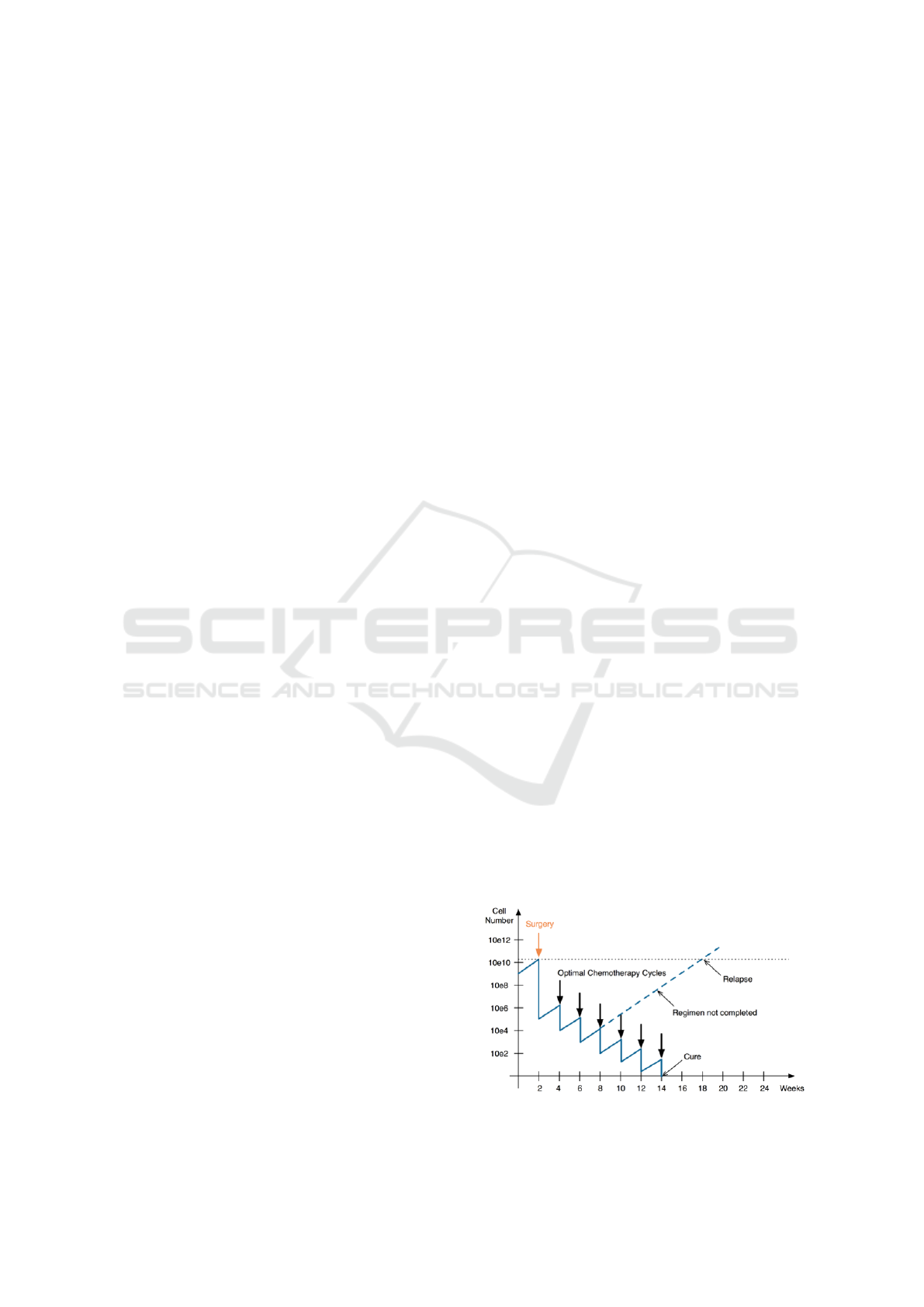
remission as shown in Figure 2.
Figure 2: Optimal chemotherapy cycles.
Decision Making Support in the Scheduling of Chemotherapy Coping with Quality of Care, Resources and Ethical Constraints
461
If for some reason, chemotherapy cures do not
closely follow the intended periodicity or if doses are
significantly reduced, the treatment efficiency may be
suboptimal. In such conditions, cancerous cells may
multiply again, which can result in a cancer relapse as
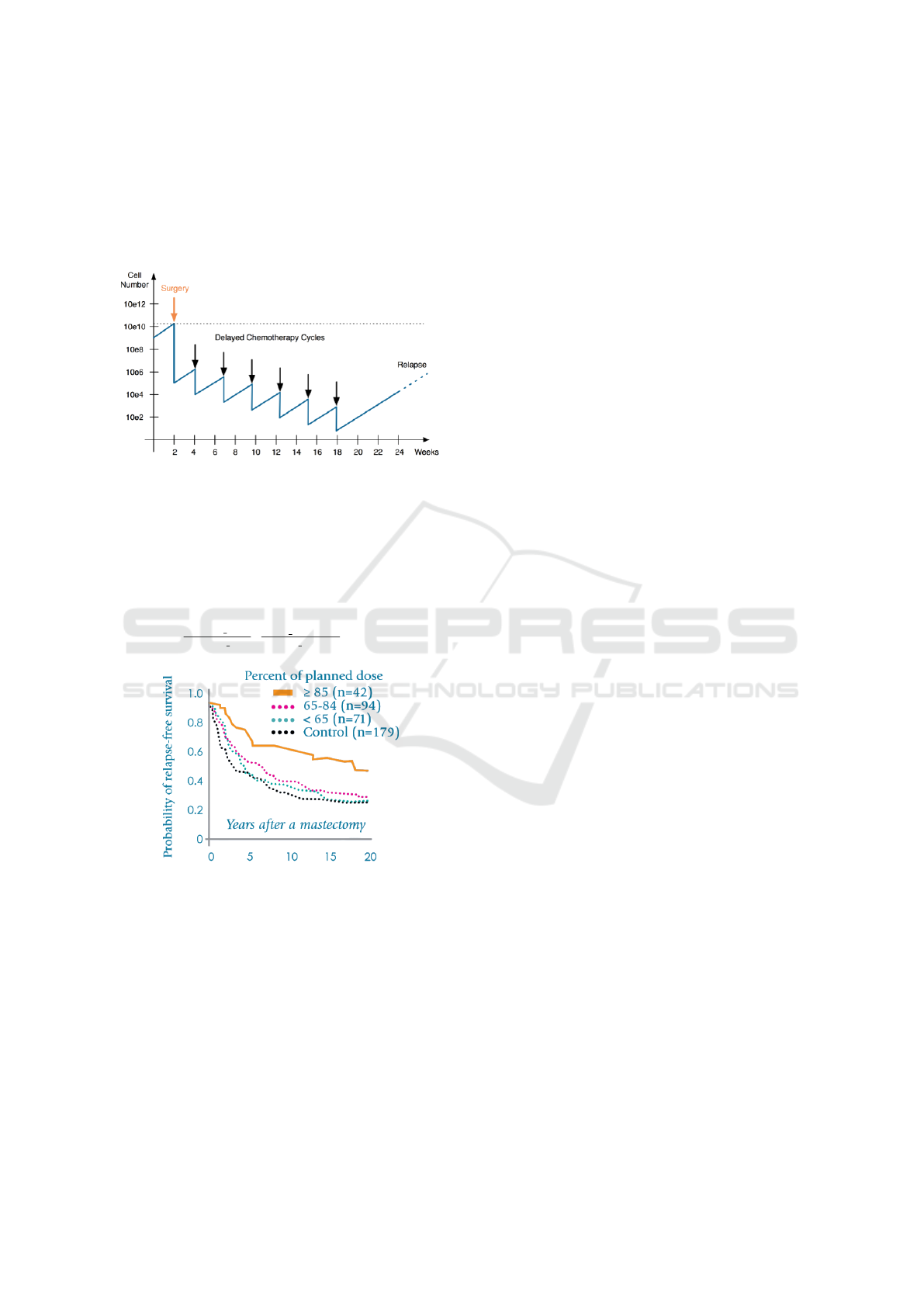
shown in Figure 3
Figure 3: Delayed chemotherapy cycles.
