
Predicting the Risk Associated to Pregnancy using Data Mining
Andreia Brandão, Eliana Pereira, Filipe Portela, Manuel Santos, António Abelha
and José Machado
ALGORITMI Research Centre, Universidade do Minho, Guimarães, Portugal
Keywords: Data Mining, Intelligent Decision Support Systems, Voluntary Interruption of Pregnancy, Business
Intelligence, Technology Acceptance.
Abstract: Woman willing to terminate pregnancy should in general use a specialized health unit, as it is the case of
Maternidade Júlio Dinis in Porto, Portugal. One of the four stages comprising the process is evaluation. The
purpose of this article is to evaluate the process of Voluntary Termination of Pregnancy and, consequently,
identify the risk associated to the patients. Data Mining (DM) models were induced to predict the risk in a
real environment. Three different techniques were considered: Decision Tree (DT), Support Vector Machine
(SVM) and Generalized Linear Models (GLM) to perform the classification task. Cross-Industry Standard
Process for Data Mining (CRISP-DM) methodology was applied to drive this work. Very promising results
were obtained, achieving a sensitivity of approximately 93%.
1 INTRODUCTION
The use of Information and Communication
Technologies (ICT) are increasingly, occupying an
important place in society. The health sector is no
exception, as these among other things, can provide
complete and reliable information for healthcare
professionals, allowing support to their clinical and
administrative decisions and consequently
decreasing medical errors associated with these
decisions (Pinto, 2009).
An example of a clinical system focused on
nursing practice it is the Nursing Practice Support
Systems - SSNP a.k.a SAPE. SAPE was created
with the goal of giving visibility to the work done by
nursing professionals, since these are the users who
produce, process and deliver most clinical
information (Pinto, 2009).
SAPE is currently used in Centro Hospital of
Porto (CHP) and consequently in Centro Materno
Infantil do Norte (CMIN) to support nursing
practice. In CMIN, the Voluntary Interruption of
Pregnancy (VIP) process is a focus of nursing. The
patient clinical data records as well as the entire
process of VIP are supported by SAPE, making it
therefore possible to use this information to extract
useful knowledge in the context of Pregnancy
Termination (PT).
In this case, it is possible to apply Data Mining
(DM) to process the data stored, extracting useful
knowledge in order to support clinical decisions
based on evidence, as the case of the PT procedure
(Bonney, 2013). This process is composed by four
steps, where the first step is a medical appointment
to verify if the patient is aware of her decision. If she
decides to move on, the next two steps are the drug
administration and the last step consists of the
evaluation process. In this last step of the process, a
revision consultation is usually done.
Focusing only on the last step, revision
consultation, which is characterized by scheduling a
consultation with a physician, four possible
situations can occur: VIP was achieved; VIP was not
achieved; VIP is incomplete and finally the patient
did not appear at the revision consultation.
Having regarded this procedure, the purpose of
this article is the use of Data Mining techniques,
namely classification models to study the final stage
of the VIP process and consequently identify the risk
group. This group is characterized by patients who
do not appear at the revision consultation and cannot
successfully perform the PT procedure.
Besides the introduction, this article includes six
sections. The second section is related to the
background and related work, which describes the
process of VIP and a brief look is taken at the
Interoperability System. Subsequently, in section
three, the process of Knowledge Discovery in
Databases and the method of CRISP-DM, based on
594
Brandão A., Pereira E., Portela F., Santos M., Abelha A. and Machado J..
Predicting the Risk Associated to Pregnancy using Data Mining.
DOI: 10.5220/0005286805940601
In Proceedings of the International Conference on Agents and Artificial Intelligence (ICAART-2015), pages 594-601
ISBN: 978-989-758-074-1
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)

the previous is described; the DM techniques used
and the statistical metric applied. In the fourth
section, each stage of CRISP-DM method is
described while the remaining two sections are the
discussion and the conclusion.
2 BACKGROUND AND RELATED
WORK
2.1 Voluntary Interruption of
Pregnancy
In CMIN, the medication methods are used to
perform the PT process. This process consists on the
administration of specific drugs, in particular
mifepristone and misoprostol.
Furthermore, it is a procedure that involves
several steps. The first phase consists in a
physician’s appointment followed by a period of
three days, where the patient needs to consider her
decision. Then, the patient receive a medication
dosage performed in the CMIN ambulatory. A triage
is also executed by the nursing staff in order to
verify if the patient is capable to administrate the
second medication dosage at home or if she needs to
be monitored by the nursing team in CMIN.
