
A Decentralized Pseudonym Scheme for Cloud-based eHealth
Systems
Liangyu Xu and Armin B. Cremers
Institute of Computer Science, University of Bonn, 53117 Bonn, Germany
Keywords: Pseudonym, EHR, Healthcare, Cloud, eHealth, Security, Privacy.
Abstract: A decentralized pseudonym scheme is proposed for providing storage, encryption and authentication of
patients’ EHRs in cloud-based eHealth systems. The pseudonyms of a patient are generated from the
patient’s secrets and each of them is used as the index of an EHR entry of the patient. An encryption key
derived from the pseudonym can be used to encrypt the corresponding EHR entry. The pseudonyms can
also be used for the patient proving the ownership of the EHR without disclosing the identity of the patient.
Some protocols and remarks for using the pseudonym scheme are also discussed.
1 INTRODUCTION
Storing shared EHRs (Electronic Healthcare Record)
(Garets & Davis, 2006) at a place which can be
accessed from anywhere is an attractive feature in
eHealth (electronic healthcare) systems. Each patient
owns an EHR containing many EHR entries which
detail the healthcare information of the patient. The
sharing of EHR can improve the quality of diagnosis
and treatment, and even enable the patients to view
and manage their own EHRs through their own
devices (Ruland et al., 2008).
The cloud (Mell & Grance, 2011) is an ideal
media for storing EHRs providing wide access,
because it is able to offer ubiquitous services to
customers over the Internet (Rui & Ling, 2010).
However, many challenges exist for adopting the
cloud as the storage media for EHR data in an
eHealth system. Since the EHRs of many patients
are stored at a central place, the cloud, there must be
an efficient approach to index the EHR entries and
map the EHR entries to their owners. i.e., the cloud
needs to be able to provide fast access to the EHR
entries from queries of different patients. Another
challenge is that since the cloud’s resources are
assumed to be publicly accessed and the cloud itself
may also be malicious (Deng et al., 2011), the
storage media for the patients’ EHRs is not
physically secure anymore, which makes the EHRs
face more potential attacks from external adversaries
as well as from corrupt insiders. Thus, the contents
of the EHRs in the cloud should be properly
protected, usually by encryption, and should only be
accessible by the appropriate users, i.e. the patients
themselves and some authorized persons. Another
challenge is that the patients’ identities should not be
disclosed and/or linked to the EHRs by any person
not intended to be able to. Even the cloud should not
know the identities of the patients. Although the
EHR contents are encrypted, it is not secure to
expose the patients’ identities, for attackers will
possibly acquire general knowledge of the patients’
healthcare activities (e.g., the attackers may discover
at least which doctors one patient has visited from
the doctors’ signatures) and even more from
analyzing the contents in EHRs stored in the cloud
(Stingl & Slamanig, 2008).
However, sometimes the EHR entries need to be
updated by the patients, doctors or pharmacists (e.g.,
an update of a prescription in an EHR entry when
the prescription is used in a pharmacy; the patient
manages his own EHR entries like setting custom
access control; etc.), so the cloud has to be able to
authenticate the patients and verify the ownership of
the EHR entries in order to avoid illegal changes by
attackers. It would be better that the authentication
process not leak any information about the patients’
identities to the cloud or possible attackers.
In this paper we discuss how a decentralized
pseudonym scheme can act in the cloud-based
eHealth systems for the purpose of EHR storing and
protecting, while providing the ability for the cloud
to authenticate the ownership of EHRs without
230
Xu L. and Cremers A..
A Decentralized Pseudonym Scheme for Cloud-based eHealth Systems.
DOI: 10.5220/0004747602300237
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2014), pages 230-237
ISBN: 978-989-758-010-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

knowing the identities of the patients, besides
protecting the identities of patients.
The remainder of this paper will be organized as
follows. We list and discuss some previous related
work in section 2. Section
3 gives a simple model of
cloud-based eHealth systems and shows generally
how pseudonyms are used to protect patient privacy
while performing EHR storing, retrieving,
managing, and ownership authenticating. A concrete
pseudonym design will then be presented in section
4. Several detailed evaluations and points of
discussion will be addressed in section 5. The last
section 6 presents some conclusions and an outlook
on future work.