In order to measure the quality of chemotherapeu-
tic cares, a quantifiable indicator called the “Relative
Dose Intensity” (RDI) (Lyman, 2009) was defined.
It captures both the the fact that the required dose is
administered and the timing of the delivery, on a scale
from 0% (no treatment) to 100 % (total conformance).
RDI =
planned dose
delivered dose
x
real duration
planned duration
Figure 4: Probability of relapse-free survival vs. RDI.
Medical literature has shown, for a number of can-
cers, that the relapse-free survival is strongly corre-
lated with the RDI. For instance, for breast cancer, a
key threshold value is 85 % as illustrated in Figure 4
(Piccart et al., 2000). Hence this indicator can be seen
has a gauge that should be carefully managed across
the whole clinical pathway.
2.2 Local Search Frameworks
Local search frameworks aim at making the devel-
opment of algorithmic local search solutions much
simpler than traditional coding. To this end, they
provide different degrees of implementation support,
from problem modelling to the elaboration of a search
procedure. We use such a framework to develop a
schedule optimizer for clinical pathways.
Among the general local search frameworks, Ea-
syLocal++ is a well known and representative one
that requires a dedicated model to be developed
from scratch using ad-hoc algorithms. It mainly
provides support for declaring the search procedure
(Di Gaspero and Schaerf, 2003). It does not provide
as much assistance in the development of a model as
a CBLS framework would. Notably it does not allow
the developer to package efficient global constraints
that can be instantiated on demand.
Besides OscaR, the framework we have used and
described in the next section, there are a few tools
supporting constraint-based local search specifically:
• Comet is the seminal system for constraint-based
local search (Van Hentenryck and Michel, 2009).
It features a differentiation facility that is not im-
plemented in OscaR.cbls. OscaR.cbls relies rather
on partial propagation to provide a comparable ef-
ficiency. Besides, differentiation as provided by
Comet cannot handle intricate models where con-
straints are posted on variables controlled by in-
variants. Comet is a proprietary system available
under a commercial licence.
• LocalSolver is a commercial solver implement-
ing CBLS. It supports boolean and floating point
variables. It does not require the user to specify
neighbourhoods or meta-heuristics (Benoist et al.,
2011).
• Kangaroo provides a partial propagation feature
that is more selective than OscaR.cbls (Newton
et al., 2011).
2.3 CBLS, the OscaR Way
Among the different solvers, OscaR.cbls was se-
lected. Since this contribution has been done in the
context of the OscaR.cbls tool, we further introduce
the basic concepts of CBLS using the vocabulary of
OscaR.cbls.
As usual in local search, solving a problem in-
volves specifying a model and a search procedure.
The model is composed of incremental variables
(integers and sets of integers at this point), and in-
variants which are incremental directed constraints
maintaining one or more output variables according
to the atomic expressions they implement (e.g. Sum:
the sum of inputs). Constraints are special invari-
ants that maintain their violation as an output variable.
ICEIS 2017 - 19th International Conference on Enterprise Information Systems
462
They are Lagrangian relaxations of their specification.
Besides, they also maintain some information about
which variable causes the violation.
The search procedure is expressed using neigh-
bourhoods, which can be queried for a move, given
the current state of the model, an acceptance crite-
rion, and an objective function. Combinators are a set
of operators on neighbourhoods that combine them
and incorporate several metaheuristics, so that a com-
plex search strategy can be represented by a compos-
ite neighbourhood totally expressed in a declarative
way (De Landtsheer et al., 2015). A library of combi-
nators is available for specifying standard metaheuris-
tics (e.g. simulated annealing, restart, hill climbing),
for managing solutions (e.g. when to save the current
state, or restore a saved state), and for expressing stop
criteria.
In order to set up the floor for designing a schedul-
ing solution, we give details on how the model is rep-
resented and updated during the search.
The data structure behind a model is a graph,
called the propagation graph, which we can approxi-
mate to a directed acyclic graph, where the nodes are
variables and invariants. Variables have an associ-
ated type and implement specific algorithms related
to their type. Invariants have specific definitions, and
implement this definition mostly through incremental
algorithms. Edges in the graph represent data flows
from variables to listening invariants and from in-
variants to controlled variables. The directed acyclic
graph starts with input (a.k.a. decision) variables, and
typically ends at a variable whose value is maintained
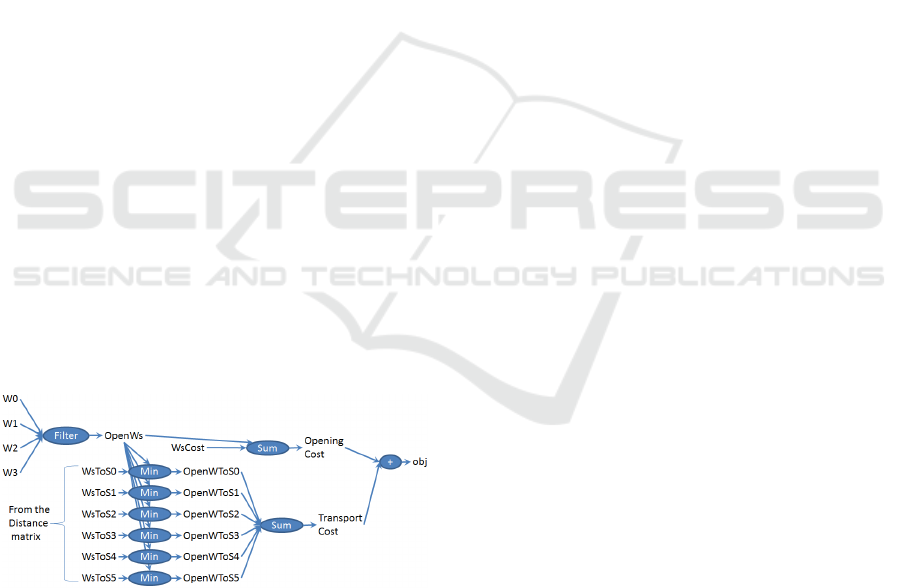
to be the one of the objective function. Figure 5 il-
lustrates a propagation graph for a simple warehouse
location problem.
