
Protecting Medical Data Stored in Public Clouds
Nikos Fotiou and George Xylomenos
Mobile Multimedia Laboratory, Department of Informatics, School of Information Sciences and Technology,
Athens University of Economics and Business, Patision 76, Athens 10434, Greece
Keywords:
Access Control, Identity-based Encryption, Proxy Re-encryption.
Abstract:
Public Clouds offer a convenient way for storing and sharing large amounts of medical data. Nevertheless,
using a shared infrastructure raises significant security and privacy concerns. Even if the data are encrypted,
the data owner should share some information with the Cloud provider, in order to enable the latter to perform
access control; given the high sensitivity of medical data, even such limited information may jeopardize end-
user privacy. In this paper we employ an access control delegation scheme to enable the users themselves to
perform access control on their data, which are stored in a public Cloud. To selectively provide access to these
data without sacrificing their confidentiality we rely on encryption: our system encrypts data before storing
them in the Cloud and applies proxy re-encryption so as to encrypt data separately for each (authorized) user.
1 INTRODUCTION
Nowadays, smart devices that collect users’ vital sig-
nals have become a commodity. It is expected that
soon the data collected by these devices will be used
for preventing and/or diagnosing various health re-
lated problems, as well as for promoting a health-
ier way of living and well-being. Storing and shar-
ing these data using a public Cloud infrastructure ap-
pears to be an appealing option, as public Clouds of-
fer cost effective and reliable storage services. On the
other hand, security and privacy concerns are raised,
as medical data are highly sensitive and they should
be protected, even against the Cloud service provider.
Encryption and access control can be used as a coun-
termeasure, but privacy threats remain. For exam-
ple, an access control policy of the form “these (en-
crypted) data can only be accessed by psychiatrist A”
reveals to the entity that performs access control that
the data owner shares some data with a psychiatrist.
In this paper we propose a system that allows se-
cure and private storage of medical records in the
Cloud. Our system allows data owners to define ac-
cess control policies and to enforce them by them-
selves. The Cloud provider is only responsible for
storing data and for respecting the access control de-
cisions of the data owner. Even if the Cloud provider
misbehaves, the data remain protected since they are
encrypted in a way that only authorized users can ac-
cess them; unauthorized users – including the Cloud
provider – learn nothing about the data. In order
to achieve our goal we extend the system proposed
by (Fotiou et al., 2015) by adding an additional layer
of data confidentiality protection. Our proposal en-
crypts data before storing them in the Cloud and
re-encrypts them as necessary before sharing; data
are encrypted only once by an entity owned by the
data owner, and then the Cloud is responsible for re-
encrypting the data in such a way that only authorized
clients can access them.
The remainder of the paper is organized as fol-
lows. Section 2 briefly presents access control del-
egation and proxy re-encryption. Section 3 presents
our system design. In Section 4 we evaluate our so-
lution and in Section 5 we present related work in the
area. Finally we conclude our paper in Section 6
2 BACKGROUND
2.1 Access Control Delegation
The access control scheme proposed in (Fotiou et al.,
2015) separates data storage and access control func-
tions: the former is implemented in a public Cloud,
whereas the latter is implemented by a trusted entity
named access control provider (ACP). These entities
interact with each other as follows (Figure 1)
1
: Ini-
tially, a data owner creates an access control policy,
1
The description has been modified to fit the purposes of
the present paper.
Fotiou, N. and Xylomenos, G.
Protecting Medical Data Stored in Public Clouds.