After the medication administration phase, a new
clinical consultation is performed, where the patient
is examined in order to determine whether the
procedure was successful. If the opposite occurs, the
PT was not achieved or the procedure was
incomplete (resulting in the patient admission)
(Valente et al., 2012).
In this last phase, two situations may occur: the
patient is consulted and she is examined by the
physician or the patient does not attend to the
consultation. In the first case, the patient is evaluated
and it is reported if PT was successful. On the other
hand, if it was verified ovular remains by ultrasound
(incomplete PT), it is necessary to hospitalize the
patient. Then if the PT was not achieved, it is
necessary to repeat the process.
In the second case, the patient was not evaluated,
consequently their condition and the procedure
result remains unknown. This situation characterizes
who are the risk patients. By the fact that it can
originates some problems, in particular, health risks
associated to the patient and to the fetus due lacking
of medical supervision. Sometimes it constitutes a
waste of resources for these patients, since all drugs
are reimbursed by the Portuguese State and the
entire PT procedure is quite expensive (on average
one PT costs 700 euros to the National Health
Service).
In maternity care and particular in the VIP
module, the use of DM can be considered scarce. So
the models studied in this paper can be seen as an
innovation in this area and can be used in a Decision
Support System for health professionals. To develop
this work some Oracle tools (Database and Data
Mining) were used.
2.2 Interoperability System
This work, like all the others processes of
knowledge extraction in the CHP was possible due
to the fact there is in the CHP, the Agency for
Integration, Archive and Diffusion of Medical
Information (AIDA) is implemented. AIDA is based
on the use of intelligent agents, allowing the
interoperability among the existing systems. This
multi-agent system enables the standardization of
clinical systems and overcomes the medical and
administrative complexity of the different sources of
information from the hospital (Peixoto et al., 2012).
The SAPE resulted from the Nursing Information
Systems, as an alternative to the traditional way of
information on paper and its design in functional
terms. It was developed at the Escola Superior de
Enfermagem do São João by Nurse Abel Paiva
(Pinto, 2009), (O’Sullivan et al., 2008).
3 KNOWLEDGE DISCOVERY
AND DATA MINING
3.1 Knowledge Discovery in Database
The Knowledge Discovery in Database (KDD) is a
set of on going activities that enable the extraction of
useful knowledge. The main goal of KDD is to
discover useful, valid, relevant and new knowledge
about a particular activity through algorithms, taking
into account the magnitudes of data increasing
(Goebel, Siekmann and Wahlster, 2008).
This process can be resumed in five steps (Cios,
2007):
Selection: Occurs the selection of the dataset
that was needed to run the DM. For this case,
data from AIDA and SAPE were used.
Pre-processing: This step includes cleaning and
processing of data, with the aim of making
them consistent. For example, the elimination
of null values.
PredictingtheRiskAssociatedtoPregnancyusingDataMining
595
Transformation: At this stage, the data were
processed with the ultimate goal of making
them uniform. For example, the change in
attributes with continuous values for attributes
with discrete values;
Data Mining: According to the type of the
desired result, the type of task being performed
was defined and the technique to be used was
identified. In this case, the classification task
was applied and the SVM, GLM and DT
techniques were used.
Interpretation/Evaluation: Consist of the
interpretation and evaluation of the patterns
obtained (Palaniappan and Awang, 2008).
3.2 Cross Industry Standard Process
for Data Mining (CRISP-DM)
The DM methodology that addressed this paper was
the Cross Industry Standard Process for Data Mining
(CRISP-DM) methodology, because of its
characteristics:
It is an independent tool;
It is industry independent - The same process
can be applied to analyse business, financial
data, human resources, manufacturing,
services, etc.;
There is a relationship with the models in the
KDD process.
The CRISP-DM breaks the process of Data
Mining into six main phases (Catley et al., 2006),
(Chattopadhyay et al., 2008), (Frawley et al.,1992):
Business Understanding, Data Understanding, Data
preparation, Modelling, Evaluation and
Implementation.
3.3 Data Mining Techniques
In this work, the following DM techniques were
used:
Decision Tree (DT): DT generates rules
automatically, which are conditional statements
that reveal the logic used to build the tree.
Generalized Linear Models (GLM): GLM is a
statistical technique for linear modelling. GLM
is usually implemented for binary
classification.
Support Vector Machine: SVM is a powerful
algorithm based on linear and nonlinear
regression. SVM is usually implemented for
binary and multiclass classification.
Naïve byes (NB): is based on applying Bayes'
theorem with strong independence assumptions
between the features. Although NB also was
explored, the obtained results were very weak,
consequently there were not presented in this
paper.
