
Automated Personalized Goal-setting in an Activity Coaching
Application
Miriam Cabrita
1,2
, Harm op den Akker
1,2
, Reinoud Achterkamp
1,2
, Hermie Hermens
1,2
and Miriam Vollenbroek-Hutten
1,2
1
Roessingh Research and Development, Telemedicine Group,
Enschede, The Netherlands
2
University of Twente, Faculty of Electrical Engineering and Computer Science, Telemedicine Group,
Enschede, The Netherlands
Keywords:
Accelerometers, Physical Activity, Goal-setting, Personalization, Telemedicine, Body Area Networks.
Abstract:
The ageing population and the increase in sedentary lifestyles of knowledge workers has led to increasing
concerns about the physical activity habits of the European population. Pervasive technologies and theories of
behavioral change are being combined in an effort to promote physical activity. The Activity Coach is an ex-
ample of one such system. Whereas the previous version of the Activity Coach set a fixed and permanent daily
goal, in this work we describe the addition of an automatically adaptive goal-setting feature to this existing
system. With the new feature, the daily goals for physical activity are set based on the user’s routine, contribut-
ing to the personalization of the system. A technical evaluation was performed to test the system’s adaptation
to the user’s routine. Additionally, a conversion factor between a unit of energy expenditure and number of
steps was determined. The evaluation indicates that our method of goal-setting provides more challenging
but still attainable goals when compared to the previous version. Additional evaluations are recommended to
evaluate the user’s perception and effects on physical activity behavior change of this new feature. The results
of this research are implemented in the existing Activity Coach and will be used in future patient evaluations.
1 INTRODUCTION
Due to the ageing population, the prevalence of
chronic disease is increasing worldwide. The growing
demand on healthcare services calls for cost-effective
treatments that reduce the demands on healthcare pro-
fessionals. From the socio-economical point of view,
the remaining labor force is responsible for cover-
ing the costs of a growing number of dependent el-
derly. This means that people have to work till a
later age and for longer periods of time, even when
not feeling in their healthiest condition. According
to the European Commission, nearly 25% of the Eu-
ropean working-age population suffers from a long-
standing problem which restricts their daily activi-
ties (Directorate General for Health and Consumers,
2011), chronic illnesses being the principal cause.
Provision of eHealth and Telemedicine services is
widely regarded as a promising paradigm to limit the
prevalence of chronic disease, reduce the burden on
the healthcare system and keep employees healthy
and at work. An important factor in reducing this bur-
den is the maintenance of a healthy lifestyle in terms
of regular physical activity. Regular physical activ-
ity is beneficial for everyone and the American Col-
lege of Sports Medicine recommends that the major-
ity of adults perform moderate-intensity cardio res-
piratory exercise training for at least thirty minutes
a day (Garber et al., 2011). However, of all Dutch
employees, 50% exercises too little and 44% is over-
weight (Hooftman et al., 2011). This not only poses a
risk for the inactive subject, but can also result in in-
creased sick leave and in a smaller active labor force
to finance healthcare.
Over the past years, a telemedicine intervention
to promote sustainable behavior change in terms
of physical activity was designed, implemented and
evaluated in several different studies (Van Weering
et al., 2009; Evering et al., 2011). Subjects were given
a 3D-accelerometer based sensor to assess daily ac-
tivity patterns, combined with a smartphone for pro-
viding continuous visual feedback in the form of a
graph. By comparing the subjects’ daily activity to
389
Cabrita M., op den Akker H., Achterkamp R., Hermens H. and Vollenbroek-Hutten M..
Automated Personalized Goal-setting in an Activity Coaching Application.
DOI: 10.5220/0004878703890396
In Proceedings of the 3rd International Conference on Sensor Networks (SENSORNETS-2014), pages 389-396
ISBN: 978-989-758-001-7
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

a pre-defined reference activity pattern, subjects were
automatically given motivational cues based on their
performance at regular intervals throughout the day.
The smartphone system, called the Activity Coach,
and the telemedicine platform which it is part of is
described in more detail in Section 2.3. Earlier stud-
ies using the Activity Coach have already shown the
effectiveness of providing real time motivational cues
on the users level of physical activity. However, more
recent studies have shown that compliance to the in-
tervention tends to drop after several weeks of use
(Tabak et al., 2013; Dekker-van Weering et al., 2012).
In order to increase long term compliance, we in-
tend to tailor the system better to its individual users.