2 RELATED WORK
Many efforts have been made recently to migrate
EHRs which are scattered in clinics and hospitals
into “the cloud”; an important issue of this task is
security and privacy concerns, because the
disclosure of healthcare information of patients may
cause severe problems, especially to the patients
(Alemán et al. 2013). There exist some healthcare
clouds such as Microsoft HealthVault (Microsoft,
2007), where registered patients claim and manage
their personal EHRs themselves, including sharing
their EHRs with selected doctors or other desired
persons (These EHRs are often referred as PHRs
(Tang et al., 2006)). The privacy protection of such
kind of services depends on the security mechanism
implemented by the cloud (Löhr et al., 2010). A
prerequisite to guarantee the privacy in such services
is that these healthcare cloud providers should be
completely trustworthy to protect the EHRs
properly. Other research proposes solutions that
remove the high dependency on trusting the cloud,
cf. e.g. (Alhaqbani & Fidge, 2008; Li et al., 2011).
The EHRs in these systems are encrypted by keys
unknown to the cloud. These solutions may protect
the patients’ privacy better, but they make the
systems considerably more complex.
To protect the identities of the patients,
pseudonyms (Pfitzmann & Köhntopp, 2001) can be
utilized to hide the real identity information.
Patients’ real identities appearing in the EHRs are
removed or replaced by the pseudonyms. There are
some pseudonym schemes in which a centralized
party (which needs to be trusted) generates the
pseudonyms for the patients (Alhaqbani & Fidge,
2008). In such schemes, it is easy to avoid
pseudonym collision, and the centralized party can
easily provide the service for other parties (e.g. the
cloud) of authenticating the patients. The centralized
party has to be online with high availability.
Moreover, the existence of such a centralized party
will possibly harm the privacy of the patients, as a
successful attack on the centralized party or a
corrupt insider will cause privacy infringement to
the patients. In eHealth systems, as the EHR data are
top private information for patients, the existence of
a trusted party that has the ability to know patients’
identities or the plaintext of their EHR data and has
potential risk to be attacked would not be accepted
by many patients.
It is highly desirable that pseudonym generation
be decentralized, where no trusted party exists for
generating and authenticating pseudonyms. There
are some decentralized pseudonym schemes for
eHealth systems. In (Li et al., 2011), such a
pseudonym scheme is used to index the EHR entries.
The pseudonyms can only be reproduced to retrieve
the EHR entries from the cloud by fetching two parts
of secret information which were separately stored
in two trusted parties when the pseudonyms were
generated at the first time. However, this solution
would require the patients to store much information
in the smart cards, and the existence of trusted
parties places disclosure risk on the patients’
privacy. In (Lysyanskaya et al., 2000), a general
pseudonym scheme is proposed for generating
pseudonyms for one user (possessing a secret) and
using the credentials issued by one organization at
other organizations without revealing the user’s
identity. Each user’s pseudonym is generated based
on the user’s secret with the organization’s
participation. They minimize the dependency on a
trust party, and the security relies on the user-only
known secrets. However, the scheme might
encounter problems when a central cloud is utilized
in eHealth systems.
In a cloud-based eHealth system, Not only
should a pseudonym scheme be carefully designed
to protect the identities of the patients from being
disclosed, but also some protocols are needed to
apply the pseudonym scheme correctly to protect the
privacy of the patients while keeping the healthcare
processes running smoothly. One motivation of this
paper is to design such a pseudonym scheme which
can pseudonymize patients’ identities with provable
security, and also provide corresponding encryption
key management and authentication algorithm
without disclosing patient’s identities. Another
intention of the paper is to apply the pseudonym
scheme to a typical cloud-based eHealth system, by
discussing the possible risks of privacy and identity
disclosure and corresponding solutions.
