
Mobile Application Design for Health Intermediaries
Considerations for Information Access and Use
Izak van Zyl and Retha de la Harpe
Department of Research and Development, Faculty of Informatics and Design,
Cape Peninsula University of Technology, 80 Roeland Street, Cape Town, South Africa
Keywords: Health Information Needs, Health Intermediaries, Mobile Application Design, Context.
Abstract: Health intermediaries in emerging contexts exhibit a diversity of information needs in conducting their
professional duties. There is limited understanding, however, as to the complex needs of these groups.
Furthermore, there is still a paucity of research on supporting the information needs of intermediaries via
technological means. This paper employs a qualitative meta-analysis in unpacking the dynamism of
intermediary practice in South Africa. The authors consider mobile application design in accessing and
using health information. A number of critical design considerations are presented, including the role of
context as a static and dynamic modality. The authors ultimately derive an information model, which
assimilates four intersecting dimensions of context.
1 INTRODUCTION
There is still a paucity of research on supporting
information needs in marginalised health contexts
via technological means. This especially concerns
aspects of health promotion, disease prevention, and
intrapartum care. Within global and national
discourses on hyperconnectivity (Bilbao-Osorio et
al., 2013), underpinning the role of information
access and literacy, technology-supported
information systems become crucial considerations
(Neter and Brainin, 2012). Additionally, in the
context of rapid access and the ubiquity of portable
devices, ‘mobility’ becomes a significant component
to said information systems. We focus our efforts,
therefore, on considerations for mobile application
design.
This study discusses the information needs of
three groups of health practitioners: midwives,
home-based caregivers, and health promoters. We
consider the multifarious ‘personas’ of these
individuals in mediating health information to
beneficiaries (patients, families, and community
members). In this regard, we interpret the role of
practitioners largely as intermediaries, acting as
conduits of health information in marginalised
contexts.
The primary objective of this paper, ultimately,
is to present a qualitative meta-analysis of three case
studies that have considered the respective groups.
We locate the ‘health information needs’ of each
group, and identify those personal and contextual
dynamics that shape the design of systems that
support health information access. All three case
studies employed human-centred design in ideating
a series of mobile application possibilities to support
health intermediaries.
The research question that guides our analysis is:
“What are the design considerations of mobile
applications that facilitate the dissemination,
exchange and reporting of relevant health
information?” The proposed output of this
endeavour is a conceptual model for health
information that encompasses ‘situated’ design
thinking.
2 STATUS OF THE LITERATURE
2.1 Considerations for Information
Access and Use
In peripheral settings, marked by the inadequacy or
inaccessibility of health information, intermediaries
become the primary source of health-related
knowledge. Intermediaries translate and adapt
health-related information for local use, thus acting
as conduits or dependable information sources
323
van Zyl I. and de la Harpe R..
Mobile Application Design for Health Intermediaries - Considerations for Information Access and Use.
DOI: 10.5220/0004800803230328
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2014), pages 323-328
ISBN: 978-989-758-010-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

(Chetley, 2006).
Intermediaries generally exhibit a variety of
information needs. These are based on a continuum
of requirements and desires, which can vary from
unexpressed, conscious, formal, and compromised
needs. Information needs will vary in nature,
complexity, and content, and are mediated or
manifest through information practices. These
describe the ways in which intermediaries
collectively share, withhold and manage information
as they interpret it according to their professional
functionings (Dourish and Anderson, 2006).
In community-based contexts, intermediaries
typically convey information on an informal basis,
via face-to-face meetings, focus groups, or
discussions. This could however result in
information degradation over time, or prove
inadequate for sharing and public dissemination.
Moreover, in the context of increasingly ubiquitous
mobile technology in the Global South, community-
oriented information systems become critical in
addressing the shortcomings of transitory
information sharing. This is especially the case in
granting universal access, and in ensuring free and
flexible use, in line with locally defined practices
(Bilbao-Osorio et al., 2013). In this vein, there is a
growing need to develop community-based systems
that cater to the collaborative information behaviour
of health intermediaries (see Ruxwana et al., 2010).