Figure 5: Propagation graph on a warehouse location prob-
lem.
In such engine, propagation is about propagating
updates along the propagation graph in such a way
that a node is reached at most once by the update
wave, and only if one of its inputs has changed and
if needed by the model update. OscaR.cbls manages
this wave by sorting the nodes based on the distance
from the decision variables. The propagation is co-
ordinated through a dedicated heap that aggregates
nodes at the same distance in a list. This offers a
slightly better time complexity than the classical ap-
proach based on topological sort initially presented in
(Van Hentenryck and Michel, 2009).
The search starts from an initial solution and ex-
plores the specified neighbourhood. Each neigh-
bour solution is examined by modifying the input
variables, and querying the objective function of the
model which is updated through propagation.
During propagation, variables notify each invari-
ant listening to them about their value change. For
integer variables, a notification carries a reference to
the variable, and the old and new value of the variable.
For set variables, it carries a reference to the variable,
the old value of the variable, the new value of the vari-
able, and both the set of values that have been added
and removed from the variable. All values transmitted
by variables, through notification or through queries
to the variables are immutable, to make the imple-
mentation of algorithms in invariants easier.
3 PROBLEM STATEMENT
The problem considered here is to continuously opti-
mize the scheduling on an evolving set of patients fol-
lowing a specific chemotherapy process as described
in Section 2. The goals of the scheduling optimization
are the following:
• maintain the best quality of care (i.e. achieve the
best RDI) by avoiding delay for all the patients in
the pool
• meet the resources constraints: available treat-
ment rooms and nurses.
• respect service opening days (weekends, holi-
days) and hours.
• take into account strong unavailabilities of pa-
tients, when known.
• when possible, distribute the workload evenly
over time to avoid work peaks.
When entering his chemotherapy pathway, a pa-
tient can be given an indicative optimal schedule
based on what is known at that time. However the
global scheduling can be impacted by many events
such as:
• the cancellation of treatment delivery, because of
patient no shows or medical no-go (e.g. too low
white blood cells detected in last blood test),
• the delivery of a partial dose, due to degraded con-
dition induced by chemotherapy toxicity,
• other patients entering and leaving the pathway.
Decision Making Support in the Scheduling of Chemotherapy Coping with Quality of Care, Resources and Ethical Constraints
463

These events are communicated by different ac-
tors to the system (e.g. nurses monitoring the
drugs delivery, doctors checking the patient condi-
tion, administrative staff registering the arrival or non-
attendance of a patient).
To maintain optimality, the occurrence of such
events will trigger a re-scheduling. Consequently, the
considered scheduling is an on-line problem which
should meet the following additional constraints:
• the recorded past is of course irreversible: this
makes any deviation to the ideal care delivery
schedule hard to reverse.
• confirmed appointments for other patients should
preferably not be changed because it requires ad-
ministrative work and can induce a cascading ef-
fect.
A key actor in charge of activity re-planning is
the administrative nurse. She is frequently in con-
tact with the patient and acts as a relay between the
patient and the system. She is also in charge of ne-
gotiating and confirming the future treatment delivery
dates between the patient and the system:
• in the ideal case, all dates initially computed are
respected.
• in case of problems in the patient’s pathway, the
patient schedule is adapted. This can impact the
schedules of other patients. This is not important
if the schedule shift is minor and concerns dates
that are not yet confirmed.
• if the patient wants to delay a treatment delivery,
the system shall estimate the impact of such delay
in terms of degradation of the chances of healing.
This degradation shall be reported to the patient,
e.g. by strongly insisting on the importance to
comply with the proposed date if a good RDI is
compromised.
Figure 6 gives a complete contextual view of the
information flow between the patient and the schedul-
ing system and the information the system need an
access to.
Figure 6: Problem context diagram.
4 SOLUTION DESIGN
In this section, we first propose a global architecture
for the scheduling solution and then consider the more
tricky problem of specifying a fair objective function.
4.1 Global Scheduling vs. First Come
First Serve
Our approach is about scheduling the care of all pa-
tients together in such a way that some global time
constraints are enforced. The actual situation in most
day hospitals is that patients are scheduled on a first-
come first-serve basis. With such a policy, in case of
resource shortage (beds, nurses), the treatment of a
patient might be postponed by some days. For some
patients, such a delay can result in great harm in terms
of chance of healing.
In contrast, our solution avoids resource shortage
by smartly spreading over time the start date of the
chemotherapy pathways. However, if resources were
still limited, the system will smartly select patients
to postpone by limiting the impact on their time con-
straints and thus their RDI.
4.2 Proposed Architecture
An agile prototype-based approach was applied to de-
sign our scheduling solution. The architectural design
of our solution quickly evolved towards the agent-
based architecture depicted in Figure 7 and composed
of the following agents:
• the Orchestrator is the central agent. It ensures
that the system behaviour is consistent with the
input received and that the information generated
by the system is dispatched to the end user.
• the User interface captures relevant patient infor-
mation and gives comprehensive views over the
pathways at different levels of detail.
• the Simulator is used for validation purpose (see
Section 5).
• the Persister is is charge of managing the state in-
formation about the patients involved in the clin-
ical pathways. It provides a domain representa-
tion to the orchestrator and relies on a relational
database for persistent storage.
• the Oncoplanner is responsible for proposing so-
lutions matching the domain constraints sent by
the Orchestrator when a change requires to com-
pute an updated solution. It relies on the Os-
caR.cbls framework.