3.4 Assessment Measures
Through the Confusion Matrix, resulting from the
application of DM techniques, four types of results
were obtained: a true positive (TP) result that
corresponds to the number of positive examples
correctly classified; the false positive (FP) result that
corresponds to the number of positive examples
classified as negative; the true negative (TN) result,
that corresponds to the number of negative examples
actually classified as negative and, finally, the false
negative (FN), that corresponds to the number of
negative examples classified as positive.
From this type of values, statistical metrics can
be estimated: sensitivity, which is the ability to
correctly detect the occurrence of the procedure;
specificity that is the ability to correctly identify in a
model the non-occurrence of a procedure; and
accuracy that is the total percentage of agreement
between the values detected correctly and the actual
values (Chapman et al., 2000).
Table 1 presents the expression that characterizes
the metrics described.
Table 1: Expressions that define the statistical measures.
Sensitivity Specificity Accuracy
4 DATA MINING PROCESS
CRISP-DM is considered a complex process, but
when applied to a certain problem becomes easier to
understand, implement and develop. This
methodology was used in this case study. Then it is
presented all the stages of the process described in
section Cross Industry Standard Process for Data
Mining (CRISP-DM).
4.1 Business Understanding
The process comprises two VIP phases of
administering medication that are followed by a
medical examination. This examination evaluates
whether this process was successful or not.
However, there is a group of patients who cannot
ICAART2015-InternationalConferenceonAgentsandArtificialIntelligence
596
attend to this appointment and, therefore, are
considered a risk group. This is due to not having
any information about these patients and the current
health state of her or the fetus being unknown.
Thus, a problem was formulated: "How can be
predicted whether a patient belongs to the risk
group of patients?”.
This question can be translated into a DM
problem: "What is the probability of a patient
belonging to the risk group of patients?”.
A model that predicts whether a woman is
considered a risk patient should be constructed based
on the data that were previously recorded in the VIP
process.
Prior to the development of the model, data
associated to the attributes which establish a
relationship between the patient and the group of
women who did not attend to the evaluation
appointment must be selected.
4.2 Data Understanding
This phase includes the extraction of data from
SAPE and AIDA using intelligent agents and an
analysis of the variables to be used in this DM
problem. The extracted data cover the period from
01.01.2012 to 31.12.2012. The amount of data used
reaches a number of 1124 records/pregnant. Each
record is contains the fields:
Age: corresponds to the age of the patient
who will perform VIP procedure;
Number of previous VIP (N_VIP): this
variable sets the number of times the patient
underwent the process of VIP previously;
Gesta: corresponds to the number of previous
pregnancies of the woman;
Para: corresponds to the number of births
that the woman had;
Professional Status (PS): this variable
informs if the pregnant woman in question is
employed or not.
Achieved PT (AA): this variable informs if the
PT procedure was achieved or not.
Failed PT (FA): this variable informs if the
PT procedure has failed or not.
Incomplete PT (IA): this variable informs if
the PT procedure was incomplete or not.
Revision Consultation (RC): this variable
informs if the patient attended to the revision
consultation or not;
Contraceptive Method (CM): the variable
informs if the pregnant woman had used (1) a
contraceptive method or not (0);
Weeks of Gestation (WG): corresponds to the
weeks of the gestation of the pregnant
woman, when she arrived to CMIN.
A statistical analysis has shown that the data had
quality; however they needed to be transformed in
order to be incorporated into the DM models.