In Proceedings of the International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2016), pages 127-132
ISBN: 978-989-758-180-9
Copyright
c
2016 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
127
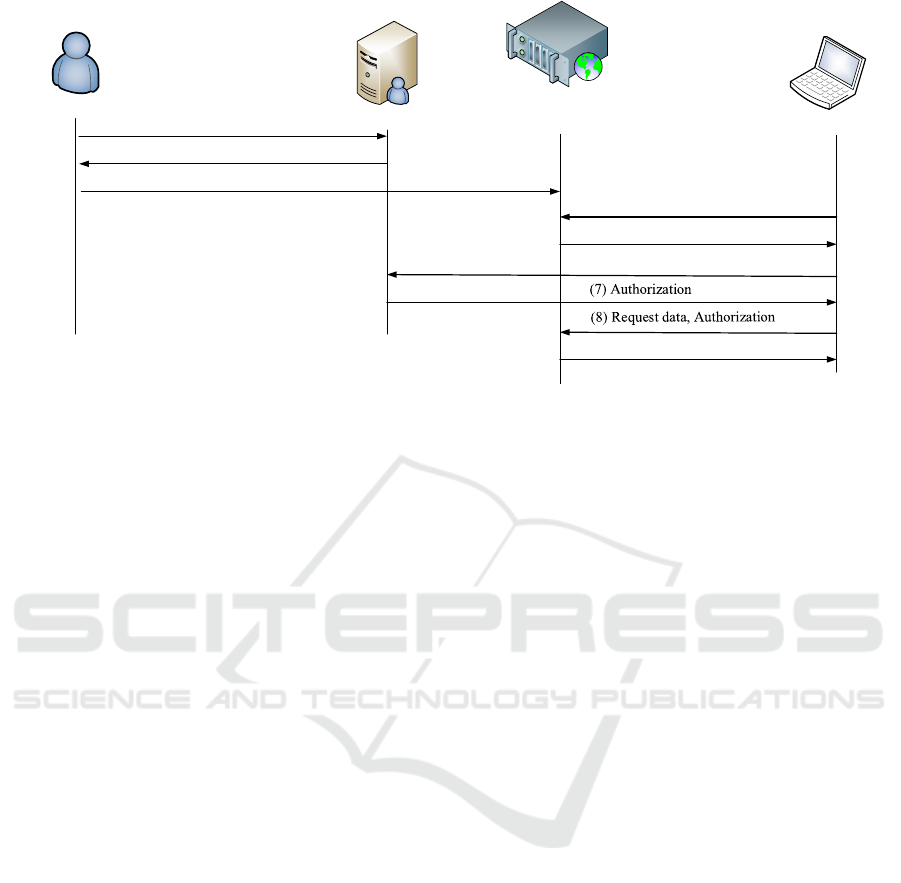
Data Owner
(1) Access control policy
(2) URI to policy
(3) Data, URI to policy
(4) Request data
(5) Token, URI to policy
(6) Authenticate, Token, URI to policy
Cloud
Client
ACP
(9) Data
Figure 1: Access control delegation.
stores it in an ACP (step 1) and obtains a URI for
that policy (step 2). Then, he stores some data in the
Cloud, indicating at the same time the URI of the pol-
icy that protects these data (step 3). When a client
tries to access these data (step 4), the Cloud responds
with the URI of the access control policy and a unique
token (step 5). Then, the client authenticates herself
to the ACP and requests authorization (step 6). If the
client “satisfies” the access control policy, the ACP
generates a signed authorization and sends it back
(step 7). Finally, the client repeats her request to the
Cloud, this time including the authorization (step 8).
The Cloud checks the validity of the authorization and
if it is valid, it returns the desired data (step 9).
This scheme has many advantages. The Cloud
provider learns nothing about the client since all her
personal data (which are required to evaluate the ac-
cess control policy) are stored in the ACP. Moreover,
Cloud providers do not have to interpret any access
control policies, therefore they do not need to under-
stand content owner specific semantics. Access con-
trol policies are reusable i.e, in order to protect a new
item using an existing access control policy the same
URI can be simply re-used. Access control policies
can be easily updated; updating and access control
policy does not involve any communication with the
Cloud provider. Finally, providing that many Cloud
providers support this scheme, it is trivial for a data
owner to migrate from one Cloud provider to another.