This architecture has the following benefits:
ICEIS 2017 - 19th International Conference on Enterprise Information Systems
464
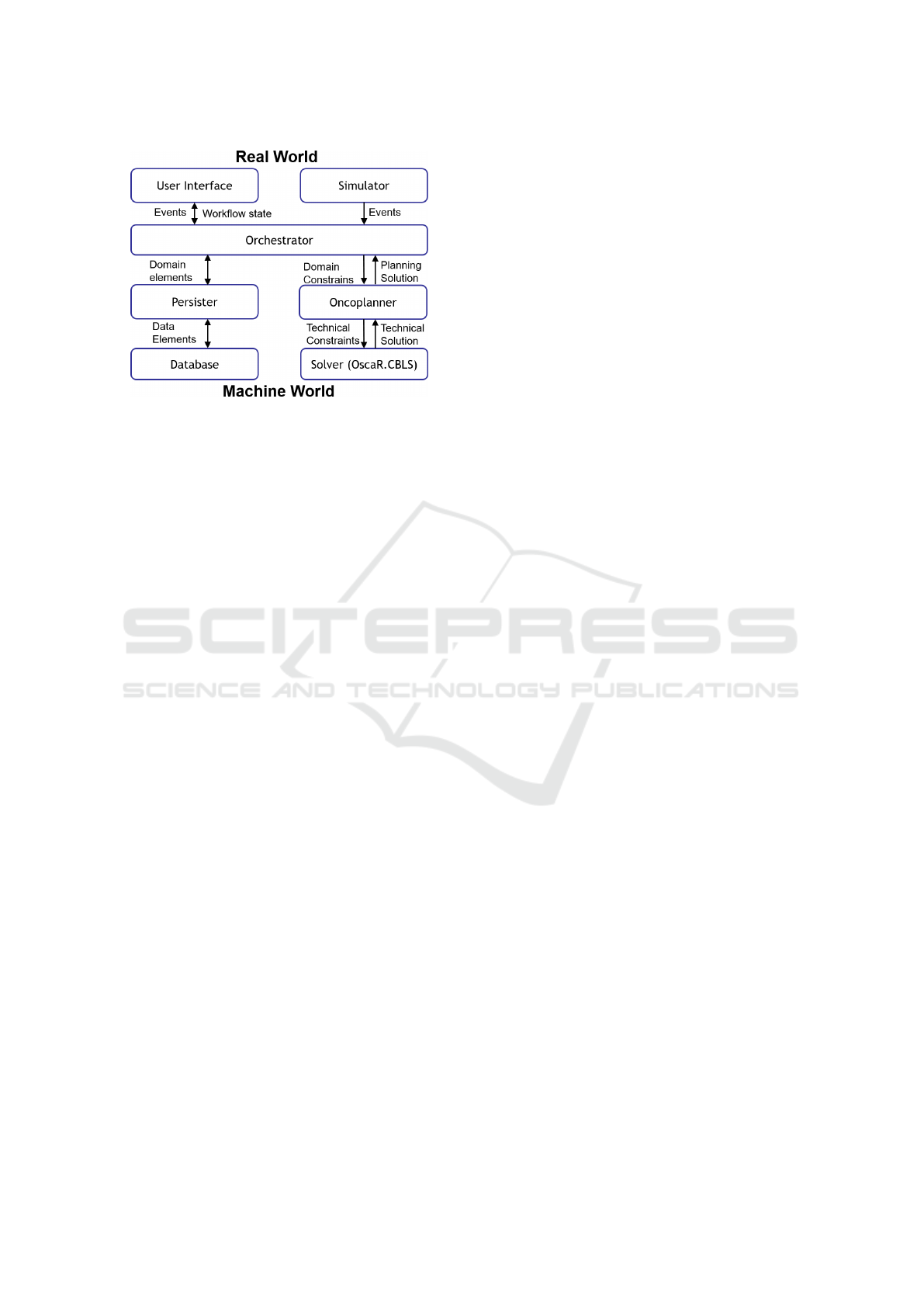
Figure 7: Global architecture.
• it ensures a clear separation between the real
world (user side) and the computer world.
• it allows one to plug different kinds of user inter-
faces easily: first, a basic command line user in-
terface, and later a web-based one using the same
communication protocol.
• it also enables to easily integrate a full environ-
ment simulator which can play complex scenarios
that are able to test the system under high stress.
• it provides good integration capabilities with hos-
pital systems, e.g. to retrieve information from
available databases through specific agents.
In this architecture, the scheduler can also work as
a background service constantly trying to improve the
solution in the open future (i.e. beyond all confirmed
appointments), while the orchestrator can take care of
reporting when some change occurs in the real world.
In case a change makes the current computation irrel-
evant, the orchestrator can ask the scheduler to stop
his work and launch a new computation based on the
updated constraints.
We started with a simplified model combining
the chemotherapy workflows models resulting from
a rigorous analysis process (Damas et al., 2014),
resource constraints and possible interfering events.
An appointment scheduler was developed along with
key companion tools such as a scenario repository,
a graphical interface to manage appointments and a
simulator of patient-related events. This greatly made
easier the validation described in Section 6. The fol-
lowing features were progressively addressed to reach
a model that is now realistic enough to consider a val-
idation at day hospital :
• simple resource model, expressed in bed/nurse
hours evolving to a finer grained model where
each nurse/bed is explicitly allocated.
• service opening days and hours.
• treatment plans, modelled as sequences of steps
(day of cure, resting periods) parameterized with
doses, durations and involved resources.
• constraints on treatment plan instances: earli-
est/latest start date, patient unavailability, set ap-
pointment (past or confirmed).
4.3 Modelling the Objective Function
The objective function to maximize is the global RDI
over the pool of patients. We have developed two
global criteria:
A first criterion was to maximize the minimal RDI
among all patients. It is implemented by minimiz-
ing the schedules makespan among all patients us-
ing iFlatRelax (Michel and Hentenryck, 2004). The
schedule of a patient is an interleaving of appoint-
ments and resting periods, followed by a “stub” activ-
ity at the end. This stub is needed because all patients
do not start their treatment at the same time. That stub
activity enables us to consider their treatment duration
instead of reasoning on their ending date. This crite-
ria may look fair but patients with the highest “healing
chances at start” (e.g. with no dose reduction) could
be considered as “neglected”.
A second criterion was to maximize the summed
RDI. This can be modelled as a tardiness problem,
i.e. overshot of a given point in time (patient depen-
dent) multiplied by a constant. This problem is widely
studied and was solved using a task swapping neigh-
bourhood starting from a solution provided by iFla-
tRelax because it was tightly packed and computed
very quickly.
5 IMPLEMENTATION OF
AGENTS
The implementation of the architecture detailed in the
previous section relies on web services technologies:
our agents communicate through a RESTful protocol
relying on the JSON format for exchanging the re-
quired information. This section highlight key imple-
mentation issues of the agents, except for the simula-
tor which is detailed in Section 6.
5.1 Scheduler Agent
A strong requirement was to cope with large patient
sets, typically involving hundreds of patients simulta-
neously at various stages of their own clinical path-
way. In order to scale to such size, we used lo-
Decision Making Support in the Scheduling of Chemotherapy Coping with Quality of Care, Resources and Ethical Constraints
465
cal search-based approaches, mainly iFlatRelax for
scheduling, and in a later phase, BinPacking for day-
level reasoning. Both algorithms were implemented
using the CBLS engine of OscaR (De Landtsheer and
Ponsard, 2013)(OscaR Team, 2012). They are further
described in the next subsections.
Based on this techniques, our prototype is able
to schedule chemotherapy appointments over roughly
five hundred of patients in a few seconds and supports
interactive adjustments.
5.1.1 Iterative Flattening-Relaxation Search
The algorithm implemented in our prototype is the
one already presented in our previous report, namely:
the iFlatRelax. This algorithm has been improved
with the following new features:
• The possibility to define non-moveable tasks, that
is: tasks that already have a given date. We need
to represent these, because some appointments of
treatments might already be fixed, and we do not
want them to be moved, since they were commu-
nicated to the patient.
• The possibility to define forbidden zones for some
activities, that is: a set of points in time where the
activity cannot take place. The activity is hence-
forth moved forward in time until a proper posi-
tion is found. We will use this feature to represent
patient unavailability.
• A more flexible model of resources, that will
enable us to represent bin-packing resources, as
mentioned in the next section.
5.1.2 Bin Packing
Beds and nurses need to be modelled as they are in
the real world: a patient needs to occupy a bed for a
certain amount of time, and more beds allocated for
a patient will not reduce his time spent in a specific
bed. The consequence is that we cannot represent the
bed resources as a single integer value in terms of bed
hours available in a certain day. Instead, we need to
model beds as done in a bin packing problem: each
bed is a bin whose size is the duration of the day, and
each patient of the day must be put in a bed selected
among the available ones. This allocation shall com-
ply to the fact that the sum of duration of each patient
occupying the same bed is lower or equal to the dura-
tion of the day. Patients will occupy the same bed in
sequence, of course.
