
Recovery of the Cognitive Function by the Non-Invasive
Multichannel Neuro-Electrostimulation
for Patients with Amnesic Syndrome
Vladimir Kublanov
1
, Timur Petrenko
1,2
, Mikhail Babich
1
, Anna Petrenko
1
and Konstantin Retyunskiy
2
1
Research and Development Medical and Biological Engineering Centre of High Technologies, Ural Federal University,
Mira 19, 620002, Yekaterinburg, Russian Federation
2
Department of Psychiatry, Ural State Medical University, Repina 3, 620028, Yekaterinburg, Russian Federation
Keywords: SYMPATHOCOR-01 Device, Biofeedback, Neuromodulation, Autonomic Balance Correction,
Neurorehabilitation, Neuro-Electrostimulation, Amnesic Syndrome.
Abstract: The efficiency of non-invasive multichannel neuro-electrostimulation device for recovery of cognitive
functions is presented in article. The article contain description of the structural schematic and algorithm of
the microcontroller execution program of “SYMPATHOCOR-01” device. The possibility of the
“SYMPATHOCOR-01” application for the cognitive disorders treatment is justified. As the example, results
are presented that involved five middle-aged men with signs of pronounced organic amnesic syndrome,
previously held specialized treatment in hospital. As a result, the stimulation rate during the three weeks of
recovery could achieve stable fixing of memory and other cognitive functions in all the patients according to
clinical observation and methods of neuropsychological assessments FAB, MoCA and MMSE. A significant
positive trend noted by the results of the data analysis of EEG and heart rate variability. A hypothesis
mechanism for clinical effect is formulated.
1 INTRODUCTION
Nowadays, population ageing, more complex
technosphere and rapid growth of social stressors
define importance of cognitive disorders, caused by
organic injuries of the Central nervous system (CNS).
The memory is one of the most important cognitive
function. Severe disorders of memory are observed
for patients with organic amnesic syndrome. The
amnesic syndrome arises as a result of the severe
cerebral injury or the intoxication of the brain
(Kopelman, 2002). Neuromodulation, which is a
technology shown to induce neuroplasticity changes,
is the alternative to the traditional pharmacological
methods of the cognitive function recovery (Doidge,
2010). However, contemporary elaborations of the
neuro-electrostimulators applicable to this task in
medicine have a number of the significant drawback
that reduce efficiency of the exposure. For example,
the quick adaptation of the nervous system to
exposure to the external electric fields results in a
decreased reaction when the exposure is continuous.
2 SYMPATHOCOR-01 DEVICE
Group of scientists and engineers from the Ural
Federal University developed the
“SYMPATHOCOR-01” device. The device is
included in the register of medical equipment
products of the Russian Federation (registration