Ostensibly, technical and infrastructural
considerations remain key in designing health
information systems. In marginalised community
settings, especially in rurally isolate areas, ‘context’
becomes a foremost and critical design
consideration. That is, intermediaries are entrenched
in deep spatial, temporal and cultural modalities.
These define and redefine both information practices
and collaborative information behaviour (Räsänen
and Nyce, 2008).
An understanding of context as a nuanced and
multifarious system helps to stipulate the embedded
requirements of health interventions or services
(Bradley and Dunlop, 2005). Context can here be
described as a frame, an environment or a
background that surrounds the phenomena under
study. But human activities involve practices and
relations that are meaningful for a particular
situation or setting that need to be studied and
understood (Dourish, 2004). Through eliciting users’
(intermediary) contexts, designers may recognise
multiple circumstantial representations, including
location, identity, environment and time. In this
regard, context can be seen as an interactional
problem that represents the relational property
between objects or activities (Dourish, 2004). This
view of context is both dynamic and situational,
recognising that intermediaries socially construct
their practices by attaching meaning to what they are
doing. Practice, in this sense, is both the physical
activity and its meaningful experience – thus uniting
action and meaning (ibid.).
Ultimately, the surveyed literature reveals
agreement that context of use becomes a critical
consideration in providing health information, and in
developing technology-supported information
services.
2.2 MHealth
With more than 6 billion connections worldwide and
US$1.3 trillion in annual revenue, mobile telephony
has become the largest and most prevalent
information and communication technology in
history, at least economically (Bold and Davidson,
2012). And whilst the global scale of mobile
telephony and its economic impacts are
predominantly well documented (and understood),
its “ultra-personal” and omnipresent social
networking ability is expected to have a far greater
impact (ibid.). In addition, mobile broadband has
become the primary method of internet access for
people around the world. In emerging regions, this
indicates that mobile is the first, or even the only,
way that individuals or communities can gain
internet access (ibid.).
Mobile telephony accords with the need for
healthcare systems that are readily accessible and
usable (Katz and Rice, 2008). mHealth enables the
connecting of individuals to information and
services that would otherwise be unfeasible,
especially in emerging regions. Additionally,
mHealth can support the shift from treating acute
and chronic diseases to prevention and health
promotion (Leon and Schneider, 2012).
Drivers for mHealth applications are socio-
economic rather than technical (Norris et al., 2009).
A single-solution focus on mHealth should be
replaced with it being an extension and integrator of
underlying health information systems that support
the point-of-care for health workers (Mechael &
Searle, 2010). In this case, the interoperability of
mHealth applications is a growing concern, so to
link health workers with relevant information when
and where it is needed (ibid.).
HEALTHINF2014-InternationalConferenceonHealthInformatics
324

3 METHODOLOGY
In this paper, we document part of a qualitative
meta-analysis of three case studies. Each study
centres on the role of health practitioners in
mediating information to patients or beneficiaries.
The meta-analysis is conducted at an ‘etic’ level, and
considers an assemblage of contextual and personal
experiences as exhibited by health practitioners.
Each of the three case studies has employed human-
centred design (HCD) in ideating the challenges and
opportunities in accessing health information. The
ontological basis for human-centred design here is
self-evident: the users of artefacts, technologies, or
services are located at the heart of the design
process.
Within each study, HCD manifested across a
participatory methodology in two phases: discovery
and creation. The discovery phase – also termed the
exploration and insight stage – aimed to elucidate
the many social, cultural, and environmental
dynamics that characterise the micro health
landscape. The creation phase – also termed the
design stage – assimilated the exploratory outcomes
within tangible design considerations. Both phases
are initial processes, and build towards the latter
stages in participatory design: testing, reflection,
implementation, and iteration. These latter stages
will be discussed in follow-up research.
Each case gathered empirical data using a series
of techniques associated with participatory design:
context and stakeholder mapping, semi-structured
interviews, focus groups, user need analysis, co-
design sessions, service concepting, prototyping and
iteration. These data sets were collated and
assimilated according to the research question that
guides this study. Overall, this process corresponds
to the pursuit of a qualitative meta-analysis, and is
guided by its fundamental principles.