ADecentralizedPseudonymSchemeforCloud-basedeHealthSystems
231
3 USE OF PSEUDONYMS
IN CLOUD-BASED eHEALTH
SYSTEMS
3.1 Our Model of a Cloud-based
eHealth System
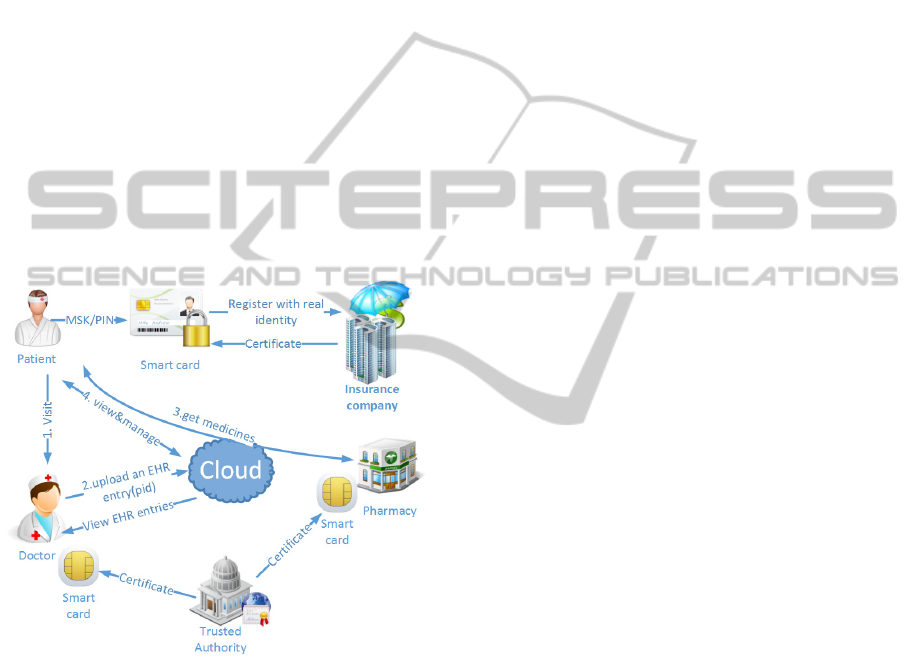
We model a basic cloud-based eHealth system as
shown in Figure 1. The cloud plays the role of
associating almost all the participating eHealth
entities such as patients, doctors, pharmacists, and
health insurance companies (will be abbreviated as
insurance companies in the following). We note that
the pseudonym scheme proposed in this paper does
not depend on the existence of insurance companies.
It would be easier to adapt the pseudonym scheme in
eHealth systems without an insurance company as
the insurance companies could also be possibly
curious to know the health information of their
clients (i.e. patients).
Figure 1: A simple model of cloud eHealth systems.
Each patient has a set of secrets consisting of MSK
and PIN, which are only known by the patient
himself, where MSK is the main secret key of the
patient, usually stored in the protected memory of a
smart card, for which a PIN is employed to
authenticate the patient to avoid abuse. The MSK of
the patient will be used to generate pseudonyms,
encrypt the EHR data, prove the patient’s ownership
of the EHR to the cloud and in some other functions.
Hence, it should be properly protected in the smart
card and safely backed up by the patient in case of
loss of the smart card. The special issues of smart
card loss are discussed in section 5.
The patient’s real identity is only known by the
insurance company while the patient has to register
there in the beginning. Each patient will get a
certificate from the insurance company with a
corresponding private key which is only known by
the patient (We will abbreviate the patient’s
corresponding private key from insurance company
as SKI). The patient’s identity should not be
included in the certificate. Typically, a certificate
number, which can only be mapped to the patient’s
real identity by the insurance company, a token of
the insurance company, the public key of the patient,
and the period of validity will be necessary in the
patient’s certificate.
The healthcare providers (e.g. doctors and
pharmacists) also need to get certificates from a
trusted authority with self-known private keys. The
trusted authority could be the health department of
the government which confirms the healthcare
providers’ qualifications by issuing them the digital
certificates in which information like healthcare
categories and healthcare providers’ identities can be
enclosed. The certificates and the corresponding
private keys could also be stored in the protected
memory of smart cards issued to the healthcare
providers with authenticating PINs. The healthcare
providers’ private keys can be used to sign the
record sections of the patient’s EHR data and
prescriptions. The private keys of the patients (SKIs)
and the healthcare providers would be used for
signing bills, which can be received through the
cloud and will be paid by the insurance company.
The billing procedure is not depicted in the figure
for simplicity.