We therefore needed to represent a so-called “bin
packing resources” exhibiting this behaviour. A bin
packing resource in a scheduling problem is a re-
source divisible into bins of given size. Each activ-
ity using this resource declares a certain amount of
usage. The activities using the same resource at the
same time must be scheduled in proper bins, so that
the sum of each activity using the same bin do not
exceed the capacity of that bin.
So far, we have developed a model of the bin-
packing problem, and a solver for bin-packing prob-
lems. We still need to integrate this solver into our
scheduling engine.
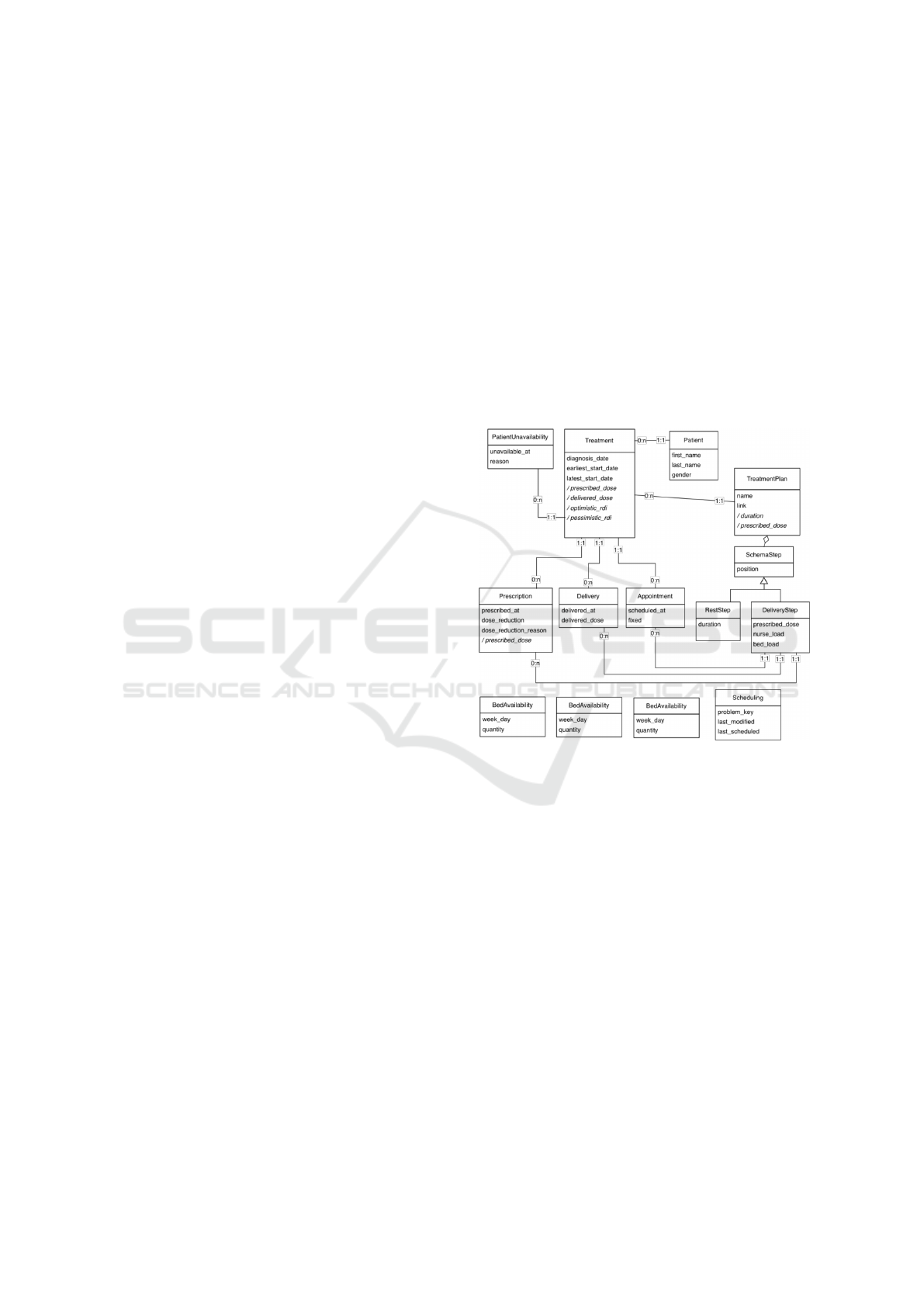
5.2 Persister Agent
The persister agent provides a service-based imple-
mentation of the normalised conceptual model de-
picted in Figure 8.
Figure 8: Data model for a chemotherapy pathway.
It can also be considered as a domain specific lan-
guage for clinical pathways and is composed of the
following concepts:
• Patient: models the information about patients
treated and monitored by the tool.
• TreatmentPlan: captures a reusable treatment
template which is composed of one or more
SchemaSteps, either RestStep or DeliveryStep.
• Treatment: captures a processing instance, for
a given patient. It involves a number of moni-
tored events such as Prescription, Delivery and
Appointment. These are linked to drug injection
steps through DeliveryStep.
• PatientUnavailability, NurseAvailability, and Be-
dAvailability respectively capture the availability
of beds, nurses and patients for the scheduling of
appointments.