Ongoing research focuses on tailoring the motiva-
tional messages that are sent to the users, in particular
their timing (op den Akker et al., 2010) and content
(Wieringa et al., 2011; Achterkamp et al., 2013). In
the presented research, we describe the addition of a
complex new feature to the Activity Coach, which al-
lows it to automatically generate personalized daily
goals for its users. Considering that users might have
particular activity habits during the different days of
the week, the new feature of the Activity Coach auto-
matically sets daily goals based on previous measure-
ments. In this way adaptation to the user’s routine and
subsequently more realistic goals are guaranteed.
The rest of the paper is outlined as follows. Sec-
tion 2 describes the background on the use of mobile
technologies in the promotion of physical activity, the
Goal Setting Theory and the Activity Coach — the
specific system under consideration here. Section 3
describes the design and implementation of the new
smart goal setting module. Section 4 deals with the
evaluation of the system. Conclusions, discussion and
an overview of future work are given in Section 5.
2 BACKGROUND
In this section, relevant background information is
given regarding (1) mobile technology for the pro-
motion of physical activity (Section 2.1), (2) the goal
setting theory that forms the theoretical basic of the
generation of automated goal lines (Section 2.2), and
(3) the technology platform in which the system has
been implemented (Section 2.3).
2.1 Mobile Technology in the Promotion
of Physical Activity
It is estimated that the penetration rate of mobile
phones in 2013 is around 96% worldwide (Union,
2013). The development of new technologies and the
spread of mobile technology in the general population
opens a whole range of new possibilities for promo-
tion of physical activity, combining real-time moni-
toring and coaching features. Around the world, sev-
eral research groups evaluate the efficiency and effi-
cacy of tailored interventions using pervasive technol-
ogy. Well-known examples of exercise tracking appli-
cations, e.g. Runkeeper
1
, Beeminder
2
, Endomondo
3
or Runtastic
4
, typically only use the smartphones
built-in global positioning system sensor for provid-
ing feedback in terms of e.g. speed and distance. Ap-
plications that encourage appropriate and sufficient
physical activity throughout the day are less widely
available, and in most cases use external sensors. The
advantage of using external sensors over sensors in
the smartphone is that the external sensor is usu-
ally worn on the body continuously, whereas smart-
phones are typically not. Additionally, modern ex-
ternal accelerometers are usually more accurate than
the smartphones built-in accelerometers. An exam-
ple of a system using an external sensor is given in
(Mutsuddi and Connelly, 2012) that combines the use
of pedometers and a smartphone. The authors sent
text messages to the subjects during a period of three
months. The messages encouraged physical activity
and were based on personalized step goals. Results
showed that the subjects increased both their daily
physical activity and their motivation regarding phys-
ical activity during the intervention. Other examples
are UbiFit Garden (Consolvo et al., 2009) and Fish
‘n‘ Steps (Lin et al., 2006).
2.2 Goal-setting Theory
The Goal-Setting Theory is among the most used the-
ories of individual behavior change in interventions
aiming at the promotion of healthy lifestyles. Firstly
focused on the work setting, Locke and Latham’s the-
ory emerges as the result of nearly forty years of em-
pirical research on the relationship between conscious
performance goals and task performance level (Locke
and Latham, 2002).
Setting goals implies the choice of the goal time-
frame (when should the goal be achieved?), the goal
source (who sets the goal?) and the goal complex-
ity, or difficulty (how hard will it be to achieve the
goal?). Regarding complexity, the Goal-Setting The-
ory defends that individuals are more likely to change
1
http://www.runkeeper.com/
2
http://www.beeminder.com/
3
http://www.endomondo.com/
4
http://www.runtastic.com/
SENSORNETS2014-InternationalConferenceonSensorNetworks
390

a behavior the higher the specificity and (achievable)
difficulty of a goal. At the same time, when setting a
goal, one should bear in mind personal characteristics
of the subject, such as goal importance, self-efficacy
and feedback.
The effectiveness of different goal-setting ap-
proaches has been researched extensively (Colineau
and Paris, 2010; Shilts et al., 2004). However, our
empirical experience with clinical trials suggests that,
within the therapeutic context, the currently available
systems tend to contain three specific flaws. First, the
majority of the monitoring and feedback systems use
a common goal to all the users disregarding the in-
dividual health status and physical condition. As a
consequence, a goal that is easily achievable for a
certain user can be unattainable for others. Second,
the goal is regularly maintained throughout time, not
following a possible, and desired, behavior change.