3.2 Use of PID (Pseudonyms)
to Conceal Patients’ Identities
A typical pseudonym generation occurs at a doctor’s
practice when a patient visits the doctor, taking
along his smart card. The doctor checks the validity
of the patient by checking certificate and challenging
the patient’s SKI, with the insurance company's root
certificate which could also be issued by a trusted
authority. The doctor does not necessarily know the
identity of the patient. But in practice, as the doctor
is assumed to be trusted, it is usually the case that
the identity (at least parts of identity information
such as name, gender, age, and telephone number) of
the patient is known to the doctor. After the doctor’s
diagnosing and treating, the doctor writes down a
record (including the diagnosis, examinations,
treatment and other information), with a prescription
stating the medicines that the patient needs to take
HEALTHINF2014-InternationalConferenceonHealthInformatics
232

and buy at a pharmacy. Meanwhile, a new
pseudonym (PID) and an encryption key (EK) are
generated by the patient’s smart card from the MSK.
Both the record and the prescription will be
encrypted by the encryption key and signed by the
doctor’s private key. Then, all the data from the
doctor is uploaded to the cloud along with an index
header, the new PID, forming an EHR entry for the
patient. Thus, an EHR entry needs to be at least
compatible with the following sections where “||”
means concatenation,
EHR entry = PID || Enc
EK
(record) || sig
d
(record)
||Enc
EK
(prescription) ||sig
d
(prescription).
The cloud can validate the doctors by verifying
their certificates and challenging their private keys
with the trusted authority’s help to avoid illegal
uploading of EHR entries. Actually, no one else is
able to generate a meaningful EHR entry for a
patient, as nobody can generate valid EKs or PIDs of
the patient without knowing the MSK and each pair
of valid PID and EK is only used for one EHR entry.
Forged EHR entries can be easily recognized and
removed by the patient through checking the
correctness of decryption or the PIDs.
3.3 Use of PID to Index EHR Entries
The cloud stores the EHR entries of each patient by
indexing the PID section of the EHR entries. We
expect that each EHR entry would have a unique
PID. The special problem of PID collision is
discussed in section 5. The cloud does not keep any
registration information of the patient, so the cloud
does not know the identity of the patient other than
the PIDs. As most of the essential contents in the
EHR entries are encrypted with the encryption keys
which are unknown to the cloud, it is unable to
disclose the identities of patients or any meaningful
information in the EHR data, even if the cloud is
curious to know. For the same reason, attackers who
can access all EHRs in the cloud can neither get any
useful information from the EHRs nor the identities
of the patients.
The cloud returns the EHR entries upon the PIDs
the patients reproduce and send to the cloud when
the EHR entries are retrieved from the cloud.
3.4 Use of PID to Authenticate
the Ownership of EHR
Pseudonyms are used by the cloud to authenticate
the patients’ ownerships on their EHRs when the
EHRs need to be updated by their owners. A typical
scenario for an EHR entry that needs to be updated
is when a patient goes to a pharmacy to buy
medicines by using the prescription which is
enclosed in an EHR entry. The patient retrieves the
EHR entry from the cloud by providing the cloud a
PID (the PID of the EHR entry with an unused
prescription can be temporally stored in the smart
card for fast query) and shows the decrypted
prescription with the doctor’s signature to the
pharmacist. The pharmacist can check the
prescription’s signature of the doctor. If the
signature is valid, the pharmacist generates an
additional signature on the prescription indicating
that the prescription has been used and asks the
patient to update the original prescription’s signature
section of the EHR entry by including the
pharmacist’s signature. The cloud needs to check
beforehand whether the patient is the owner of the
EHR entry or not. Only if he is, the cloud updates
the old prescription’s signature section by adding the
pharmacist’s signature. After the pharmacist
confirms that the patient has updated the prescription
signature, the medicines are sold to the patient. Due
to the updating of the prescription signature, the
updated EHR entry with a pharmacist’s signature
looks like this,
updated EHR entry = PID || Enc
EK
(record) ||
sig
d
(record) ||Enc
EK
(prescription) ||sig
d
(prescription)
|| sig
p
(prescription).
4 THE DESIGN OF A NEW
PSEUDONYM SCHEME
4.1 Secrets Setup
A patient’s main secret key MSK and PIN are
initially set and only known by the patient when the
patient receives a blank smart-card from a system
provider that may also deploy the healthcare
application software in the cloud. The initialization
of MSK and PIN needs the help of some software
coupling with the smart card. The MSK is stored in
the protected memory of the patient’s smart card in
which the password PIN usually can be set by the
patient to avoid abuse of the smart card.