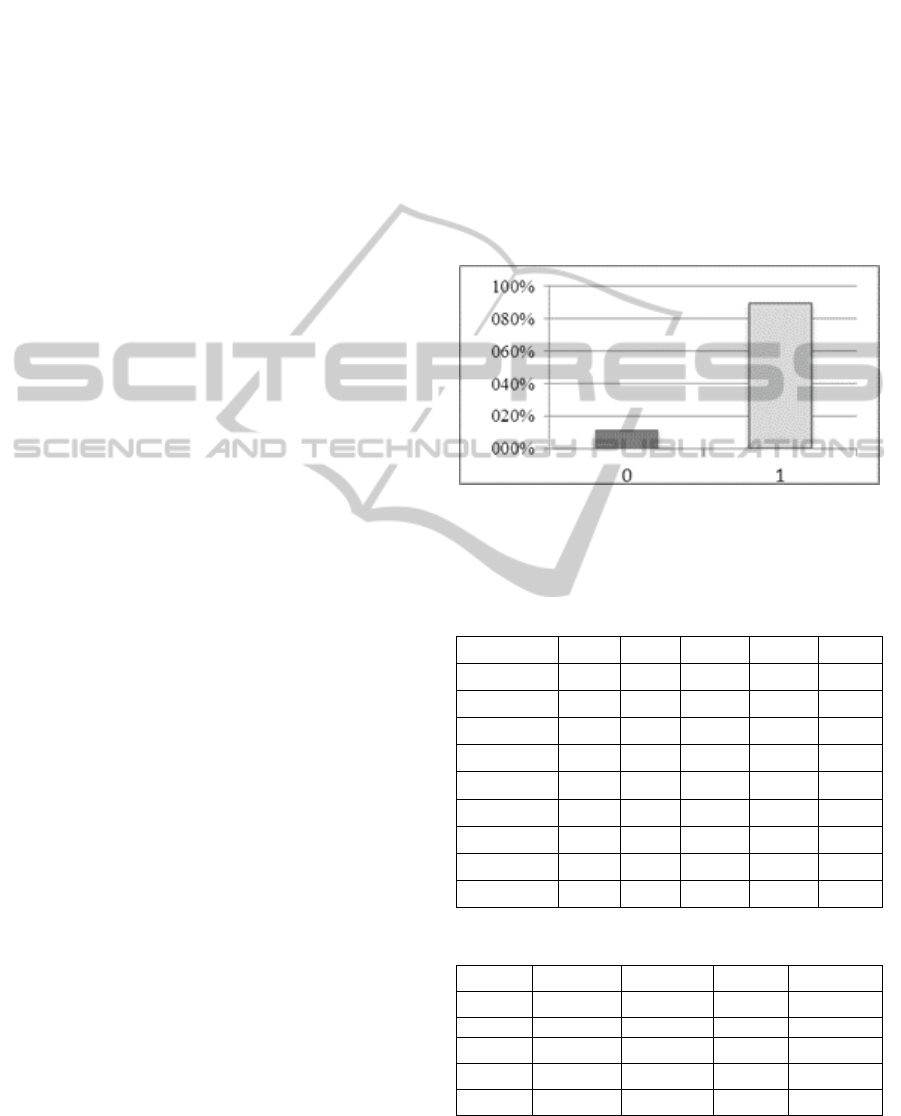
Figure 1 illustrates the target variable Revision
Consultation distribution (percentage). As can be
seen from this figure, about 10% of patients do not
attend to the revision consultation. In the table 2
some statistical measures related to the numerical
variables are presented, while in table 3 the
percentage of occurrences (number) for each one of
the selected variables is shown.
Figure 1. Distribution of values of the target variable
Revision Consultation, which may take the values attended
(1) or not attended (0).
Table 2: Statistics measures of N_VIP, WG, Age, Gesta
and Para variables.
Number
CM PS N_VIP Para Gesta
0 38.79
53.11 82.36 48.78 41.58
1 61.21
26.55 14.58 27.90 24.75
2
20.34 2.43 17.82 19.80
3
0.36 4.59 9.18
4
0.27 0.63 2.61
5
0.09 1.08
6
0.09 0.45
8
0.09 0.36
9
0.18
Table 3: Percentage of occurrences of some variables.
Minimum Maximum Average stDev
N_VIP 0 4 0.22 0.52
WG 3 10.40 7.16 1.46
Age 13
46 27.43 6.95
Gesta 1
9 2.14 1.30
Para 0
8 0.82 0.98
PredictingtheRiskAssociatedtoPregnancyusingDataMining
597
4.3 Data Preparation
At this stage the variables that suited the problem,
based on the variables defined in the previous
subsection were selected. Thus, the variables
Revision Consultation, Gesta, Para, Professional
Status, Number of Previous VIPs, Age,
Contraceptive Method and Weeks of Gestation were
used in this problem of DM. Subsequently, the
selected data were subjected to a pre-processing
phase where all the records containing unfilled or
noise fields were eliminated. After this processing,
there were used only 1119 entries.
Some of the procedures performed to eliminate
noise from the data were the replacement of the
comma by point to separate the decimals on Weeks
of Gestation variable, the elimination of the text
associated to the numerical variables and also the
assignment of numerical values to the variable
Professional Status, where the value 0 is associated
with unemployment, the value 1 is associated with
employment and value 2 is assigned to the students.
After those transformations of the data, the table
of cases with some of the scenarios considered most
suitable was built. In a second phase of data
preparation, a simple oversampling task was
performed in an attempt to obtain better results.
Thus, the data was stratified by the target (all rows
with 1) and then it was replicated as a package,
several times with the goal of balancing the
occurrence of target variable (0 and 1). With this
operation the dataset maintained their structure.