ICEIS 2017 - 19th International Conference on Enterprise Information Systems
466
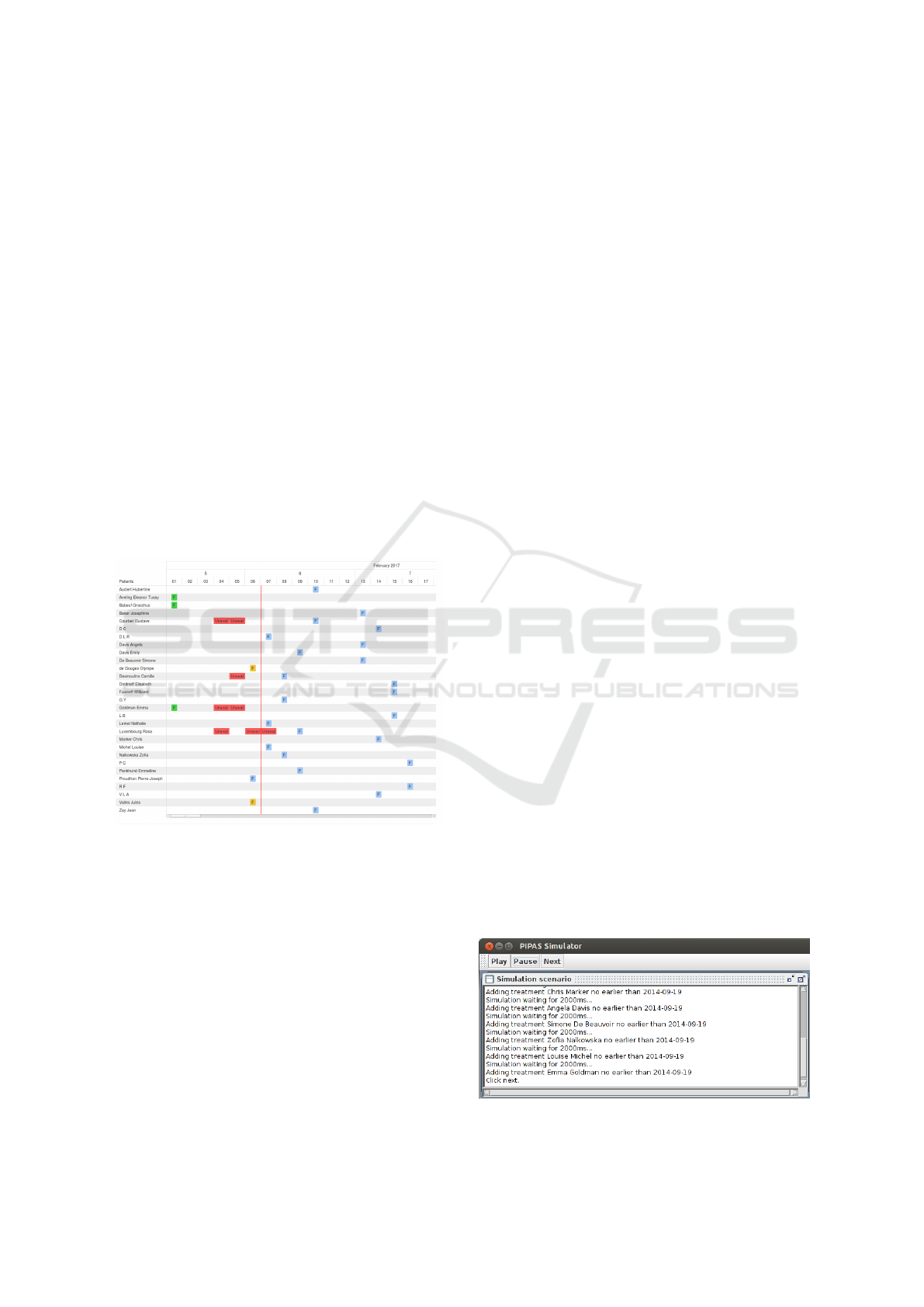
5.3 Agenda-based User Interface Agent
The user interface is a browser-based HTML/-
JavaScript application interacting with the orchestra-
tor. It is implemented using AngularJS. The interface
is depicted in Figure 9. It provides:
• the visualisation of the clinical pathways of the
whole set of patients, allowing to spot the past
chemotherapy deliveries, the future deliveries
with a distinction between the confirmed ones (the
scheduler will not alter them but the nurse could
move them provided the patient is in the loop)
and unconfirmed ones (these can be moved by the
scheduler until they become confirmed). Service
and patient unavailability are also displayed.
• control over the pool of patient, e.g. adding a new
patient and encoding specific characteristics of his
workflow instance (earliest start date, regimen pe-
riodicity and duration, target dose, etc.).
• encoding of delivery related information, e.g. par-
tial dose delivery, cancellation, no-show, . . .
Figure 9: Agenda user interface.
6 VALIDATION
6.1 Validation Approach
Validation of care pathways in a real day hospital en-
vironment will be considered in advanced research
phases. Until now we used a simulation-based ap-
proach because it helps to understand the system be-
haviour over long periods and under stressed condi-
tions that are difficult to experience in the real world.
It also has the ability to step inside processes and pro-
vide a good understanding of problematic scenarios.
In order to enable an earlier validation, we de-
signed the simulator to:
• Provide a reactive and complete user interface,
clearly illustrating the key characteristics of the
algorithms: quality of the solutions, speed of re-
calculation, taking into account complex events
(no-show, partial dose, report ...)
• Integrate an environment simulator able to gener-
ate flows of planned and unforeseen events that
are experienced by the targeted hospital services
and that can be used to consolidate the required
indicators proving the value of our tool, especially
in relation to the quality of care in terms of com-
pliance with RDI and load management.
6.2 Simulation Framework
As shown by Figure 7, the simulator agent is directly
connected to the orchestrator through the same proto-
col as the user interface. The simulator has two main
components:
• a “driver” responsible for simulating the interac-
tions a user would normally have with the orches-
trator using the UI. It relies on exactly the same
communication protocol (JSON via HTTP) as the
UI.
• a “control panel” to have the control over the
running simulation, depicted in Figure 10. Two
modes are available: (1) step-by-step mode. This
mode enables to have a deep understanding of a
specific run. It can also be used to introduce spe-
cific events manually using the usual user inter-
face. (2) fully automated mode, running at ma-
chine speed. This mode relies on the generation
of events based on probability distributions. It can
be used to spot specific problems and also to as-
sess the performance over a large number of runs
using a Monte-Carlo process.
• a component collecting and displaying the evolu-
tion of relevant indicators, such as the RDIs and
the service load.
Figure 10: Simulator control panel.
Decision Making Support in the Scheduling of Chemotherapy Coping with Quality of Care, Resources and Ethical Constraints
467
The state machine for the patient is illustrated in
Figure 11: between treatment deliveries, it should be
in an “appointment fixed” state and during delivery, it
will be in “Delivery” state (if correctly reported). The
“waiting state” should only be transitory: either just
after a delivery or in case of no show. Those states
should be tracked for minimal duration. The simu-
lator generated events covering those transitions with
given probabilities, e.g. for no show events.
Figure 11: Possible patient states and transitions.