4 RESULTS AND DISCUSSION
4.1 Intermediary Personas
This meta-study considers three personas of
intermediaries derived from the South African health
landscape. Personas are user archetypes that help
define the intended design intervention by replacing
the notion of the abstract, elastic user. The persona is
a precise description of a hypothetical (end) user and
his or her goals, and it represents a group of users
throughout the entire design process (Kujala and
Kauppinen, 2004). The three personas of health
intermediaries that we identified include the
midwife, the caregiver, and the health promoter.
Each is briefly described below. It is acknowledged
that these do not and cannot articulate the full scope
of individual users’ identities, histories, experiences,
values and behaviours. Rather, personas here
function as a point of reference for deriving a
common understanding of user needs, contexts, and
preferences.
4.1.1 Midwife Intermediary
A specific midwife persona is identified as the
following: Agnes is a qualified midwife appointed
by the Department of Health to provide services in a
local Midwife Obstetric Unit (MOU), based in a
resource-restricted community in South Africa.
Agnes, in her thirties, is also from the area and
travels by public transport to the MOU daily. Being
the only maternal unit in the area, Agnes is
overburdened and has limited time for each new
patient. Long patient queues encircle the unit, adding
pressure on the clinical staff. Pregnant mothers are
seen here for the first time, and for follow-up visits.
Problem and critical cases are referred to local
hospitals. Due to the highly stressful environment,
Agnes feels overwhelmed about her patient load,
and makes numerous referrals to specialised care.
This is especially the case when she is uncertain
about the severity of her patients’ conditions. Some
of her patients arrive from outside of the province,
and she does not have access to suitable information
on their personal health history. Having this access
is especially important in the case of communicable
and chronic illness. This need typically occurs
during emergencies when additional information
about the patient is not available. Patients are
generally unable to supply the required information
due to being semi- or illiterate, or uninformed about
their health conditions.
4.1.2 Caregiver Intermediary
A specific caregiver persona is identified as the
following: Priscilla is a home-based health worker in
a peri-urban community, and resides in the vicinity.
Priscilla is thirty-four years old and has received
basic training as a home-care nurse from her local
hospice. She visits patients on foot, and is
sometimes afraid to enter dangerous areas. She owns
a feature phone on a prepaid airtime basis. Although
the hospice provides her with weekly airtime, this is
minimal, and often insufficient in fulfilling her
duties. She enjoys her work, but find it physically
demanding and emotionally draining. Recently, she
MobileApplicationDesignforHealthIntermediaries-ConsiderationsforInformationAccessandUse
325

needed to attend to an influx of migrant labourers
from the Eastern Cape and other provinces. She
finds it challenging to converse with these patients
due to not speaking their home language. Given their
cultural heritage and personal beliefs, she is not
always knowledgeable in taking care of them.
Priscilla wishes that she had access to relevant
information in helping her better respond to her
patients’ needs. She is unable to remember
everything she learnt during her training at the
hospice. She often uses her mobile phone to contact
the care coordinator, using the “please-call-me”
option. This is a free service, and alerts the
coordinator to phone her.
4.1.3 Health Promoter Intermediary
A specific health promoter persona is identified as
the following: David is a young man, residing in in a
peri-urban community. He has recently completed
his Matric (Grade 12) and decided to work as a
health promoter in the area. He is contracted by a
local non-profit organisation, which works in
partnership with the Department of Health and the
provincial government. David receives a stipend for
his services, which includes basic transport and
meals. He is responsible for distributing promotional
health materials (informational pamphlets and
contraceptives) in High Transmission Areas like taxi
ranks, public restrooms, and shopping centres. David
spends up to 9 hours a day in these areas, and
engages in regular conversation with community
members. They are interested in discussions about
reproductive health, but challenge David on his
knowledge about topics like unprotected sex,
medical male circumcision, and condom use. Some
members feel that these are culturally contested
issues, and engage in heated debates with David.
David does not have modern promotional materials
available, and uses paper-based guidelines, written
in two or three languages, to support his discussions.
He wishes that these were more interactive and
colourful, to enable him to better communicate
about important issues. He also wishes that his
supply of contraceptives were more conducive to
local needs (stronger materials, better smell, more
colourful).