The patient chooses a k-bits (k is usually no less
than 160) prime integer
q, and another prime number
p (the size of p is usually not less than 512 bits)
which satisfy
q|(p-1). By
∗
we denote a
multiplicative group modulo
p. The patient finds ∈
∗
, to be of order q modulo p. Then g is the
generator of the subgroup
. By randomly
choosing∈
, a patient’s MSK is formed: [x, g, p,
ADecentralizedPseudonymSchemeforCloud-basedeHealthSystems
233

q].
According to difficulty of the discrete logarithm
problem (McCurley, 1990), given
g, h ∈
, such
that
h was selected from
uniformly at random, it
is hard to compute an integer
x such that
g
x
= h mod p.
The complexity to find such x is no less than O(
)
(Lim & Lee, 1997). For ease of notation, we will
sometimes drop the “mod
p” part of the arithmetic
expressions in
. We build up our secure
pseudonym scheme based on the discrete logarithm
problem in the subgroup
.
4.2 Algorithm for Generating PIDs
Assume that previously a patient has already used i
PIDs (i.e.,
PID
1
, PID
2
, ⋯, PID
i
). We express
0
as
(
0
,
0
) which is (0, 0) by default (refer to section 5
for more considerations of choosing
0
to avoid
pseudonym collisions). Following is the algorithm to
generate the i+1
th
pseudonym PID
i+1
where “||”
means bit concatenation.
INPUT:
0
= (
0
,
0
), i, MSK, PIN (to be
authenticated by the smart card)
OUTPUT:
1
,
+1
+1
=
KHash
(i+1||
0
||
0
, ), where KHash is a
keyed hash function by key x
+1
=
||
,
+1
=
+1
= Hash(
+1
||
+1
)
Since the order number of the last used PID is
needed to generate the next new PID, the order
number of the last PID should be stored somewhere,
e.g., in the smart card.
+1
can be used as the
encryption key (it might be necessary to be truncated
or padded according to the encryption algorithm) for
encrypting the private contents of the EHR entry
with the index of the new pseudonym
1
.
4.3 Algorithm for Reproducing PIDs
All the PIDs and EKs can be reproduced one by one
through the following algorithm.
INPUT:
,
, MSK, PIN, the
number
last of last used pseudonym
OUTPUT:
PID
1
~PID
last
,
~
FOR i=1 to last DO
||
||
,,
|
|
,
= Hash(
||
)
The above algorithm shows how to reproduce all
the used pseudonyms and the encryption keys. In
fact any single
PID
i
and EK
i
pair can be reproduced
by executing one single loop of the above algorithm.
4.4 Protocol for Authenticating
the Ownership of EHR Entries
Following is the protocol for the cloud (abbreviated
as C) verifying a patient’s (abbreviated as P)
ownership of one EHR entry with pseudonym
PID,
where “→” means sending a message.
INPUT: an EHR entry with PID in the cloud; p, q
of the patient’s MSK are known by the cloud
OUTPUT:
Yes or No.
P → C: Patient sends (
, ) such that PID =
Hash(a||b)
C: checks whether PID ?= Hash(a||b). If not, C
returns
No; otherwise continues.
P → C: Patient randomly chooses s, calculates
and sends (A=a, B=a
s
mod p)
C → P: Cloud randomly chooses and sends
c
P → C: Patient computes and sends y = s+cx mod
q
C: checks
a
y
?= Bb
c
mod p. If yes, C returns
Yes; otherwise returns No.
The security of the above algorithm and protocol
relies on the difficulty of the discrete logarithm
problem in
and the one-way property of the hash
function. Only the patient possessing the secret
x can
respond to the cloud’s challenge correctly. Anybody
else who wants to impersonate the patient is required
to compute the discrete logarithm in
which is
conjectured to need the complexity of O(
) (Lim
& Lee, 1997).