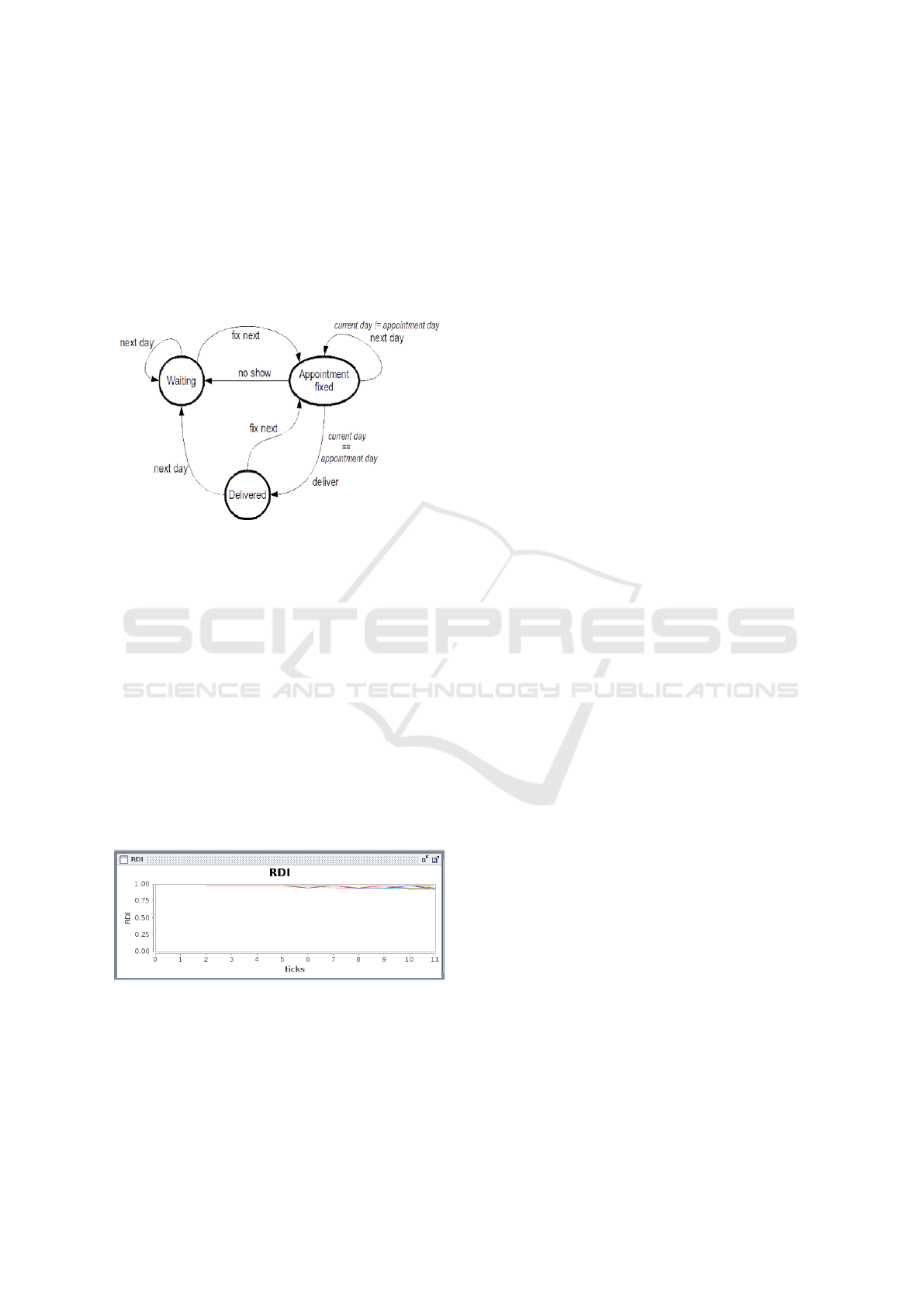
6.3 Results Validation
Several simulations sessions were organised both
with the technical team and in sessions with oncology
practitioners involving three hospitals (UCL/Cancer
Institute, Grand Hospital of Charleroi and UZ Leu-
ven). The feedback from doctors was quite positive
about our contribution to ensure both quality of care
and the smarter use of resources. Figure 12 shows
that the RDI is kept above the 0.85 and above 0.90
in many cases. It is decreasing over time as the re-
sult of minor delays or partial doses delivered due to
chemotherapy toxicity. The day hospital load is also
exhibiting a smooth curve meaning that appointments
can be evenly dispatched over time.
Figure 12: RDI reached in a typical oncology unit.
The prototype also raised ethical concerns, such
as the capacity of the tool to choose to favor some
patients rather than others in case of resource short-
age. Our conclusion is that the system should report
such situations ahead of time to allow the day hospi-
tal team to take corrective measures, like a transient
increase of staffing. In order to keep the medical team
in control, the developed graphical display was also
a huge practical improvement. Some interesting fea-
ture such as the visualization of allocation windows
ensuring a good RDI level definitely helped oncolo-
gists and nurses in charge of appointments updates.
7 RELATED WORK
A complete literature review on integrated hospi-
tal scheduling problems, including pathways, was
recently published by (Marynissen and Demeule-
meester, 2016). Although concepts such as clini-
cal pathways or diagnosis related groups have been
around for more than 20 years, the study reveals that
most of the relevant work is quite recent. Besides
progress in methods and tooling, the main trigger fac-
tor is that hospitals are facing the necessity to break
barriers across services for dealing with the perfor-
mance and capacity challenges they have to face. Cur-
rently, off-line scheduling approaches are more often
reported than on-line methods because hospitals want
to provide the best possible solutions which are re-
lated to the largest possible exploration of the state
space. This rules outs methods which are mostly
based on (meta-) heuristics. However very good (and
in some cases optimal) results of using local search
for outpatient scheduling has been reported in the
literature (Kaandorp and Koole, 2007) and are con-
firmed by the quality of our simulation results. A
key point is that our CBLS engine ensures fast ex-
ploration of the search space, resulting in a good cov-
erage. Moreover our design also allows the system
to continue optimizing the time horizon for appoint-
ments not yet confirmed to patients and thus without
strong time constraints.
A methodology to design appointment systems for
outpatient clinics and diagnostic facilities that offer
both walk-in and scheduled service is presented in
(Kortbeek et al., 2011). The proposed schedule has
two levels: a global level stating the number of ap-
pointments per day and a day level detailing when
each appointment should be scheduled on a given day.
Each level is managed by a specific model and the
two models are connected by an algorithm. Our ap-
proach also proposes two levels with a coarser gran-
ularity at the global level (e.g. we consider global
bed-hours availabilities) while at the day level a fine
grained model is used (i.e. we assign patient to avail-
able beds). Our current validation is however cur-
rently limited to the global level.
Scheduling has also been successfully applied in
other hospital areas. In radiotherapy, several ap-
ICEIS 2017 - 19th International Conference on Enterprise Information Systems
468

proaches of operation research ranging from strategic
capacity management to operational scheduling lev-
els are reported in (Vieira et al., 2016). It highlights
that many improvements regarding the waiting times
and resource utilization can be achieved. A substan-
tive attention is also devoted to the scheduling of the
operation room because it accounts for up 40% of re-
source costs in a hospital. However it differs from on-
cology pathways by a far more important level of un-
predictability. Reported results shows that about 30%
more patients can be scheduled than in actual practice
and the operating room utilization rate is increased by
20% (Barbagallo et al., 2015).
Multiple algorithms and software tools to generate
qualitative surgery schedules on the tactical and op-
erational level are also reported in (Demeulemeester
et al., 2007). This work actually also shows a wider
impact on the whole hospital, since these operation
rooms are interrelated to many other departments or
organizational problems like nurse scheduling or bed
levelling. It also points out the necessity of a good vi-
sualization capabilities because they help health man-
agers to have good insights and they also guide them
in testing different scenarios.
Regarding the computer tools used, the observed
practice is that tool support is often still relying on
manual or basic tools such as spreadsheets or schedul-
ing templates (Ahmed et al., 2011).
8 CONCLUSION
This paper presented an approach for assisting the
scheduling of drug deliveries for treatments where
such deliveries must comply to time constraints un-
der relatively limited resources, namely chemother-
apy regimens. A chemotherapy is delivered in several
deliveries or cures; some timing constraints must be
enforced between these cures. If the cures are spaced
too much, the efficiency of the treatment gradually de-
creases. If the cures are too close in time, there is a
high risk of side effect. These side effects should be
avoided as much as possible.
When it comes to mass medicine, we must con-
sider not only individual patients, but pools of pa-
tients. Every patient that is treated by chemotherapy
depends on the resource of the hospital for the deliv-
ery of his cures. These resources consist mostly in
bed time, nurse time, and doctor time. Since they are
shared resource, there exists a form of competition -
in the mathematical sense - to access these resources.