4.2 Design Considerations
In the following sections, we identify specific
considerations that have emerged in our qualitative
meta-analysis. These are grouped along the
modalities of context and information needs: two
leading dimensions in the design of mobile services
for health intermediaries.
4.2.1 Context
Our meta-analysis identifies ‘context’ as a
significant dimension to the provision of information
access and use in supporting the work practices of
intermediaries. We observe four dimensions of
context within which intermediaries are located:
personal, physical, macro, and interactional. The
personal (micro) context contains those social,
biological and behavioural phenomena that
constitute the subjective realm of the intermediary.
General examples of micro contexts may be derived
from our respective personas: all three
intermediaries work in the communities they live,
received basic health training, and converse mostly
in the same language than the people they service.
Additionally, intermediaries have a positive attitude,
with a real desire to assist. All three intermediaries
possess a mobile phone, but with limited money to
make calls or to send messages. It is expected that
these yet ‘static’ elements of personal context may
shape ‘dynamic’ information needs and practices.
For example, intermediaries possess mobile phones
– this is a static modality. They may use these
phones to access the internet to retrieve nursing
guidelines. This dynamic interaction constitutes
information behaviour.
We observe in the physical (meso) context
dimensions of material, temporal, infrastructural,
and environmental significance. As with the micro
context, we may derive general examples of physical
meso contexts: internet connectivity is problematic
and the available physical and infrastructural
resources are limited. It is expected that these static
elements of meso context will shape eventual
information practices and behaviour.
The former contexts ascribe to a broader (macro)
context that constitutes socio-economic, political,
and geographic modalities across South Africa, the
Global South, and the world. We may here derive
very general macro elements: poverty and socio-
economic status; the inability of the national
government in providing essential healthcare; the
proliferation of HIV/AIDS and tuberculosis, among
other chronic conditions and communicable illness;
crime and violence; inter alia. These phenomena are
generally embedded within an emerging landscape,
characterised by resource limitations, a lack of
locally relevant content (health information),
insufficient resources for adapting information, a
lack of clarity around key stakeholders and available
services, inhibiting cultural factors that prevent
effective use of ICT, and lack of capital in
HEALTHINF2014-InternationalConferenceonHealthInformatics
326
developing and sustaining ICT solutions (Chetley,
2006).
The interactional context, lastly, encapsulates
information practices, which are fluid and adaptable.
We consider in this context an interactional space
between different information components. Within
this space, we observe a diversity of interfaces,
practices, and experiences, as exhibited by both
intermediaries and users. The interactional context
also sees the emergence of an information space: a
temporary structure that arises when intermediaries
interact with information objects, beneficiaries, and
colleagues. The space is both a container of
interactions, and a setting within which
intermediaries act (Williams et al., 2005).
We propose that this information space be
facilitated by mobile technologies. A number of
considerations remain in the design of mobile
interfaces. These should consider the preferences
and experiences of intermediaries, and as exhibited
through information practices and needs. These are
briefly discussed below.
4.2.2 Information Needs
Our meta-analysis suggests a diversity of
information needs as expressed by health
intermediaries. For purposes of summation, these are
tabulated below. Each need corresponds to the four
dimensions of context earlier identified.
Table 1: Information needs of intermediaries.
Context Information need
Personal (micro)
Locally defined information
about treatment, prevention, and
promotion.
Physical (meso)
Information that supports the
services provided, including
health facilities, resources,
services, partners, and training
opportunities in the region.
Socio-economic
(macro)
Information about guidelines,
policies, international best
practices, and laws.
Interactional
(dynamic)
Information practices;
information seeking and
behaviour of individuals and
groups; experiences when
interacting with information
objects and with mobile devices,
systems or applications.
4.2.3 MHealth Intermediary Information
Model
Emerging contexts, especially when characterised by
socio-economic and environmental constraints,
indicate critical dimensions worth considering. A list
of the foremost implications of these dimensions is
presented, as derived from our meta-analysis:
1. Health intermediaries need information to
support their work practices;
2. Currently, the vast amount of health information
is not always accessible and locally relevant;
3. An intervention may be needed to facilitate the
access and use of relevant health information
for intermediaries. mHealth has the potential to
facilitate this;
4. Intermediaries’ work practices are influenced by
the contexts in which they function;
5. Contextual aspects are complex and need to be
unpacked to provide for possible information
interventions;
6. Contexts manifest as both static and dynamic
modalities. Example, availability of a phone
(static) against using the phone to seek and use
information (dynamic).