2.2 Proxy Re-encryption
A Proxy re-encryption (PRE) scheme is a scheme in
which a third, semi-trusted party, the proxy, is allowed
to alter a ciphertext encrypted with the public key of
a user A (the delegator), in a way that another user B
(the delegatee) can decrypt it with her own appropri-
ate key (in most cases, her secret private key). During
this process the proxy learns nothing about the pri-
vate keys of A and B, and does not gain access to the
encrypted data.
In this paper we employ the identity-based proxy
re-encryption (IB-PRE) scheme by Green and Ate-
niese (Green and Ateniese, 2007). In particular we
use a variant of that scheme in which the delegatee
uses an RSA public key instead of identity-based en-
cryption (section 5 of (Green and Ateniese, 2007)).
This scheme specifies the following algorithms (the
description has been adapted to the RSA variant):
• Setup: it is executed by a Private Key Generator
(PKG). It takes as input a security parameter k and
returns a master-secret key (MSK) and some
system parameters (SP). The MSK is kept se-
cret by the PKG, whereas the SP are made pub-
licly available.
• Extract: it is executed by a PKG. It takes as input
the SP, the MSK, and an arbitrary string ID, and
returns a secret key SK
ID
.
• Encrypt: it can be executed by anyone. It takes
as input an arbitrary string ID, a message M, and
the SP, and returns a ciphertext C
ID
.
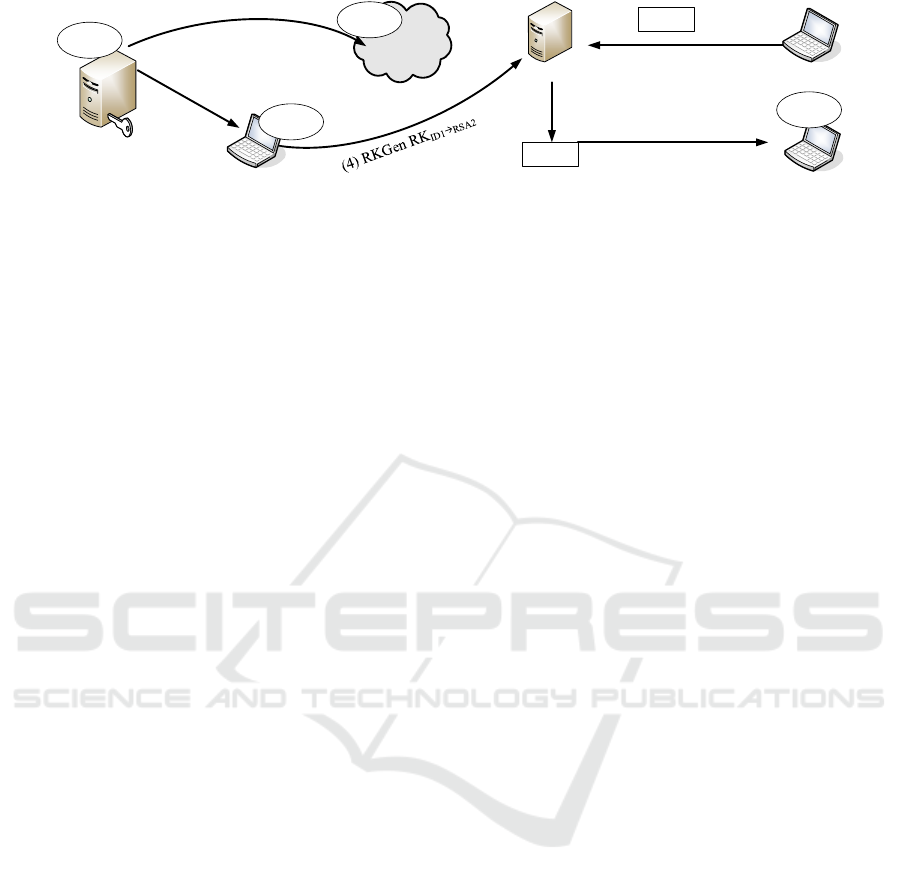
• RKGen: it is executed by the owner of the iden-
tifier ID1. It takes as input the SP, the secret key
SK
ID1
and an RSA public key RSA2 and generates
a (public) re-encryption key RK
ID1→RSA2
.