certificate № FCR 2007/00757) and has the
Certificate of correspondence to the requirements of
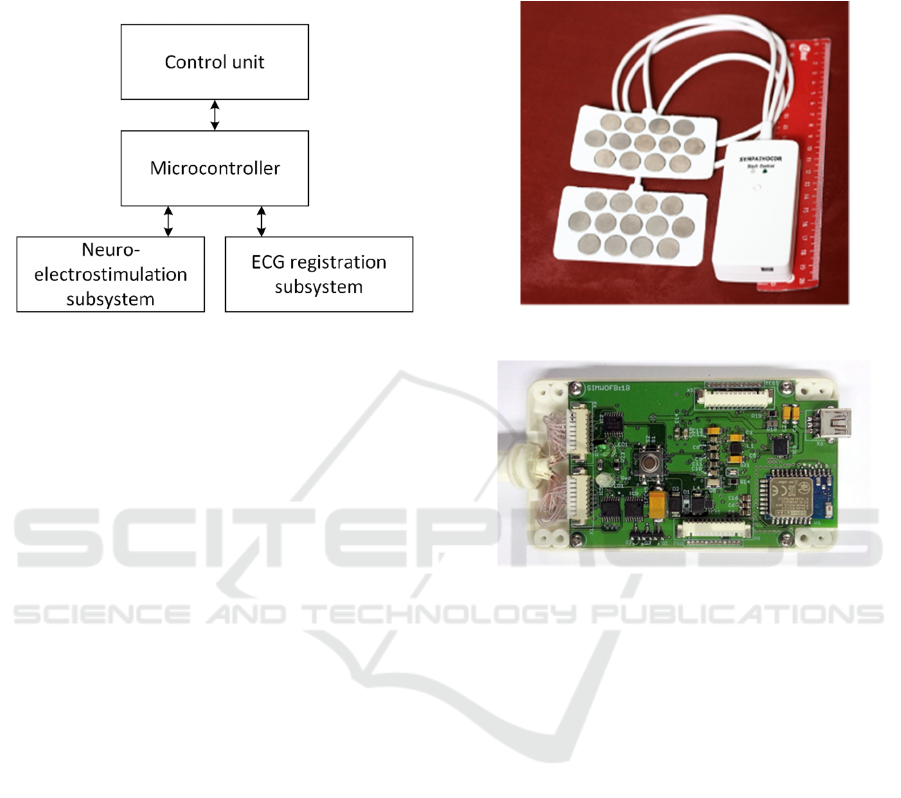
the regulations GOST R 50444-92. Block diagram of
the “SYMPATHOCOR-01” device is shown in Fig.
1. The device includes neuro-electrostimulation
subsystem, electrocardiogram (ECG) registration
subsystem, microcontroller and a control unit.
Neuro-electrostimulation subsystem is used to
create spatially distributed field of current impulses,
which allows correcting the ANS activity. ECG
registration subsystem is used for ECG registration in
the first limb lead scheme for the consequent ECG
analysis, heart rate variability acquisition and
decision making for the structural changes of the
neuro-electrostimulation field. Microcontroller is
Kublanov, V., Petrenko, T., Babich, M., Petrenko, A. and Retyunskiy, K.
Recovery of the Cognitive Function by the Non-Invasive Multichannel Neuro-Electrostimulation for Patients with Amnesic Syndrome.
DOI: 10.5220/0006074400250030
In Proceedings of the 4th International Congress on Neurotechnology, Electronics and Informatics (NEUROTECHNIX 2016), pages 25-30
ISBN: 978-989-758-204-2
Copyright
c
2016 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
25
used to receive and to process commands from the
control unit, neuro-electrostimulation subsystem and
the ECG registration subsystem, and to coordinate
subsystems.
Figure 1: Block diagram of the neuro-electrostimulation
device.
In order to display information about current
neuro-electrostimulation device state, microcon-
troller cyclically poll the neuro-electrostimulation
subsystem and ECG registration subsystem, pack
information about these subsystem states into
information messages and transmit packets to the
control unit. Current ECG data, received from the
ECG registration subsystem are buffered, packed into
information messages and transmitted to the control
unit for the further processing.
The control unit is used by the doctor to control
neuro-electrostimulation procedure, to process and to
analyze ECG signal, to alter neuro-electrostimuila-
tion field of current impulses characteristics, depen-
ding on neuro-electrostimulation program and results
of the ECG signal analysis. A personal computer or a
mobile device can be used as the control unit.
The “SYMPATHOCOR-01” device implemented
as a mobile unit and has dimensions of 90.0 x 50.0 x
18.5 mm. The “SYMPATHOCOR-01” device
general view is shown in Fig. 2. The
“SYMPATHOCOR-01” device main printed circuit
board is shown in Fig. 3.
Neuro-electrostimulation susbsystem consists of:
two multi-element electrodes, first performs
anodes function, and second – cathodes
function
voltage controlled current source (VCCS)
anodes multiplexer, which connects one of the
partial anodes to the positive pole of VCCS
cathodes multiplexer, which connects one of
the partial cathodes to the negative pole of
VCCS
Figure 2: The “SYMPATHOCOR-01” device view.