Thus, the oversampling task consisted of a
replication of cases of class "1", i.e. the set of cases
"1" has been replicated as many times as necessary
until the two elements (“0” and “1”) had a value of
approximately cases. This process raised the total
number of records up to 1959 (49% for class "0" and
51% for class "1").
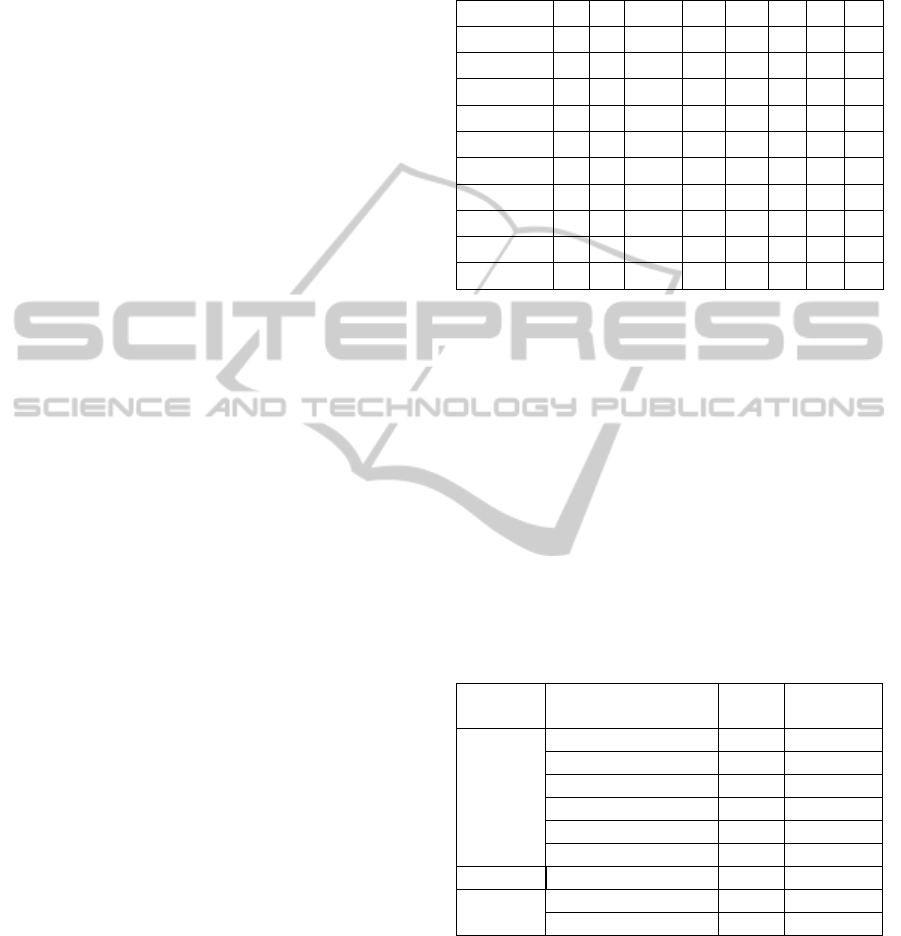
4.4 Modelling
In this step, a table of scenarios (table 4) were built,
where are represented the 10 scenarios that yielded
the best results, arising from different combinations
of variables. These scenarios were conceived
making use of domain knowledge provided by the
clinicians. In each scenario, the target variable RC is
presented, as well as other variables considered
crucial to the creation of forecast models. After
defined the table 4, the data were submitted to DM
techniques, selected in order to be able to identify
the best forecasting model for this DM problem. In
this case, the DM techniques used were GLM, SVM
and DT.
Table 4: Representation of the variables used in each of
the models.
RC Age
N_VIP
Gesta Para PS CM WG
Scenario 1 X X X X X X X X
Scenario 2 X X
X X X X X -
Scenario 3 X X
X X X X - -
Scenario 4 X X
X X X - - -
Scenario 5 X X
X - - - - -
Scenario 6 X X
X X X X - X
Scenario 7 X X
X X X - - X
Scenario 8 X X
X X X - X X
Scenario 9 X X
X X X - X -
Scenario 10 X X
X - - - X X
Each model, resulting from the application of a
particular technique for a given DM scenario can be
defined by a tuple:
= <A
f
, S
i
, TDM
y
>
The model
belongs to the classification approach
(A) and it is composed by a scenario (S)
{S1 – S10}
and a DM technique (TDM) - {GLM, DT, and
SVM}. For this DM problem they were induced 60
models were generated, also taking into account the
models based on the oversampling dataset. This total
amount of models resulted from 10 scenarios x 1
target x 3 TDM x 2 approaches. Table 5 presents the
configurations used in the DM models.