Third, the majority of the systems available do not
concern the spread of physical activity throughout the
day, setting one single daily goal. Finally, to our best
knowledge, there is no study that either implements or
evaluates the effectiveness of automatic tailored goal-
setting, i.e. goals set to meet individuals needs. Along
these lines, we propose a new feature that sets the
daily goal as well as a set of successive goals spread
over the day based on the users routine, while not ne-
glecting the therapeutic objective.
2.3 The Activity Coach
The Activity Coach is a Body Area Network con-
sisting of an activity sensor to be worn on the hip
and a smartphone application and is part of the
Telemedicine platform described in more detail in
(op den Akker et al., 2012). The sensor device con-
tains (among others) a 3D accelerometer sensor that
can capture, process and communicate wireless full
3D motion and orientation information (Figure 1).
The processed data is then sent to the smartphone
over Bluetooth. The output used by the system to es-
timate physical activity is the Integral of the Modulus
of body Acceleration (IMA), a unit that correlates to
energy expenditure (Bouten et al., 1996).
In the present work, the daily goal is defined as the
cumulative value of energy expenditure that the user
is recommended to achieve at the end of the day. In
the Activity Coach, this is seen as the final point of
the goal line (displayed on the screen as a green line).
The daily end point is the energy expenditure level
that the user has actually reached (final point of the
activity line, displayed on the screen as a blue line).
Figure 1: The Activity Coach, consisting of a smartphone
and accelerometer-based activity sensor.
Previous versions of the Activity Coach set the
daily goal either based on results from healthy control
subjects or to be 110% of the average of the daily end
points of the baseline period. The baseline period nor-
mally constitutes an initial seven days period during
which the user does not receive any kind of feedback.
In the older version the daily goal remained constant
throughout the whole intervention. Questions regard-
ing the efficiency of this way of goal-setting arose
during previous experiments. Our goal is to create
and evaluate a more efficient and effective procedure
by automatically generating personalized daily goals
for each user.
3 IMPLEMENTATION
The new version of the Activity Coach includes auto-
matically self-adaptive goal-setting features. By au-
tomatically self-adaptive goal-setting we mean that
the system sets goals for the upcoming days based on
both the user’s weekly routine and a set of parameters
defined by the healthcare professional via web-portal.
These parameters, explained in more detail in the fol-
lowing sections, are the ultimate goal, the deviation
allowance factor and the breakpoints. The high level
architecture of the system is explained in more detail
in (op den Akker et al., 2012). The self-adaptive pro-
cess is divided into two steps and is described in more
detail in the following sections.
3.1 Analysis of Physical Activity Daily
Routine
The daily data is analyzed in four parts: (1) average
of energy expenditure per minute during different day
AutomatedPersonalizedGoal-settinginanActivityCoachingApplication
391

parts (morning, afternoon, evening, and full day), (2)
deviation between the user’s physical activity and the
goal line for that day, (3) ratio between daily end point
and daily goal, and (4) a summary of the minute-by-
minute IMA values (smoothed over e.g. 15 minute
intervals) — referred to as saved IMA data. The val-
ues from the daily analysis are subsequently com-
bined with the equivalent values from previous ana-
lysis occurred on the same day of the week. There-
fore, the system keeps track of the parameters of the
four sets of data aforementioned in a specific file for
each weekday.
From the daily analysis the parameters used for set-
ting the goal line are the daily end point and the saved
IMA data. These values are combined with data pre-
viously analyzed using the Linear Moving Weighted
Average (LMWA) — Equation 1. For example, if the
system is analyzing the data obtained on a Monday,
the daily end point of this day is averaged with the
daily end points of all the previous Mondays using the
LMWA. Afterwards the resulting value will be used
for setting the goal line for the next Monday. This
method was chosen instead of an arithmetical average
to take into account the evolution of the user. In this
way the more recent a measurement, the bigger its
weight in the calculation of the average. From these
steps results the averaged end point and the averaged
saved IMA data.