Figure 3: The “SYMPATHOCOR-01” device main printed
circuit board view.
During neuro-electrostimulation procedure,
microcontroller executes program implemented in
accordance with the algorithm, that shown in Fig. 4.
Alteration of the neuro-electrostimulation field of
current impulses state is possible only at discrete time
points. These discrete time points are determined by
the formula:
∗∗,
(1)
where a
∈
N, N – set of all natural numbers,
T – impulses “packets” repeat interval,
∈,0,
(2)
where K – number of partial cathodes, involved in
neuro-electrstimulation procedure, τ – duration of the
partial impulses.
NEUROTECHNIX 2016 - 4th International Congress on Neurotechnology, Electronics and Informatics
26
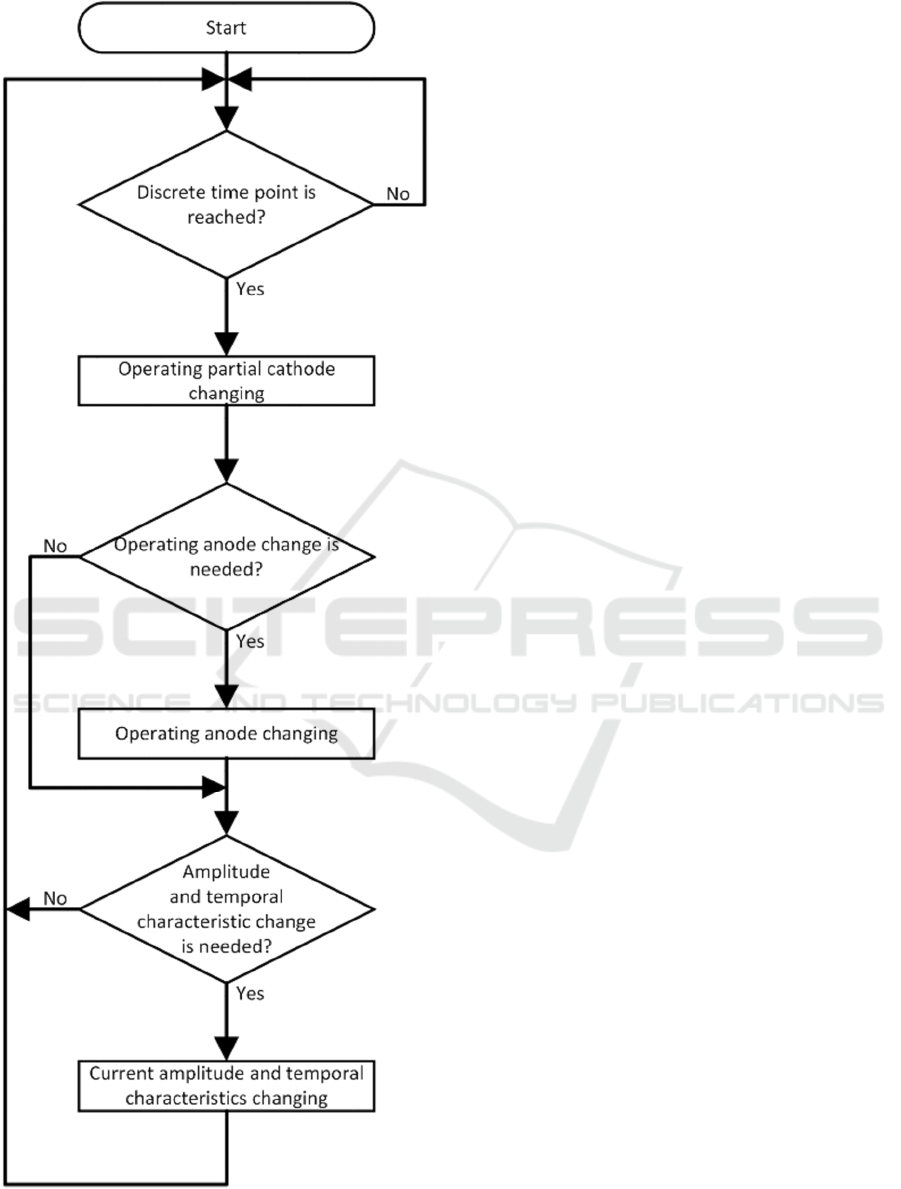
Figure 4: Neuro-electrostimulation microcontroller
algorithm.