Table 5. Configuration of DM Techniques.
Technique
Setting
Name
Setting
Value
Setting
Type
DT Minrec Node 10 Input
Max Depth 7 Input
Minpct Split 0.1 Input
Impurity Metric Gini Input
Minrec Split 20 Input
Minpct Node 0.05 Input
GLM Coefficient level 0.95 Default
SVM Conv tolerance .001 Input
Active learning Enable Input
4.5 Evaluation
For the evaluation of the obtained results in DM
models, an assessment metric has been taken into
account, namely sensitivity.
This measure assesses the ability to correctly
detect the occurrence of a procedure. It is therefore
the most appropriate metric for evaluating the
ICAART2015-InternationalConferenceonAgentsandArtificialIntelligence
598
models, since the ultimate goal is to detect the
occurrence of patients with a strong probability of
belonging to the risk group. At this stage, the top
three models were selected for each one of the
scenarios and DM techniques.
They are represented in table 6. Using the data
obtained from the second phase of data preparation,
the techniques of DM used in the first approach were
applied again.
For these results, statistical metrics were
calculated, including sensitivity, specificity and
accuracy for the best models obtained previously
(present in the table 6), as shown in the table 7.
Analysing the two tables it is possible to observe
that the values of the sensitivity decreased, however
the oversampling approach yielded better values for
specificity and accuracy. This happens due to a most
balanced number of cases in the target variable.
Table 6: Sensitivity, specificity and accuracy values of the
top 3 models from the first approach.
SVM GLM DT
Sensitivity Sensitivity Sensitivity
Model 4 0.929 Model 4 0.925 Model 4 0.926
Model 7 0.924 Model 5 0.929 Model 5 0.926
Model 10 0.926 Model 9 0.923 Model 9 0.926
Specificity Specificity Specificity
Model 4 0.100 Model 4 0.093 Model 4 0.090
Model 7 0.093 Model 5 0.092 Model 5 0.090
Model 10 0.101 Model 9 0.092 Model 9 0.090
Accuracy Accuracy Accuracy
Model 4 0.574 Model 4 0.543 Model 4 0.446
Model 7 0.583 Model 5 0.437 Model 5 0.446
Model 10 0.631 Model 9 0.579 Model 9 0.446
Table 7: Sensitivity, specificity and accuracy values to the
top 3 models for each algorithm, using oversampling.
SVM GLM DT
Sensitivity Sensitivity Sensitivity
Model 4 0.644 Model 4 0.594 Model 4 0.873
Model 7 0.693 Model 5 0.645 Model 5 0.524
M
odel 10 0.608 Model 9 0.595 Model 9 0.873
Specificity Specificity Specificity
Model 4 0.753 Model 4 0.613 Model 4 0.524
Model 7 0.650 Model 5 0.579 Model 5 0.524
M
odel 10 0.822 Model 9 0.614 Model 9 0.524
A
ccuracy
A
ccuracy
A
ccuracy
Model 4 0.680 Model 4 0.602 Model 4 0.555
Model 7 0.670 Model 5 0.605 Model 5 0.555
M
odel 10 0.657 Model 9 0.603 Model 9 0.555
4.6 Deployment
The extracted knowledge by inducing DM models so
as their availability and the way of how the
information is presented (through a BI platform),
were well accepted by the health professionals.
Depending on the requirements, this information
may be available through simple or complex reports
and can lead to the implementation of a process of
repeated DM. In this particular case, the processes of
DM are intended to be integrated in the BI platform
of CHP.