• Reencrypt: it is executed by a proxy. It takes
as input the SP, a re-encryption key RK
ID1→RSA2
,
and a ciphertext C
ID1
and outputs a new ciphertext
C
RSA2
.
ICT4AWE 2016 - 2nd International Conference on Information and Communication Technologies for Ageing Well and e-Health
128
ID2
(2) Extract SK
ID1
RSA
2
ID3
C
ID1
(3) Encrypt using ID1
Proxy
(5) Reencrypt using RK
ID1
ID2
C
ID2
(6) Decrypt using SK
RSA2
ID1
SK
ID1
(1) Setup
PKG
MSK
SP
Figure 2: IBE-PRE example.
• Decrypt: is is executed by the owner of the key
RSA2. It takes as input the SP, C
RSA2
, the corre-
sponding RSA private decryption key SK
RSA2
, and
returns the message M.
Figure 2 gives an example of a complete IBE-PRE
transaction. In this figure, initially the PKG generates
the MSK and the SP, and makes the SP publicly avail-
able (step 1). Then it extracts SK
ID1
and distributes it
to the corresponding user ID1 (step 2). Another user
creates a ciphertext using as a public key the string
ID1 and stores it in a proxy (step 3). This can only
be decrypted by the user that owns ID1, (and there-
fore knows the corresponding SK
ID1
). To allow a user
ID2 to decrypt the content using an RSA private key
RSA
2
, the user that owns ID1 creates a re-encryption
key RK
ID1→RSA2
and sends it to the proxy. The proxy
re-encrypts C
ID1
using the re-encryption key and gen-
erates C
RSA2
. The user ID2 is now able to decrypt
the re-encrypted ciphertext. The proxy learns nothing
about the contents of the ciphertext or the secret keys
of the users. Moreover, the scheme of Green and Ate-
niese assures the SK of the delegator (in this example,
SK
ID1
) is protected even if the proxy and the delegatee
collude.
If the original version of the scheme is used (in-
stead of the RSA variant) then all delegator-delegatee
pairs have to agree on the the same PKG. This how-
ever, raises security concerns, since PKGs will know
the private keys of both parties of a transaction. More-
over, if a delegatee interacts with many delegators (as
for example in the case of a hospital that interacts with
its patients) then this results in a non-negligible key
management overhead.
3 DESIGN
Our system assumes smart devices that collect user
related data (such as smart watches that measure car-
dio activity) and store them in a public Cloud. All
these devices interact with the Cloud through a user
controlled gateway. This gateway has the roles of the
PKG and ACP described in the previous section. All
communications (between the smart devices and the
gateway and between the gateway and the Cloud) are
secured using TLS. Data storage is implemented us-
ing the following steps:
• Initially the gateway executes the IBE-PRE setup
algorithms and generates the user’s master secret
key (MSK) and the corresponding (public) sys-
tem parameters. The MSK is then securely stored
in the gateway. Moreover, the gateway generates
a secret key (SK) that corresponds to the user’s
identity. The form and the semantics of a user
identity are application specific.
• The user defines access control policies specify-
ing the public keys that can access the data gener-
ated by each device. These policies are also stored
in the gateway. For each policy the gateway gen-
erates a URI of the form <gateway FQDN/access
control policy name>. We will refer to this URI
as URI
policy
.
• For each data item that arrives in the gateway, the
gateway generates a symmetric encryption key K,
encrypts the item using K (we refer to the output
as Enc(key)), and encrypts K using the IB-PRE
encrypt algorithm, with the user’s identity as input
(we refer to the output as C
ID
(K)).