The frequency
ν1
⁄
(3)
is called a frequency of the impulses “packets”.
At the discrete time point microcontroller
performs several steps:
Turns off the previous connected cathode and
turns on following cathode according to the
neuro-electrostimulation program. If the
previous connected cathode is the latest
cathode in accordance to the neuro-
electrostimulation procedure than turning on of
the following cathode does not occurs.
After change of the partial cathode, if change
of the anodes is required in accordance with the
neuro-electrostimulation program or by doctor
command, received from the control unit,
microcontroller disconnects the current
connected anode and connects new anode.
If the current amplitude and temporal
characteristics of field of current impulses
(such as impulses “packets” repeat interval,
partial impulse duration, impulse amplitude) is
different from the target characteristics, set by
neuro-electrostimulation program or set by the
control unit, the current field characteristics are
changed in accordance with the following
equations:
,
∆
∆
,
∆
∆
,
∆
(4)
,
∆
∆
,
∆
∆
,
∆
(5)
τ
τ
,τ
τ
∆
τ
∆
,τ
∆
τ
τ
∆
,τ
∆
τ
,
(6)
where A
i
– the partial current impulses amplitude at i
discrete time point, A
target
– the target partial current
impulses amplitude, Δ
A
– the maximum current
impulses amplitude increment, T
i
– the impulses
“packets” repeat interval at i discrete time point, T
target
– the impulses “packets” repeat interval, Δ
T
– the
maximum impulses “packets” repeat interval
increment, τ
i
– partial impulse duration at i discrete
time point, τ
target
– target partial impulse duration, Δ
τ
– the maximum partial impulse duration increment.
Rapid amplitude and temporal characteristic
changes during neuro-stimulation procedure cause
Recovery of the Cognitive Function by the Non-Invasive Multichannel Neuro-Electrostimulation for Patients with Amnesic Syndrome
27

pain. Therefore, microcontroller limit amplitude and
temporal characteristics of field of current impulses
growth rate using amplitude and temporal
characteristics increments.
Subsequent switch of the partial cathodes at the
neck area forms spatially centered current structure.
Maximum of the current density in this structure is
located in the center of the anode. Ability to switch
operating anode allows one to move the maximum
current density point of the spatially centered current
structure. This leads to neuro-electrostimulation
improvements due to increase of the local neuro-
electrostimulation targets number in the neck area.
Improvements of the neuro-electrostimulation
efficiency is achieved through involvement in the
regulatory process brain structures responsible for
motor, visual, auditory, vestibular functions, in
addition to the ANS.
The neuro-electrostimulation subsystem is based
on Analog Devices ADG5408 8-channel multiplexor
chips. These chips perform partial cathodes and
anodes commutation to the VCCS. At the current
version of the neuro-electrostimulation devices four
ADG-5408 chips are used, that allows to connect up
to 16 partial cathodes and 16 anodes for the neuro-
electrostimulation procedure. VCCS is formed by a
current mirror with two BC807 and one BC817
bipolar transistors.
Microcontroller with built-in 12-bit digital-to-
analog converter (DAC) generates control voltage.
Current mirror resistor values are calculated in a way
that the current source can generate a current in the
range 0 to 15 mA with a load from 0 to 2 kOhms.