5 DISCUSSION
5.1 Risks and Countermeasures in
Protecting Patients’ Privacy by
Pseudonyms
5.1.1 Cloud’s Knowledge of Complete PID
Sets of Patients
A patient’s frequent access to his EHR may let the
cloud know all the patient’s PIDs. Since all the
patient’s pseudonyms are independent without
knowing the patient’s secrets, common attackers
could not know which EHR entries belong to one
patient. However, the cloud may know more about
the pseudonyms of one patient than the common
HEALTHINF2014-InternationalConferenceonHealthInformatics
234

attackers outside. The patient or the doctor treating
the patient may have to access all the patient’s EHR
entries in one query. They have to send all the
pseudonyms of the patient to the cloud for retrieving
all the corresponding EHR entries. If the cloud
wants to, it can record the pseudonym set from a
single querying source (e.g., network IP). Although
in general, it is difficult to prevent the cloud from
gaining the pseudonym set knowledge, some tricks
can be used to let the cloud not know the exact
pseudonym set. E.g., the patient or doctor can send
some fake pseudonyms (fake pseudonyms mean the
pseudonyms existing in the cloud but belonging to
other patients. As we assume the pseudonyms in the
cloud are public available resources, anyone can
view these pseudonyms freely.) to the cloud with the
actual pseudonyms; the patient or doctor can use
anonymous proxies and other network technologies
to avoid to be traced.
5.1.2 Dealing with Pseudonym Collision
In the above pseudonym scheme, the secret
parameters (MSKs) for generating pseudonyms for
patients are chosen by the patients themselves
independently. It is possible that two patients choose
a same parameter, although the probability is very
low. This would certainly cause problems if it
happened, as the pseudonyms generated by the two
patients will be equal. A solution is to utilize
to avoid the occurrence. The system provider of the
smart card can control that all patients will have
different
s, or the
can be set by each
patient to be one of the patient’s unique identifiers
(e.g., identity no., passport no., SSN, etc.).
According to the algorithm of pseudonym
generation, it is expected that different pseudonym
sequences will be produced. Although this solution
can prevent obvious collision of two pseudonym
sequences of two patients, there is still very small
probability that two arbitrary pseudonyms (from one
patient or two patients) might collide since the
generating scheme is not an injection. A solution is
to count on the encryption or HMAC (Keyed
Hashing for Message Authentication Code) on EHR
data. That is, the collision of two pseudonyms is
allowed by the cloud. But the EHR data must have
been encrypted with a detection of an error or have a
HMAC by different secret keys. The two EHR
entries with same pseudonym are highly expected to
have different encryption keys or different HMACs
by using the pseudonym scheme designed in this
paper, so the patients can recognize which one is the
desired one upon receiving more than one answer
from the cloud when they retrieve the EHR entries
by providing a pseudonym to the cloud. The collided
EHR entries which cannot be correctly decrypted or
cannot get a correct HMAC will be dropped as
undesired EHR entries by the patients. As for the
possible repeated occurrence of pseudonyms, the
cloud should not use the pseudonym section alone as
the main index key for the database table.
Another problem caused by the possible collided
pseudonyms is that, as the cloud cannot tell which
patient is the exact owner of two EHR entries with
one collided pseudonym from two different patients,
a patient could update the other patient’s EHR entry
which does not belong to him/her. One solution is a
patient only creates updates in new EHR entries with
reference to the updated entries. However, in many
cases, the cloud could do some further check to
confirm whether the patient is making a valid
updating on the EHR entry with a collided PID or
not. For example, in the case where a patient wants
to update the prescription’s signature section, the
update should include a valid signature on the
prescription from a pharmacist, so the cloud can
check the pharmacist’s signature to prevent arbitrary
updating by the patient. While in other cases, where
the updates are made by the patient, (e.g., to set
custom access control) the updates should be
encrypted or have some integrity check mechanism.
The malicious updates can be abandoned by the real
owner of the EHR entry, even if the cloud did not
carry out the further check or wrongly accepted
some malicious updates.
5.1.3 Trust Mode of the Cloud
The cloud in this paper is not necessary to be trusted,
but it is expected to be honest. This is usually the
case in practice. The physical storages of public
clouds are distributed and the data stored in them
may be vulnerable for abuse by the cloud itself or
easily be obtained by a skilled attacker. In this paper,
we do not store in the cloud more information (such
as patient’s registration information) than protected
data or publicly available data (e.g., root certificates
of trusted authority for validating doctors). But we
require that the cloud acts honestly, i.e., the
healthcare application software running deployed by
the “system provider” on the cloud is honest. For
example, as the cloud does not intend to tamper the
EHR data, it will also follow the protocol designed
for authenticating the ownership of the EHR entries
before allowing an update on them. We also require
the cloud to understand some structure information
of the EHR entries and to process just the desired
ADecentralizedPseudonymSchemeforCloud-basedeHealthSystems
235

sections (e.g. the section of a pharmacist’s signature
on the prescription) of the EHR entries in an honest
manner. If the protocols are properly designed, the
cloud cannot benefit from dishonesty except
disturbing the normal procedure of the activities in
eHealth system.