• The gateway stores Enc(key), C
ID
(K), and
URI
policy
in the Cloud.
All potential clients that want to access some data
stored in the Cloud must have generated a pub-
lic/private key pair. The public part of this pair (which
we refer to as PK
client
) is the key used by data owners
when defining access control policies. Data access is
implemented using the following steps:
• The client sends a data request to the Cloud. The
Cloud responds with URI
policy
and a token.
• The client communicates with the gateway of the
user (located in gateway FQDN), and authenti-
cates himself. The authentication procedure is
application specific. For example, it can be im-
plemented by having the client digitally sign a
gateway-generated nonce using his private key.
When the authentication procedure is completed,
Protecting Medical Data Stored in Public Clouds
129

Smart device PKG
ACP
Gateway
Cloud
Client
Files
Data
Owner
Policies
File Request
Token, URI
Token, Authorisation Req.
Authorization, Re-key
Figure 3: Design overview.
and providing that the client is authorized to ac-
cess data items protected by URI
policy
, the gate-
way generates the appropriate authorization and
uses the IB-PRE RKGen algorithm to generate the
(public) re-encryption key RK
ID→PK
Client
.
• The client sends a new data request to the Cloud,
including this time the authorization and the re-
encryption key. The Cloud provider validates
the authorization, and if it is valid, it re-encrypts
C
ID
(K) and sends the new ciphertext along with
Enc(key) to the client.
• Provided that the client is indeed the owner of the
PK
client
used during the authentication process, he
is able to decrypt the re-encrypted version of K
and then use K to decrypt the file.
Figure 3 gives an overview of our system. It
should be noted that access control policies and re-
encryption keys are re-usable. Therefore, if a client,
authorized for a particular URI
policy
, requests another
item protected by the same policy, then communica-
tion with the gateway is not required.
3.1 Group Policies
It is often desirable to organize potential clients in
a group and define access control polices based on
these groups. For example, “doctors of hospital A”
could be considered a group. Contemporary crypto-
graphic techniques such as attributed-based encryp-
tion (Goyal et al., 2006), or hierarchical identity-
based encryption (Boneh et al., 2005) could be used to
achieve this goal. However, we do not consider this
option, because, for security reasons, we want each
client to be able to generate her keys by herself, which
is not possibly with these cryptographic techniques.
Instead, we follow a more conservative approach. We
assume that each group is identified by a public key.
This key is known to data owners and it is used dur-
ing access control definition. Moreover, each group
member has generated a public/private key pair. The
public part of this pair is included in a X.509 certifi-
cate which is digitally signed using the private key of
the group. For instance, in our example the public
keys of the doctors should be signed by the private
key of the group “doctors of hospital A”. If a client
belongs to multiple groups, he should have multiple
X.509 certificates.
When a client requests authorization from the
gateway, she includes in her request her digital certifi-
cate. The digital signature included in the certificate
is used by the gateway in order to evaluate whether or
not the client belongs to an authorized group. If this
is the case, then the gateway can use the public key of
the client (included in the certificate) to perform the
proxy re-encryption procedure described above, and
therefore to allow the user access to the data. Note
that the gateway does not need to know or store any
details about the members of the group; it only needs
to know the public key of the group.
4 EVALUATION
We have implemented the IB-PRE part of our sys-
tem by modifying the Green-Ateniese IBE-PRE
implementation included in the Charm Crypto li-
brary (Akinyele et al., 2013) to support RSA public
keys for the delegatee. In order to achieve a security
level equivalent to RSA with a key size of 1024 bits
for the encryption of the symmetric key, the size of
C
ID
(key) is 3232 bits, and the size of a re-encryption
key is 1536 bits. In an Ubuntu 12.04 Desktop ma-
chine, running in a single core of an Intel i5-4440
3.1 GHz processor with 2GB of RAM, the creation
of C
ID
(key) required 40 ms, the creation of a re-
encryption key required 20 ms, the re-encryption of
a ciphertext required 31 ms, and the decryption of a
ciphertext required 28 ms.