The ECG registration subsystem obtain signals
from the first limb lead. The signal electrode 1 and
the signal electrode 2 are located on the patient’s
hands. The RLD electrode may be on placed either on
the right leg of the patient or on the any hands of the
patient, if the case of the short circuiting is avoided.
Standard disposable adhesive electrodes for ECG are
used.
The ECG registration subsystem is based on the
usage of the analog interface for ECG applications
ADS1292 chip. The ADS1292 consists of a
differential amplifier with the programmable
amplification factor, 24-bit delta-sigma analog-to-
digital converter (ADC), the device for the down
sampling and digital low-pass filtration, the SPI
interface, the Right Leg Drive (RLD) amplifier.
The first step of the ECG registration is filtration
of the impulse interferences on the patient by a low-
pass RC-filter with the 2 kHz cut-off frequency. The
second step of the conversation is gain of the ECG
signal by a differential amplifier, the amplified signal
is supplied to the ADC and the RLD amplifier. The
RLD amplifier compares the constant component of
the ECG signal with the half supply voltage, amplifies
the difference of signals and uses amplified difference
as RLD signal. Thus, the RLD signal applied to the
patient fluctuates around the half supply voltage
value, which provides chip normal operation.
Delta-sigma ADC operates at 8kSPS sampling
frequency, but further digital signal is filtered with
help of digital low-pass filter and decimated in
accordance with chip configuration. The ECG
registration subsystem signal sampling rate after
decimation is 500 SPS, with 131 Hz cut-off frequency
of the digital low-pass filter. This frequency range is
sufficient to assess the characteristics of the ANS.
The filtered digital signal is sent to the
microcontroller using the modified SPI protocol. In
addition to the standard SPI protocol lines such as
MOSI, MISO, SCLK, additional lines Data Ready
(DRDY) and Conversation Start are used. DRDY
signal is used by the ADS1292 to notify the
microcontroller about the conversion end of the
current data sample. Conversation Start signal is used
for forced start of the ADC.
Usage of the ADS1292 significantly reduces
devices size and improves patients comfort during
neuro-electrsotimulation compared with the case,
when the ECG registration subsystem is implemented
using multiple chips.
3 TREATMENT OF PATIENTS
WITH AMNESIC SYNDROM
Models of cognitive disorders are not sufficiently
formed at the moment. So, researchers and clinicians
encounter with various difficulties in development of
effective approaches for neuro-rehabilitation.
The experimental studies on the laboratory
animals confirmed the efficiency of the developed
technology application for the restoration of the blood
flow after artificial ischemia of the muscle tissue and
for the normalization of the behaviour patterns after
adjustment disorder (Kublanov et al., 2010). Clinical
trials of the patients with epilepsy after application of
the neuromodulation showed non-specific changes of
the neurometabolism based on the data of the single-
photon emission computed tomography (SPECT) in
the cerebral cortex. The global decrease of the activity
of the epileptic areas was shown by the
electroencephalography features (Kublanov, 1999).
The goal of the present study is to define
possibilities of the dynamic correction of the neck
NEUROTECHNIX 2016 - 4th International Congress on Neurotechnology, Electronics and Informatics
28
nerve structures conduction activity for the recovery
of the cognitive function for the patients with the
organic amnesic syndrome. The study was approved
by USMU ethics committee (protocol #8 from
16.10.2015)
Design of serious clinical studies will be produced
based on the results of this project.
3.1 Objectives and Methods
For this pilot study five male patients with clinical
manifestation of the organic amnesic syndrome, as a
result of brain damage caused by different
pathological factors (traumatic brain injury, chronic
alcohol intoxication, poisoning by household toxins)
were investigated at the department of psychiatry of
the Ural state medical university. All patients prior to
the investigation held specialized treatment in
psychological and/or neurological hospital without
significant improvement. The duration of the disease
varied from 12 to 24 months. Patients age varied from
33 to 48 years.