In practice, such competition is usually solved in
a first come first serve way: every patient sets its ap-
pointments for deliveries, according to its constraints,
and to the available resources. The level of critical-
ity of time enforcement is patient-dependent as it de-
pends on their past history, the status of their disease,
their actual chemotherapy, etc. An indicator has been
proposed, called the RDI to measure the timeliness of
a chemotherapy regimen, and it has been shown to be
correlated with the survival rate of patients for some
cancer types.
Our approach suggests setting the dates of treat-
ment deliveries based on this RDI indicator, by max-
imizing a global measure of the RDI among the con-
sidered pool of patients.
By combining the use of a scalable open source
CBLS scheduling technology with visualization and
simulation components, we were able to show the
feasibility of quality indicator-driven scheduling of a
large pool of patients.
At some point, the following provocative question
for operations research practitioners was raised: is it
really a good or a fair idea to install an optimizing
engine in such a critical setting? As usual the answer
is not in the technology but in the way it is used and
controlled. For instance, the global formula of RDI
is very critical in the sense that it might set global
policies for deciding some life-or-death trade-offs in
the pool of patients. If a patient has a very poor RDI
for its past treatment deliveries, should he get a very
high priority for his coming deliveries or should the
hospital resources be allocated to patients that have
higher probabilities of survival, thus abandoning the
ones that have lower chances?
Clinical pathways involve an intricate decision
making process and our experience shows that the
scheduler can definitely support the medical actors in
their work.
Our next step is to conduct on-site validation
based on an extended prototype. A major request is to
achieve finer tasks management, i.e. within each day.
This requires to rework our algorithms to integrate the
bin packing solver into the scheduling engine. On site
validation should be carefully designed to ensure that
at no time the global process will depend solely on
non-validated tooling. As such, a first step is typically
to run such a tool in parallel with the existing process
and compare their behaviour and outcomes. The next
step is to transmit scheduling suggestions from our
tool to the existing process to check with practition-
ers that the suggestions proposed are applicable and
contribute to improve the quality of care.
Decision Making Support in the Scheduling of Chemotherapy Coping with Quality of Care, Resources and Ethical Constraints
469

ACKNOWLEDGEMENTS
This research was partly funded by the Walloon Re-
gion by the PIPAS (nr. 1017087) and PRIMa-Q (nr.
1610088) projects. We thanks UCL/Cancer Institute,
Grand Hospital of Charleroi and UZ Leuven for their
valuable feedback in key elicitation, design and vali-
dation phases of our work.
REFERENCES
Ahmed, Z., T., E., and S., B. (2011). Developing an efficient
scheduling template of a chemotherapy treatment unit:
A case study. Australas Med J., 4(10):575–88.
Barbagallo, S. et al. (2015). Optimization and planning of
operating theatre activities: an original definition of
pathways and process modeling. BMC Medical Infor-
matics and Decision Making, 15(1):38.
Benoist, T., Estellon, B., Gardi, F., Megel, R., and Nouioua,
K. (2011). Localsolver 1.x: a black-box local-search
solver for 0-1 programming. 4OR, 9(3):299 – 316.
Campbell, H., Hotchkiss, R., Bradshaw, N., and Porteous,
M. (1998). Integrated care pathways. British Medical
Journal, pages 133–137.
Choo, J. (2001). Critical success factors in implementing
clinical pathways/case management. Ann Acad Med
Singapore 30 (4 Suppl), 7:17–21.
Damas, C., Lambeau, B., and van Lamsweerde, A. (2014).
Analyzing critical decision-based processes. IEEE
Trans. Software Eng., 40(4):338–365.
De Landtsheer, R., Guyot, Y., Ospina, G., and Ponsard, C.
(2015). Combining neighborhoods into local search
strategies. In Proceedings of MIC’2015.
De Landtsheer, R. and Ponsard, C. (2013). Oscar.cbls :
an open source framework for constraint-based local
search. In Proceedings of ORBEL’27.
Demeulemeester, E., Sermeus, W., Belin, J., and Cardoen,
B. (2007). Clinical pathways and operations manage-
ment. it takes two to tango. Review of Business and
Economic Literature, LII(3):451–470.
Di Gaspero, L. and Schaerf, A. (2003). EASYLOCAL++:
an object-oriented framework for the flexible design
of local-search algorithms. Software: Practice and
Experience, 33(8):733–765.
Gooch, P. and Roudsari, A. (2011). Computerization of
workflows, guidelines, and care pathways: a review of
implementation challenges for process-oriented health
information systems. Journal of the American Medi-
cal Informatics Association, 18(6):738–748.
Kaandorp, G. C. and Koole, G. (2007). Optimal outpatient
appointment scheduling. Health Care Management
Science, 10(3):217–229.
Kortbeek, N., Zonderland, M. E., Boucherie, R. J., Litvak,
N., and Hans, E. W. (2011). Designing cyclic appoint-
ment schedules for outpatient clinics with scheduled
and unscheduled patient arrivals.
Lyman, G. (2009). Impact of chemotherapy dose intensity
on cancer patient outcomes. J Natl Compr Canc Netw,
pages 99–108.
Marynissen, J. and Demeulemeester, E. (2016). Literature
review on integrated hospital scheduling problems.
Working Papers Department of Decision Sciences and
Information Management 555258, KU Leuven, Fac-
ulty of Economics and Business.
Mauro, C., Happle, T., Sunyaev, A., M.Leimeister, J., and
Krcmar, H. (2010). From medical processes to work-
flows: modeling of clinical pathways with the unified
modeling language. In Int. Conf. on Health Informat-
ics (HealthInf), Valencia, Spain. 161 (9-10).
McGlynn, E. A. et al. (2003). The quality of health care
delivered to adults in the United States. New England
Journal of Medicine, 348(26):26352645.
Michel, L. and Hentenryck, P. V. (2004). Iterative relax-
ations for iterative flattening in cumulative schedul-
ing. In 14th International Conference on Automated
Planning & Scheduling (ICAPS).
Newton, M. A. H., Pham, D. N., Sattar, A., and Maher, M.
(2011). Kangaroo: an efficient constraint-based local
search system using lazy propagation. In Proceedings
of CP’11, pages 645–659.
OscaR Team (2012). OscaR: Operational research in
Scala. Available under the LGPL licence from
https://bitbucket.org/oscarlib/oscar.
Piccart, M., Biganzoli, L., and Di Leo, A. (2000). The im-
pact of chemotherapy dose density and dose intensity
on breast cancer outcome: what have we learned? Eur
J Cancer., 36(Suppl 1).
van Dam, P. A. et al. (2013). A dynamic clinical pathway
for the treatment of patients with early breast cancer
is a tool for better cancer care: implementation and
prospective analysis between 2002–2010. World Jour-
nal of Surgical Oncology, 11(1):70.
Van Hentenryck, P. and Michel, L. (2009). Constraint-
based Local Search. MIT Press.
Vieira, B. et al. (2016). Operations research for resource
planning and -use in radiotherapy: a literature re-
view. BMC Medical Informatics and Decision Mak-
ing, 16(1):149.
Walter, F., Bass, N., Bock, G., and Markel, D. (2007). Suc-
cess of clinical pathways for total joint arthroplasty
in a community hospital. Clin Orthop Relat Res,
7:457:133.
ICEIS 2017 - 19th International Conference on Enterprise Information Systems
470