7. In designing mobile interventions, both static
and dynamic context considerations are
required.
These considerations in mind, we build towards
an mHealth information model that supports
intermediary work practice across contextual
modalities.
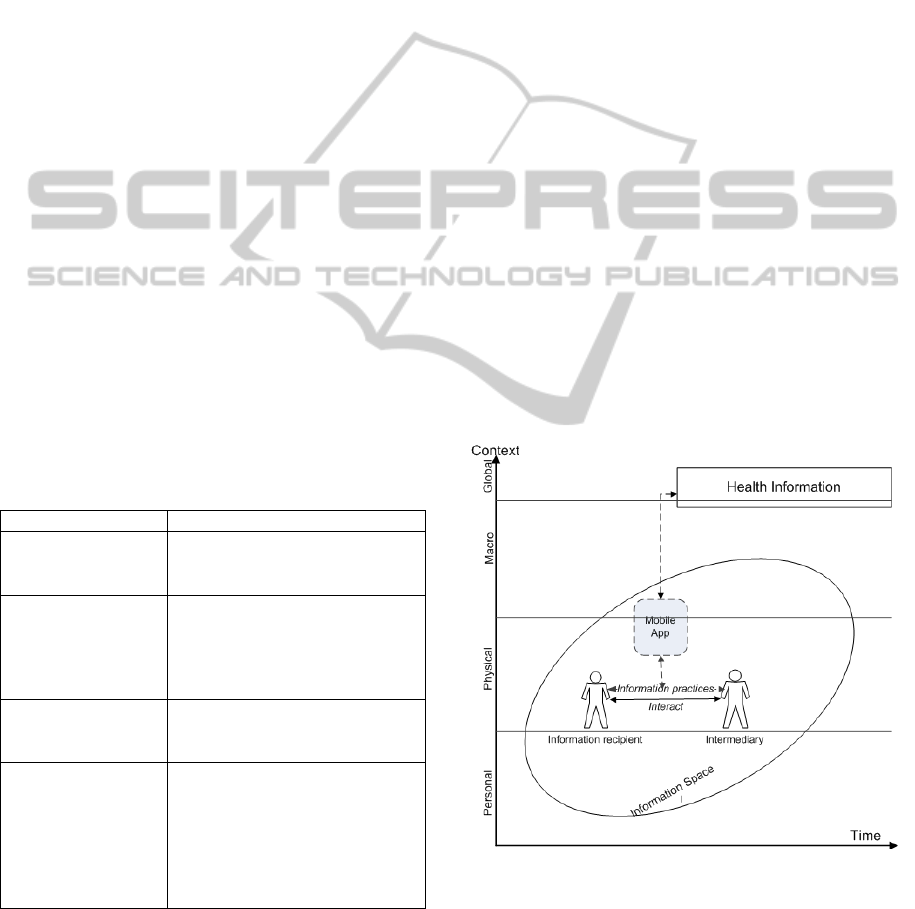
Figure 1: Considerations for access and use of health
information.
Static context dimensions – personal, physical,
macro – are depicted on the y-axis. The dynamic
dimension is indicated as time on the x-axis. Health
information appears mostly outside the contexts
MobileApplicationDesignforHealthIntermediaries-ConsiderationsforInformationAccessandUse
327

relevant to intermediaries. The information space
represents those information practices of the
intermediary in interacting with recipients. The
proposed mobile application connects intermediaries
and recipients with health information. Without this
connection, they are isolated.
Ultimately, the proposed model offers two
fundamental design considerations for fluid
interactions and relationships between users: 1)
Determine the static context dimensions across three
levels: personal (subjective, experiential realms);
physical (temporal, spatial, material realms); and
macro (geographic and socio-economic realms); and
2) Determine the dynamic information space in
terms of information practices, relations, and user
experiences (the ‘fourth context’). This concerns the
interaction between intermediaries and recipients,
especially related to information practices, objects
and –behaviour.