Neuromodulation with the “SYMPATHOCOR-
01” device was used as the treatment course. The
dynamic correction of the neck nerve structures
conduction activity technique allowed affection on
the processes of the autonomic regulation (through
the autonomic ganglia) and stimulation of the brain
stem neuronal centres (through the nerve pathways of
the neck). The treatment course consisted of the 15
procedures on the span of the 3 weeks. There was no
additional pharmacological treatment, except for
designated previously.
Clinical data and psychometric test were used for
the initial and the following evaluation of the
patient’s cognitive skills: Frontal Assessment Batter
(FAB) (Dubois et al., 2000), Montreal Cognitive
Assessment (MoCA) (Nasreddine et al., 2005), Mini-
Mental State Examination (MMSE) (Folstein et al.,
1975). Instrumental diagnostics was performed with
“Encephalan-EEGR-19/26 Medicom Ltd” complex
and included quantitate analysis of the
electroencephalograms (EEG), spectral analysis of
the heart rate variability (HRV) based on
electrocardiogram. The analysed features of the
biomedical signals: power of the main EEG rhythms,
total power of the HRV spectrum (TP), low-
frequency component of the HRV spectrum (6,5-25
s) (LF), high-frequency component of the HRV
spectrum (2,5-6,5 s) (HF). Clinical and instrumental
evaluation was carried out by independent experts.
3.2 Results
The initial state of the patient reflected symptoms of
the severe CNS damage: rough disturbance of
orientation by the amnesic type, rough disturbance of
the fixation amnesia, rapid exhaustion of attention,
lack of cognitive efficiency, phenomena of emotional
incontinence, complacency. Pronounced decrease of
cognitive status and cognitive skills was defined
according to the data of psychometric test.
Pronounced diffusion disorganization of the main
rhythms with signs of the epileptization were defined
by the EEG signals analysis. HRV signals analysis
revealed pronounced signs of autonomic
dysregulation.
The sessions of the dynamic correction of the neck
nerve structures conduction activity resulted in rather
quick positive dynamic. After clinical studies patients
become more active. The fatiguability and attention
disorders reduced, attention and acumen significantly
increase, the cognitive processes and memory
improved.
The recovery of spatial and constructive activity,
dynamic praxis and reciprocal coordination were
noted according to the psychometric tests. The results
proves recovery of the intracerebral connections. The
Table 1 present summary data of the psychometric
tests.
Table 1: Data of the psychometric tests prior and after
treatment.
Psychometric test
Mean values of the scoring
prior treatment after treatment
FAB 5,7 ± 3,1 12,0 ± 4,0*
MoCA 11,3 ± 3,0 16,3 ± 4,0*
MMSE 15,3 ± 6,2 21,3 ± 8,3*
* - significance of the difference of data after treatment
from data prior treatment, P<0,05.
The comparative analysis of the EEG quantitative
features prior and after neuro-electrostimulation
showed recovery with the increase of the alpha-
rhythm power, suppression of the diffusion delta-
activity and paroxysmal patterns “acute-slow wave”.
Results of EEG signals analysis concludes significant
normalization of functional processes in the CNS.
The comparative analysis of the HRV signals
prior and after neuro-electrostimulation noted the
increase of the total power of the HRV and change of
the autonomic balance, defined by the LF/HF ratio.
The autonomic balance became normal. That
concludes normalization of the autonomic regulation
Recovery of the Cognitive Function by the Non-Invasive Multichannel Neuro-Electrostimulation for Patients with Amnesic Syndrome
29

processes which in turn provide conditions for the
recovery of the lost functions. The Table 2 presents
data of the HRV spectrum features changes.
Table 2: Data of the HRV spectrum features prior and after
treatment.
HRV spectrum
features
Mean values of the spectrum
features
prior treatment after treatment
LF/HF 6,39 ± 2,4 2,2 ± 0,7*
* - significance of the difference of data after treatment
from data prior treatment, P<0,05.