LW MA(point, N)
i
=
N
∑
j=1
point
i−N+ j
× (i −N + j)
N
∑
j=1
j
(1)
3.2 Determining the Goal Line for the
Upcoming Day
By goal line we mean both the quantity and distribu-
tion of physical activity that is recommended to the
user over the day. It has two main parameters: daily
end goal and daily pattern, i.e. distribution of phys-
ical activity over the day. In the new version of the
Activity Coach the healthcare professional sets an ul-
timate goal for the different days of the week. This
is seen as an upper limit for the daily end goal and
should be adjusted for each user. This ultimate goal
puts a maximum on the value of the daily goal set by
the system in order to avoid unattainable goals. An-
other value set by the healthcare professional is the
deviation allowance factor. This factor determines
the growth rate of the daily goal when compared to
the averaged end point. By default this value is set to
110%.
3.2.1 Determine End Goal
After the daily analysis, the averaged end point is
multiplied by the deviation allowance factor and the
result compared with the ultimate goal. If the result is
higher than the ultimate goal, the new daily goal has
the same value as the ultimate goal. If the result is
lower than the ultimate goal, the new daily goal is set
as the averaged end point multiplied by the deviation
allowance factor.
3.2.2 Determine Goal Line Pattern
The healthcare professional also sets the distribution
of physical activity that the user should follow over
the day. This happens by setting breakpoints —
<time,percentage>-pair points. As an example,
one can say that the user should achieve 40% of his
daily activity at 12 oclock. There is no limit to the
amount of breakpoints that can be set, allowing for
a fine or coarse granularity of the goal line pattern.
When setting a new goal line, each one of these break-
points is compared to the percentage that the user ac-
complished at the same time of the day. This value is
determined by calculating the ratio between the cor-
respondent values of the averaged saved IMA data,
i.e. the one at the same (or closer) time of the day,
and the averaged end point. If this ratio is lower than
the percentage set on the breakpoint, the percentage
set in the goal line will be the average of the two val-
ues. Following the example given previously, if the
user should accomplish 40% of his daily activity at 12
o’clock and he accomplished only 20%, in the next
goal line for this day of the week, at 12 o’clock the
user is supposed to achieve 30% of his daily goal.
3.2.3 Runtime Procedure
When the application is launched the system checks
if there is data from previous days to analyze. If that
is the case, the system analyzes the data of each day
separately and verifies if there are days with no valid
data (e.g. days when the user did not use the system,
or did not wear it for a long enough period of time).
In that case, the goal line is created based either on
stored data from that day of the week or in the param-
eters set by the healthcare professional. In this way it
is guaranteed that there is a goal line for every day. If
the data of a day is valid, i.e. if there is a significant
amount of data points, the system analyzes the data
and checks if there is data stored about that day of the
week. If so, it combines the new and the old data and
SENSORNETS2014-InternationalConferenceonSensorNetworks
392

sets a new goal line after comparison with the param-
eters set by the healthcare professional. If not, it uses
only the data of the day to create a new goal line.
4 SIMULATIONS AND
EVALUATION
The presented paper reports exclusively the technical
evaluation of the new feature of the Activity Coach
and not the effectiveness of the application in terms
of behavior change. Ongoing research is being done
on the behavior change component and results are ex-
pected during the upcoming years. Additionally, our
only concern at this phase of the research regarded
the daily end goals set to the user and not the ones re-
ferred to in this paper as breakpoints. Although there
are clear guidelines on the amount of physical activ-
ity that should be performed per day/week, there is no
evidence on the way this activity should be distributed
over the day. Literature suggests that prolonged inac-
tivity is unhealthy independently of physical activity
level, meaning that single boosts of activity are not
the enough to meet the benefits of an healthy lifestyle
(e.g. (van der Ploeg et al., 2012)). This supports the
general notion that physical activity should be equally
spread over the day. However, there is no clear evi-
dence on the exact health benefits.
The Goal-Setting Theory emphasizes the impor-
tance of setting challenging but attainable goals. To
test the self-adaptive character of the system we an-
alyzed data from subjects with Chronic Obstructive
Pulmonary Disease acquired in a longitudinal study
that was executed between May and November of
2012, for the European Project IS-Active. From a
sample of 10 subjects, only the data of 7 patients was
used. Three subjects were excluded as a consequence
of the limited amount of viable data available. From
the 7 remaining subjects, two were female, four were
not working at the time of the study and all of the sub-
jects had low levels of physical activity as assessed
with the Baecke questionnaire (Baecke et al., 1982).
The experiment design followed the one described in
section 2.3. For each subject, the daily goal remained
the same throughout the intervention and was defined
as 110% of the average daily end points of the base-
line period. From now the daily goals set based on
the previous version of the Activity Coach will be re-
ferred to as fixed goals.