The IB-PRE cryptographic algorithm used by our
system has been proven to be secure in (Green and
Ateniese, 2007). Moreover, the access control dele-
ICT4AWE 2016 - 2nd International Conference on Information and Communication Technologies for Ageing Well and e-Health
130

gation solution used by our system exhibits many ad-
vantages: it is generic enough, it can be easily im-
plemented by a Cloud provider, data can be easily
transferred between Cloud providers that implement
this solution, it protects client privacy against third
parties (including the Cloud providers), and it allows
easy modification of access control policies (Fotiou
et al., 2015).
Each data item is encrypted using a different sym-
metric encryption key, therefore, the compromise of
a symmetric encryption key would require the re-
encryption of that specific item only with another
fresh key. This is an inevitable overhead of all sim-
ilar systems and it is due to the fact that public key
encryption cannot be applied directly to the file con-
tents, due to its computation complexity. Neverthe-
less, for small data items, such as readings from wear-
able devices, it may be possible to negate the need for
symmetric encryption.
5 RELATED WORK
L
¨
ohr et al. (L
¨
ohr et al., 2010) have proposed a solution
for securing e-health clouds based on Trusted Virtual
Domains (TVDs). TVD is a virtualization technique
that creates secure “sandboxes” where user data can
reside. This solution is orthogonal to our system: the
solution by L
¨
ohr et al. concerns the design of secure
clouds specific to e-health services, whereas our so-
lution assumes a generic cloud service and builds a
secure data sharing system on top of it.
Wu et al. (Wu et al., 2012) propose an access con-
trol mechanism for sharing electronic health records
in the Cloud. The main component of their mecha-
nism is an access broker that is responsible for en-
forcing access control policies. The access broker is
an entity shared among many stakeholders, therefore,
privacy concerns are raised. In our work, access con-
trol policies are enforced by data owners in a way that
reveals no information about data owners or clients
to third parties (including the Cloud provider). Son
et al. (Son et al., 2015) propose a mechanism that
supports “dynamic” access control, i.e., access con-
trol that takes into consideration the user’s context.
In their solution, access control is also implemented
in the Cloud, therefore the same privacy concerns are
raised.
Fabian et al. (Fabian et al., 2015) use attribute-
based encryption (ABE) to protect medical data
stored in multi-Cloud environments and shared
among different cooperative organizations. ABE pro-
duces encrypted data in a way that only users with
specific “attributes” can decrypt. In essence, ABE
incorporates access control policies into ciphertexts.
The disadvantage of using ABE for this purpose is
that the loss of a private key that corresponds to an at-
tribute requires the generation of a new key, the distri-
bution of this key to all users that have this attribute,
and the appropriate encryption of all files protected
by this attribute. In contrast, in our system the loss
of the data owner’s secret key only requires a new en-
cryption of all symmetric keys. Similarly, (Li et al.,
2013), (Liu et al., 2015) use attribute-based encryp-
tion to protect personal health records stored in public
cloud environments; these solution also suffer from
the same problems.
Thilakanathan et al. (Thilakanathan et al., 2014)
use ElGamal public key encryption and a proxy re-
encryption like protocol to protect generic health data
stored in the cloud. Their solution relies on a cen-
tralized trusted third party that generates private keys
on behalf of users. In our system users generate their
private keys by themselves, therefore our approach of-
fers increased security.
6 CONCLUSION AND FUTURE
WORK
In this paper we presented a solution that allows se-
cure and privacy preserving storage of medical data
in public Clouds, by leveraging access control dele-
gation and proxy re-encryption. Our solution is based
on a gateway-based design, where a user controlled
gateway is responsible for encrypting user generated
data, as well as for enforcing access control policies.