5 DISCUSSION
After the application of the CRISP-DM
methodology, it was possible to verify that the
models are quite acceptable, based on the results
presented in subsection evaluation. For the induced
models the best prediction result obtained based on
the sensitivity metric it was approximately 93%. In
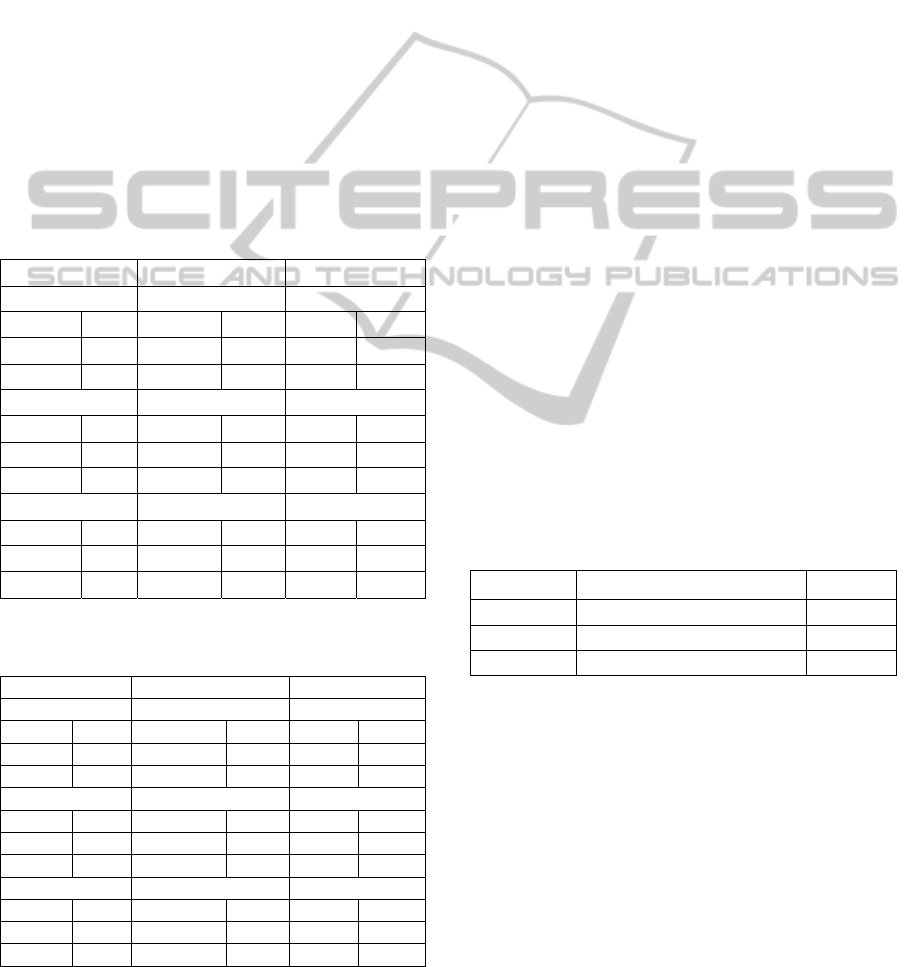
the table 8, the top 3 models are shown.
As can be seen in table 8, the top three models,
taking in consideration the sensitivity values, are the
models 4, 5 and 9. Thus, it can be considered that
the Decision Tree was one of the best DM
techniques applied, considering that the attributes
that best characterize the possible patients in the risk
group are Age, Number of Previous VIPs, Gesta and
Para.
Table 8: The best DM models obtained and the respective
technique used.
Models
DM Technique Sensitivity
Model 4 Support Vector Machine 0.929
Model 5 Generalized Linear Model 0.929
Model 9 Decision Tree 0.926
Moreover, the results from the second approach,
showing a balance in the occurrences of “0” and
“1”, give more uniform target models, where the
ability to correctly detect the patients belonging to a
risk group is identical to the ability of detecting
patients who do not belong to the same group.
In conclusion, the results obtained for predicting
the risk group of patients, based on the presence or
absence of the patient in the revision consultation
can be considered satisfactory. The oversampling
technique reveals not be a good choice because
when the models are using sensitive data as it is
clinical information it can compromise the data
significance.
PredictingtheRiskAssociatedtoPregnancyusingDataMining
599

Thus, the prediction models obtained can be used
for supporting decision-making process of the
nursing team responsible for the VIP process.
Nurses can take into account a priori the
characteristics that identify a woman who belongs to
the risk group, getting an idea if the patient is a
possible “member” of this group, and consequently
take preventive measures to these patients.
6 CONCLUSION AND FUTURE
WORK
This study demonstrated that it is possible to obtain
DM classification models to predict which patient
belongs to the risk group in the VIP process. The
study was conducted using real data inherent to the
VIP process, corresponding to 1 year of activity in
CMIN.
Good results were achieved in terms of
sensitivity, being approximately 93%, in the model 4
using Support Vector Machines. The most relevant
factors to determine the risk group are the patient's
age, the number of previous VIPs, the number of
previous pregnancies (Gesta) and the number of
previous births (Para). It can be concluded that, with
the use of classification techniques applied to
historical data from pregnant women who underwent
in the process of VIP, can be predicted if a patient
fits the features of a VIP risk group.
The results are important for a possible redesign
of the VIP protocol implemented on CMIN. These
models allow improving the service, increasing the
number of successes and decrease the costs. At same
time can be applied to other institutions with the
same problem / protocols.