4.1 Fixed Versus Self-adaptive
Goal-setting
Our aim with this simulation was to compare the chal-
lenge and attainability of the provided goals set by
the previous (fixed goals) and newer versions (adap-
tive goals) — of the Activity Coach. To clarify, the
fixed goals correspond to what was, in reality, dis-
played on the screen of the smartphone during the
IS-Active experiment and the adaptive goals are hy-
pothetical goals that would have displayed in case of
using the automatically self-adaptive goal-setting fea-
ture. We intend to evaluate if the system would in
fact adapt to user’s routine as expected during the de-
sign phase. The goals were considered challenging
and attainable if the ratio between the averaged of the
goals and the averaged activity performed would be
between 0.75 and 0.95. The exact values are to be
taken as indicative. The procedure followed in this
study was as follows:
1. Calculate the average IMA count per minute for
each one of the days of the baseline period. All
the days with less than 300 data points were ex-
cluded (frequency of acquisition is 1 data-point
per minute);
2. Save the goal set by the system during the experi-
ment (fixed goal);
3. Set an ultimate goal as 200% of the average of the
end points of the baseline period. This value was
chosen because it seems challenging but not im-
possible to double your level of physical activity;
4. Set automatically adaptive daily goals based on
the algorithm described in Section 3;
5. Compare the daily IMA averages during the inter-
vention period and the average of the fixed (step
2) and adaptive goals (step 3 and 4).
Table 1 shows the results from both methods. It is
clear that the adaptive goals tend to be more challeng-
ing than the fixed goals. Especially in the case of the
first three subjects, the former method of goal-setting
provides daily goals that are, on average, lower than
the activity during the intervention period. Clearly,
this is not a desired system behavior considering that
the subject would not feel challenged to increase
physical activity levels.
To better evaluate the self-adaptive feature, both
old and new version were analyzed graphically. Fig-
ures 2 and 3 show the results of the simulations us-
ing data from subjects isa09 and isa10, respectively.
The black line shows the subjects daily activity (Daily
data), the dashed line represents the fixed goal (Fixed)
and the light grey line the adaptive goal (Adaptive).
AutomatedPersonalizedGoal-settinginanActivityCoachingApplication
393
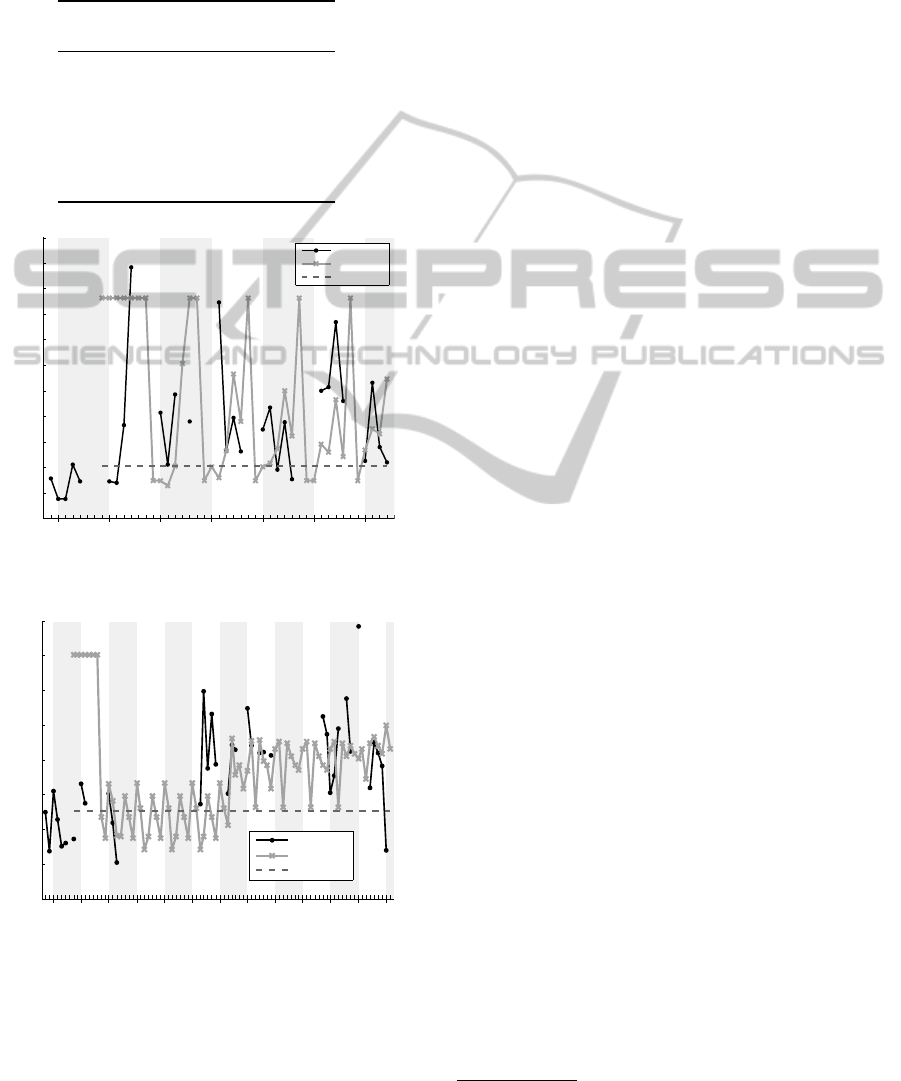
Table 1: Results of the evaluation performed with data from
subjects of the IS-Active project. Only days with more than
300 measured activity values were considered (Days). The
average of IMA counts per minute during the intervention
period was divided by the average per minute provided us-
ing the basic goal setting (Fixed) and the adaptive version
(Adaptive).
Goal Ratios
Subject Days Fixed Adaptive
isa07 40 1.05 0.83
isa09 30 1.24 0.98
isa10 38 1.26 1.01
isa11 61 0.94 0.90
isa12 53 0.99 0.93
isa13 59 0.90 0.90
isa14 36 0.92 0.74
600
700
800
900
1000
1100
1200
1300
1400
1500
1600
1700
Daily data
Adaptive
Fixed
Mon Mon Mon Mon Mon Mon Mon