4 CONCLUSIONS
The results of the study demonstrated high potential
of the dynamic correction of the neck nerve structures
conduction activity technique to recovery of the
cognitive functions. Apparently, the technique is
capable to activate neuroplasticity processes and
recover of the autonomic regulation in the whole
organism.
Analysis of the recorded data allows one to
formulate hypothesis about the formation
mechanisms of the clinical effects for the developed
neuromodulation method. The main ideas of the
hypothesis:
• cerebral blood flow is modulated due to the
regulation of the arteries tone of the small and
medium calibre;
• suppression of the sympathetic department of the
ANS;
• stimulation of the neurotransmitters production in
the brain stem nucleus;
• suppression of the pathological hypergenerator
areas in the cortex;
The mentioned mechanisms provide condition for
the recovery of the intracerebral connections, which
certainly increase overall adaptive possibilities of the
organism.
It requires full clinical trial according to the GСP
rules to confirm these hypotheses.
P. K. Anochin formulated theory of the afferent
syntheses. According to this theory, the proposed
neuromodulation technique might be the factor which
starts afferentation. The afferentation helps to limits
of the systems activity freedom in order to stabilize
its functions (Anokhin, 1974). However, this
hypothesis needs additional verification.
The obtained results confirm efficiency of the
hardware non-invasive multichannel neuromodula-
tion for the recovery of the cognitive impairment as
the result of the organic damage of the CNS. The
proximate perspectives of the developed technique
are the treatment of the neurodegenerative diseases
and affective disorders. The following development
of the non-invasive multichannel neuromodulation
technique of the nervous formations for the recovery
of the cognitive functions will be defined by the
reliability of the knowledge about plasticity
mechanisms. Biophysicist, radiophysicist, physiolo-
gists, doctors, engineers – all must take part in the
reliable knowledge formation.
ACKNOWLEDGEMENTS
The work was supported by Act 211 Government of
the Russian Federation, contract № 02.A03.21.0006.
REFERENCES
Anokhin, P.K., 1974. Biology and neurophysiology of the
conditioned reflex and its role in adaptive behavior,
International series of monographs on cerebrovisceral
and behavioral physiology and conditioned reflexes.
Pergamon Press.
Doidge, N., 2010. The Brain That Changes Itself: stories of
personal triumph from the frontiers of brain science.
Scribe Publications.
Dubois, B., Slachevsky, A., Litvan, I., Pillon, B., 2000. The
FAB: a Frontal Assessment Battery at bedside.
Neurology 55, 1621–1626.
Folstein, M.F., Folstein, S.E., McHugh, P.R., 1975. “Mini-
mental state”. A practical method for grading the
cognitive state of patients for the clinician. J. Psychiatr.
Res. 12, 189–198.
Kopelman, M.D., 2002. Disorders of memory. Brain J.
Neurol. 125, 2152–2190.
Kublanov, V.S., 1999. Electrophysics method of correction
of the system of regulation of cerebral blood flow.
Biomed. Radio-Electron. 12–15.
Kublanov, V.S., Shmirev, V.I., Shershever, A.S., Kazakov,
J.E., 2010. About Innovative Possibilities of Device
“SIMPATOCOR-01” in Management of Functional
Disorders of Vegetative and Central Nervous System in
Neurology. Kremlin Med. Clin. Vestn. 4, 60–64.
Nasreddine, Z.S., Phillips, N.A., Bédirian, V.,
Charbonneau, S., Whitehead, V., Collin, I., Cummings,
J.L., Chertkow, H., 2005. The Montreal Cognitive
Assessment, MoCA: a brief screening tool for mild
cognitive impairment. J. Am. Geriatr. Soc. 53, 695–
699. doi:10.1111/j.1532-5415.2005.53221.x.
NEUROTECHNIX 2016 - 4th International Congress on Neurotechnology, Electronics and Informatics
30