5 CONCLUSIONS
In this position paper, we uncover two critical design
considerations in mobilising health information for
intermediaries. Future research may look to unpack
the interplay between static and dynamic contexts,
and consider the deep ecology of health information
practice, especially in emerging contexts.
ACKNOWLEDGEMENTS
The authors acknowledge the INDEHELA
Information Systems Development for Development
(ISD4D) programme in funding this research.
REFERENCES
Bilbao-Osorio, B., Dutta, S., & Lanvin, B. 2013. The
Networked Readiness Index 2013: Benchmarking ICT
Uptake and Support for Growth and Jobs in a
Hyperconnected World. Geneva: World Economic
Forum.
Bold, W., & Davidson, W. 2012. Mobile Broadband:
Redefining Internet Access and Empowering
Individuals. In Dutta, S., & Bilbao-Osorio, B. (eds.),
The Global Information Technology Report 2012:
Living in a Hyperconnected World. pp. 67-77.
Geneva: World Economic Forum.
Bradley N. A. & Dunlop M. D. 2005. Towards a
Multidisciplinary Model of ‘Context’ to Support
Context-Aware Computing. Human-Computer
Interaction. 20(4). p.403-446.
Chetley, A. (Ed.). 2006. Improving health , connecting
people : the role of ICTs in the health sector of
developing countries. A framework paper: 1–65.
Dourish, P. & Anderson, K. 2006. Collective information
practice: Exploring privacy and security as social and
cultural phenomena. Human-computer Interaction.
21:319-342.
Dourish, P. 2004. What We Talk About When We Talk
About Context. Personal and Ubiquitous Computing,
8(1), 19-30.
Katz, J. E. & Rice, R. E. 2008. Public views of mobile
medical devices and services : A US national survey
of consumer sentiments towards RFID healthcare
technology. 8:104-114.
Kujala, S., & Kauppinen, M. 2004 Identifying and
Selecting Users for User-Centered Design.
Proceedings of Nordic Conference on Computer-
Human Interaction, ACM, 297-303.
Leon, N. & Schneider, H. 2012. MHealth4CBS in South
Africa: A review of the role of mobile phone
technology for the monitoring and evaluation of
community based health services. Cape Town,
Medical Research Council and University of Western
Cape.
Mechael, P., Searle, S. 2010. Barriers and Gaps Affecting
mHealth in Low and Middle Income Countries :
Policy White Paper. 1-79.
Neter, E., Brainin, E. 2012. eHealth Literacy: Extending
the Digital Divide to the Realm of Health Information.
J Med Internet Res., 14(1): 19.
Norris, A. C., Stockdale, R. S., Sharma, S. 2009. A
strategic approach to m-health. Health Informatics
Journal, 15(3):244-253.
Perez, A. M., Ayo-Yusuf, O. A., Hofman, K., Kalideen,S.,
Maker, A., Mokonoto, D., Morojele,N.,Naidoo,P.,
Parry, C., Rendall-Mkosi, K. & Saloojee, Y. 2013.
South Africa Medical Journal. 103(3):147-149.
Räsänen, M. & Nyce, J. M. 2008. Rewriting Context and
Analysis: Bringing Anthropology into HCI Research.
Advances in Human Computer Interaction.
Roto, V., Väätäjä, H., Jumisko-Pyykkö, S., Väänänen-
Vainio-Mattila, K. 2011. Best practices for capturing
context in user experience studies in the wild.
Proceedings of MindTrek’11, ACM.
Ruxwana N. L., Herselman M. E., Pottas D. and Ouma S.
2010. Advocating a quality assurance model for the
implementation of e-health solutions in rural South
Africa. Health Information Management Journal,
39(1): 36–40.
Pakenham-Walsh, N., Bukachi, F. 2009. Information
needs of health care workers in developing countries: a
literature review with a focus on Africa. Human
Resources for Health, 7(30).
Williams, A., Kabisch, E. & Dourish, P. 2005. From
interaction to participation: Configuring space through
embodied interaction. Proceedings of the 7th
international conference on ubiquitous computing.
M.Beigl et al. (Eds.): 287-304.
HEALTHINF2014-InternationalConferenceonHealthInformatics
328