Activity Average (IMA/min)
Time (day)
Figure 2: Simulation results comparing adaptive goals with
fixed goals for subject isa09.
300
400
500
600
700
800
900
1000
1100
Daily data
Adaptive
Fixed
Mon Mon Mon Mon Mon Mon Mon Mon Mon Mon Mon Mon
Time (day)
Activity Average (IMA/min)
Figure 3: Simulation results comparing adaptive goals with
fixed goals for subject isa10.
In both cases, confirming the results shown in Table
1, the goal set by the previous version of the Activity
Coach is not challenging for the respective users. This
can lead to demotivation. For the adaptive goals, it is
clear that the system adapts to the users routine. This
is especially visible in the seventh week. (Figure 3).
The system not only sets specific goals to each day of
the week but also adapts these goals over time.
4.2 Other Simulations
As part of the research we performed a study to (1)
evaluate the reasonability of the default deviation al-
lowance factor, and (2) be able to provide more con-
crete, understandable and specific feedback to the
users. When providing feedback, it is important to
assure that the user fully understands the message re-
ceived. However, we are aware that, contrarily to
other commonly known measures of physical activ-
ity (e.g. calories expenditure, distance and number of
steps performed), IMA is not an understandable unit.
In our evaluation we decided to analyze the correla-
tion between IMA counts throughout the day and the
number of steps performed.
A single-study subject was performed in order to
determine a conversion factor between IMA counts
and number of steps. In this small study we used a
FitBit Zip
5
to measure steps taken during 11 days of
free living. Over the experiment period, the value of
IMA counts were compared to the number of steps
performed during each 5-minute interval. The rela-
tion between the two units found after data process-
ing is presented in Equation 2 (p<0.0001). The num-
ber of steps was then converted to average of minutes
walking according to recommendation from Ameri-
can Journal of Preventive Medicine — 100 steps cor-
respond to a minute walking. We considered that the
factor would be reasonable (i.e. challenging and at-
tainable) if it would add less than 20 minutes walking
to the user. For this evaluation, we used once again the
data acquired during the IS-Active project. For each
subject, we calculated the total IMA added in average
to the daily physical activity and converted to number
of steps and respective number of minutes walking.
Table 2 shows the results of this evaluation.
IMA
count
(steps
count
) = 30.24 × steps
count
+ 1680
(2)
When setting a new daily end goal, the average of
the daily end points of that weekday is multiplied by
the deviation allowance factor. Based on this first ex-
plorative study we suggest that 110% is a reasonable
factor for increasing the daily physical activity of the
user. However, more studies should be performed in
5
http://www.fitbit.com/uk/zip/specs
SENSORNETS2014-InternationalConferenceonSensorNetworks
394

Table 2: Total IMA (IMA), number of steps (Steps) and
minutes of walking (Minutes) added in average to the daily
physical activity using the self-adaptive goal-setting feature.