According to the health professionals these
models are very interesting and useful to support the
decision when a women wants to make a VIP.
This type of research can promote future
developments related with this particular area of
maternity care.
ACKNOWLEDGEMENTS
”This work is funded by National Funds through the
FCT – Fundação para a Ciência e a Tecnologia
(Portuguese Foundation for Science and
Technology) within project PEstOE/EEI/UI0752/
2014 and PEst-OE/EEI/UI0319/2014”.
REFERENCES
Abelha, A., Analide, C., Machado, J., Neves, J., & Novais,
P. (2007). Ambient Intelligence and Simulation in
Health Care Virtual Scenarios, 243, 461–468.
Bonney, W. (2013). Applicability of Business Intelligence
in Electronic Health Record. Procedia - Social and
Behavioral Sciences, 73, 257–262.
doi:10.1016/j.sbspro.2013.02.050.
Catley, C., Frize, M., Walker, C. R., & Petriu, D. C.
(2006). Predicting High-Risk Preterm Birth Using
Artificial Neural Networks. IEEE Transactions on
Information Technology in Biomedicine, 10(3), 540–
549. doi:10.1109/TITB.2006.872069.
Chapman, P., Clinton, J., Kerber, R., Khabaza, T.,
Reinartz, T., Shearer, C., & Wirth, R. (2000). The
CRISP-DM User Guide. NCR Systems Engineering
Compenhagen. Brussels: NCR Systems Engineering
Copenhagen.
Chattopadhyay, S., Ray, P., Chen, H. S., Lee, M. B., &
Chiang, H. C. (2008). Suicidal Risk Evaluation Using
a Similarity-Based Classifier. In C. Tang, C. Ling, X.
Zhou, N. Cercone, & X. Li (Eds.), Advanced Data
Mining and Applications SE - 7 (Vol. 5139, pp. 51–
61). Springer Berlin Heidelberg. doi:10.1007/978-3-
540-88192-6_7.
Cios, K., Pedrycz, W., Swiniarski, R., & Kurgan, L.
(2007). Data Mining. A knowledge Discovery
Approach. Springer.
Goebel, R., Siekmann, J., & Wahlster, W. (2008).
Advances in Knowledge Discovery and Data Mining.
Springer.
Gonçalves, J., Portela, F., Santos, M. F., Silva, Á.,
Machado, J., Abelha, A., & Rua, F. (2013). Real-time
Predictive Analytics for Sepsis Level and Therapeutic
Plans in Intensive Care Medicine. International
Information Institute.
O’Sullivan, D., Elazmeh, W., Wilk, S., Farion, K.,
Matwin, S., Michalowski, W., & Sehatkar, M. (2008).
Using Secondary Knowledge to Support Decision
Tree Classification of Retrospective Clinical Data. In
Z. Raś, S. Tsumoto, & D. Zighed (Eds.), Mining
Complex Data SE - 19 (Vol. 4944, pp. 238–251).
Springer Berlin Heidelberg. doi:10.1007/978-3-540-
68416-9_19.
Palaniappan, S., & Awang, R. (2008). Intelligent Heart
Disease Prediction System Using Data Mining
Techniques. In Proceedings of the 2008 IEEE/ACS
International Conference on Computer Systems and
Applications (pp. 108–115). Washington, DC, USA:
IEEE Computer Society.
doi:10.1109/AICCSA.2008.4493524.
Peixoto, H., Santos, M., Abelha, A., & Machado, J.
(2012). Intelligence in Interoperability with AIDA. In
L. Chen, A. Felfernig, J. Liu, & Z. Raś (Eds.), Lecture
Notes in Computer Science, Foundations of Intelligent
Systems - 31 (Vol. 7661, pp. 264–273). Springer
Berlin Heidelberg. doi:10.1007/978-3-642-34624-
8_31.
ICAART2015-InternationalConferenceonAgentsandArtificialIntelligence
600

Pinto, L. (2009). Sistemas de informação e profissionais
de enfermagem. Universidade de Trás-Os-Montes e
Alto Douro.
Razavi, A., Gill, H., Åhlfeldt, H., & Shahsavar, N. (2007).
Predicting Metastasis in Breast Cancer: Comparing a
Decision Tree with Domain Experts. Journal of
Medical Systems, 31(4), 263–273.
doi:10.1007/s10916-007-9064-1.
Valente, C., Cristina, T., Rosário, F., & Alcina, B. (2012).
Acompanhamento de enfermagem na interrupção da
gravidez por opção da mulher ( I.G.O.). Porto.
PredictingtheRiskAssociatedtoPregnancyusingDataMining
601