Future work involves the transfer of the encryp-
tion process to the devices that generate the data. In
this manner, the device could store the data directly
to the Cloud, avoiding the gateway, therefore reduc-
ing communication overhead. Currently, our work as-
sumes that devices can be securely authenticated to
the gateway and, similarly, the gateway can be se-
curely authenticated to the Cloud. Future enhance-
ments of our system would also consider and imple-
ment these functions.
REFERENCES
Akinyele, J., Garman, C., Miers, I., Pagano, M., Rushanan,
M., Green, M., and Rubin, A. (2013). Charm:
a framework for rapidly prototyping cryptosystems.
Journal of Cryptographic Engineering, 3(2):111–128.
Boneh, D., Boyen, X., and Goh, E.-J. (2005). Hierarchical
identity based encryption with constant size cipher-
text. In Cramer, R., editor, Advances in Cryptology
Protecting Medical Data Stored in Public Clouds
131

EUROCRYPT 2005, volume 3494 of Lecture Notes
in Computer Science, pages 440–456. Springer Berlin
Heidelberg.
Fabian, B., Ermakova, T., and Junghanns, P. (2015). Collab-
orative and secure sharing of healthcare data in multi-
clouds. Information Systems, 48:132 – 150.
Fotiou, N., Machas, A., Polyzos, G. C., and Xylomenos,
G. (2015). Access control as a service for the cloud.
Journal of Internet Services and Applications, 6(1):1–
15.
Goyal, V., Pandey, O., Sahai, A., and Waters, B. (2006).
Attribute-based encryption for fine-grained access
control of encrypted data. In Proceedings of the 13th
ACM Conference on Computer and Communications
Security, CCS ’06, pages 89–98, New York, NY, USA.
ACM.
Green, M. and Ateniese, G. (2007). Identity-based proxy re-
encryption. In Katz, J. and Yung, M., editors, Applied
Cryptography and Network Security, volume 4521 of
Lecture Notes in Computer Science, pages 288–306.
Springer Berlin Heidelberg.
Li, M., Yu, S., Zheng, Y., Ren, K., and Lou, W. (2013).
Scalable and secure sharing of personal health records
in cloud computing using attribute-based encryption.
Parallel and Distributed Systems, IEEE Transactions
on, 24(1):131–143.
Liu, J., Huang, X., and Liu, J. K. (2015). Secure shar-
ing of personal health records in cloud computing:
Ciphertext-policy attribute-based signcryption. Fu-
ture Generation Computer Systems, 52:67 – 76. Spe-
cial Section: Cloud Computing: Security, Privacy and
Practice.
L
¨
ohr, H., Sadeghi, A.-R., and Winandy, M. (2010). Secur-
ing the e-health cloud. In Proceedings of the 1st ACM
International Health Informatics Symposium, IHI ’10,
pages 220–229, New York, NY, USA. ACM.
Son, J., Kim, J.-D., Na, H.-S., and Baik, D.-K. (2015).
Dynamic access control model for privacy preserving
personalized healthcare in cloud environment. Tech-
nology and Health Care, 24(s1):S123–S129.
Thilakanathan, D., Chen, S., Nepal, S., Calvo, R., and
Alem, L. (2014). A platform for secure monitoring
and sharing of generic health data in the cloud. Future
Generation Computer Systems, 35:102 – 113. Special
Section: Integration of Cloud Computing and Body
Sensor Networks; Guest Editors: Giancarlo Fortino
and Mukaddim Pathan.
Wu, R., Ahn, G.-J., and Hu, H. (2012). Secure sharing of
electronic health records in clouds. In Collaborative
Computing: Networking, Applications and Workshar-
ing (CollaborateCom), 2012 8th International Con-
ference on, pages 711–718.
ICT4AWE 2016 - 2nd International Conference on Information and Communication Technologies for Ageing Well and e-Health
132