Only days with more than 300 measured activity values
were considered (Days).
10% Additional Effort
Subject Days IMA Steps Minutes
isa07 40 29,823 931 9
isa09 30 62,493 2,011 20
isa10 38 43,517 1,383 14
isa11 61 55,072 1,766 18
isa12 53 64,485 2,077 21
isa13 59 55,419 1,777 18
isa14 36 42,023 1,334 13
order to address the variance related to the method of
measuring acceleration during different types of ac-
tivities and expressing this as a number of steps per
minute.
5 CONCLUSIONS
In this work we implemented self-adaptive goals in
order to encourage daily physical activity, bearing in
mind the importance of both the final goal of energy
expenditure and the distribution of activity over the
day. The level of challenge and the attainability of the
goals provided to the user was evaluated with (1) data
acquired during previous studies, and (2) newly gath-
ered data from a single-subject study. From simula-
tions using data of a 3-months-study we conclude that
self-adaptive goals tend to be more challenging than
fixed goals (both methods provide attainable goals).
The main limitation concerns the conversion from
IMA counts to steps and consequent evaluation of the
additional effort required from the user when setting a
new goal. Along these lines we suggest two different
studies. First a study should be performed including a
larger sample of subjects in order to increase the accu-
racy of the conversion factor between IMA counts and
steps. Second, within the same subject, various mea-
suring contexts should be taken into account in order
to get a personalized conversion between number of
steps and minutes walking. Additionally, the simple
study showed in section 4.2 suggests that future im-
plementations should consider also a threshold to the
additional effort required from the user. As a sugges-
tion, the additional threshold can correspond to 10%
unless the case when this value adds more than 20
minutes walking to the daily activity.
Regarding the activity pattern, at the moment of
publication, there is no guideline that defines what
a proper daily pattern of physical activity is. If fu-
ture research gives insights into the most suitable dis-
tribution of physical activity throughout the day, the
breakpoints of the goal line can be adjusted through
a web-portal in order to be coherent with the new re-
sults.
To conclude, we believe that the incorporation of
self-adaptive goal-setting in the Activity Coach will
benefit users in their way to become more active.
Also, healthcare professionals will benefit by allow-
ing them to give more accurate recommendations to
their patients as they are more aware of their physi-
cal activity routines. The results from this research
will be used in future experiments using the Activity
Coach and can be adapted to other ambulatory feed-
back systems regarding promotion of physical activ-
ity.
ACKNOWLEDGEMENTS
This publication was supported by the Dutch national
program COMMIT (project P7 SWELL).
REFERENCES
Achterkamp, R., Cabrita, M., and op den Akker, H. (2013).
Promoting a Healthy Lifestyle: Towards an Improved
Personalized Feedback Approach. In IEEE 15th Inter-
national Conference on e-Health Networking, Appli-
cations and Services (Healthcom 2013), pages 677–
679.
Baecke, J. a., Burema, J., and Frijters, J. E. (1982). A short
questionnaire for the measurement of habitual physi-
cal activity in epidemiological studies. The American
journal of clinical nutrition, 36(5):936–42.
Bouten, C. V., Verboeket-van de Venne, W. P., Westert-
erp, K. R., Verduin, M., and Janssen, J. D. (1996).
Daily physical activity assessment: comparison be-
tween movement registration and doubly labeled wa-
ter. Journal of applied physiology (Bethesda, Md. :
1985), 81(2):1019–26.
Colineau, N. and Paris, C. (2010). Motivating reflection
about health within the family: the use of goal set-
ting and tailored feedback. User Modeling and User-
Adapted Interaction, 21(4-5):341–376.
Consolvo, S., Klasnja, P., McDonald, D. W., and Lan-
day, J. a. (2009). Goal-setting considerations for per-
suasive technologies that encourage physical activity.
Proceedings of the 4th International Conference on
Persuasive Technology - Persuasive ’09, page 1.
AutomatedPersonalizedGoal-settinginanActivityCoachingApplication
395

Dekker-van Weering, M. G. H., Vollenbroek-Hutten, M.
M. R., and Hermens, H. J. (2012). Do personalized
feedback messages about activity patterns stimulate
patients with chronic low back pain to change their
activity behavior on a short term notice? Applied psy-
chophysiology and biofeedback, 37(2):81–9.
Directorate General for Health and Consumers (2011). Eu
health programme, 2011. health of people of working
age. Technical report, European Union.
Evering, R. M., T
¨
onis, T. M., and Vollenbroek-Hutten,
M. M. (2011). Deviations in daily physical activity
patterns in patients with the chronic fatigue syndrome:
a case control study. Journal of psychosomatic re-
search, 71(3):129–135.
Garber, C. E., Blissmer, B., Deschenes, M. R., Franklin,
B. A., Lamonte, M. J., Lee, I.-M., Nieman, D. C.,
and Swain, D. P. (2011). American College of Sports
Medicine position stand. Quantity and quality of ex-
ercise for developing and maintaining cardiorespira-
tory, musculoskeletal, and neuromotor fitness in ap-
parently healthy adults: guidance for prescribing ex-
ercise. Medicine & Science in Sports & Exercise,
43(7):1334–1359.
Hooftman, W., Hesselink, J., van Genabeek, J., Wiezer,
N., and Willems, D. (2011). TNO Arbobalans 2010:
Kwaliteit van de arbeid, effecten en maatregelen in
Nederland. Technical report, TNO.
Lin, J., Mamykina, L., Lindtner, S., Delajoux, G., and
Strub, H. (2006). FishnSteps: Encouraging Physical
Activity with an Interactive Computer Game. In Dour-
ish, P. and Friday, A., editors, UbiComp 2006 Ubiq-
uitous Computing, volume 4206 of Lecture Notes in
Computer Science, pages 261–278. Springer.
Locke, E. A. and Latham, G. P. (2002). Building a prac-
tically useful theory of goal setting and task moti-
vation: A 35-year odyssey. American Psychologist,
57(9):705–717.
Mutsuddi, A. U. and Connelly, K. (2012). Text Messages
for Encouraging Physical Activity. In 6th Interna-
tional Conference on Pervasive Computing Technolo-
gies for Healthcare, pages 33–40.
op den Akker, H., Jones, V. M., and Hermens, H. J. (2010).
Predicting Feedback Compliance in a Teletreatment
Application. In Proceedings of ISABEL 2010: the
3rd International Symposium on Applied Sciences in
Biomedical and Communication Technologies, Rome,
Italy.
op den Akker, H., Tabak, M., Marin-Perianu, M., Huis In’t
Veld, R. M., Jones, V. M., Hofs, D., Tonis, T. M.,
van Schooten, B. W., Vollenbroek-Hutten, M. M., and
Hermens, H. J. (2012). Development and Evalua-
tion of a Sensor-Based System for Remote Monitor-
ing and Treatment of Chronic Diseases - The Continu-
ous Care & Coaching Platform. In Proceedings of the
Sixth International Symposium on e-Health Services
and Technologies (EHST 2012), pages 19–27, Geneva,
Switzerland.
Shilts, M. K., Horowitz, M., and Townsend, M. S. (2004).
Goal setting as a strategy for dietary and physi-
cal activity behavior change: a review of the litera-
ture. American journal of health promotion : AJHP,
19(2):81–93.
Tabak, M., op den Akker, H., and Hermens, H. (2013).
Motivational cues as real-time feedback for changing
daily activity behavior of patients with COPD. Patient
Education and Counceling.
Union, I. T. (2013). The world in 2013: Ict facts and figures.
online.
van der Ploeg, H. P., Chey, T., Korda, R. J., Banks, E., and
Bauman, A. (2012). Sitting time and all-cause mor-
tality risk in 222 497 Australian adults. Archives of
internal medicine, 172(6):494–500.
Van Weering, M. G., Vollenbroek-Hutten, M. M., T
¨
onis,
T. M., and Hermens, H. J. (2009). Daily physical ac-
tivities in chronic lower back pain patients assessed
with accelerometry. European journal of pain London
England, 13(6):649–654.
Wieringa, W., op den Akker, H., Jones, V. M., op den Akker,
R., and Hermens, H. J. (2011). Ontology-Based Gen-
eration of Dynamic Feedback on Physical Activity. In
Proceedings of the 13th Conference on Artificial In-
telligence in Medicine (AIME), pages 55–59, Bled,
Slovenia. Springer.
SENSORNETS2014-InternationalConferenceonSensorNetworks
396