5.2 Computation Capability
of the Smart Card
The pseudonym scheme in this paper might bring
too much computation to the smart cards of the
patients if all the computations need to be done in
the smart cards. As shown in the section 4, one
single pseudonym generation or reproduction needs
three hash computations and two modular
exponentiation computations, where hash
computation is usually fast but the modular
exponentiation computation is more time
consuming. Noticing that the last two hash
computations and the first modular exponentiation
computation do not involve the secret
x, they can be
done by outside connected devices (e.g., the doctor’s
or the patient’s computer). In a typical
implementation of the modular exponentiation
computation (Schneier 1996), about two thirds of the
modular multiplication computations in the second
modular multiplication computation will not involve
the secret power x, so these modular multiplication
computations can also be moved to outside devices.
Thus, the computations needed to be done by the
smart cards are only one hash computation and part
of one modular multiplication computation. It
greatly decreases the computation burden of the
smart cards with a bit increase of the serializable IO
manipulations.
5.3 Recovery upon Smart Card Loss
The patients’ secrets MSKs and PINs should have a
secure backup in the custody of the patients in case
the smart cards are lost, since these secrets are only
known by the patients, nobody else can recover
these secrets instead. Once a patient lost his smart
card, he needs to get a new one from the system
provider, and restore the backup secrets into the new
card. Then he needs to re-register at the insurance
company and get a new certificate with a new
corresponding private key. The EHR data stored on
the cloud can be reused by the new card afterwards.
The order number
last of PID
last
can be recovered by
the patient sending the reproduced pseudonyms from
the first one to the last one upon which the cloud can
return correct EHR data. However, the feasibility of
having all patients keeping binary secrets depends
on the practical condition. Some feasible solutions
are available. E.g., patients can use some public
service (e.g. network storage service) to store their
secrets. The general doctors of the patients could
also help keeping the secrets. The secrets stored at
public storage or general doctors’ computers could
be protected by patients-only known passwords.
Although the security of the passwords is limited, it
can release the complete trustworthiness on the
general doctors or public storage service providers a
little.
In some particular case, if the PIN and the smart
card are taken by some attacker other than the
patient self, but the MSK stored in the smart card is
not known to the attacker (this is the common case
in practice), the attacker could access the patient’s
existing EHR entries. The patient who knows the
MSK can cooperate with the cloud to change the EK
and even MSK to disable the old EHR entries. If the
MSK is also compromised by the attacker (this is
very rare in practice), the attacker could certainly do
what the patient can. The only possible way is that
the patient cooperates with the cloud to change the
MSK and EK to disable the old EHR entries in time
(before the attacker could do that).
6 CONCLUSIONS
In this paper, we presented how to use patients’
pseudonyms for indexing, encrypting, and verifying
the ownership of the EHRs with patients’ privacy
properly protected in cloud-based eHealth systems.
A new decentralized pseudonym scheme was
proposed accordingly. The security of the scheme is
provable as it is based on the discrete logarithm
problem and the one way property of hash functions.
Although the security of the scheme can be proved,
it faces much vulnerability in healthcare activities in
cloud-based eHealth systems, which are complex
systems involving many entities and complicated
application scenarios. In comparison with the
existing pseudonym schemes, our proposed scheme
is dedicated for cloud-based eHealth systems. We
minimize the data that the patients need to store on
the smart cards to generate a new PID or to
reproduce previous PIDs. We also lower the
dependency on the trustworthiness of the cloud, and
move the trust base to patients themselves and some
technical assumptions (e.g., the smart card with
protected memory and authentication PIN). Some
corresponding protocols are carefully designed to
apply the pseudonym scheme into cloud-based
HEALTHINF2014-InternationalConferenceonHealthInformatics
236

eHealth systems. We discussed several common
application scenarios, and pointed out some possible
problems (e.g., PID collision, smart card loss, etc.),
and attacks (e.g., malicious cloud, ISP, insurance
companies, eavesdroppers, etc.), with corresponding
countermeasures. We also provide an optional
scheme for decreasing the computation burden in the
smart cards. These would make the proposed
pseudonym scheme more feasible to be implemented
in practical eHealth systems.
As future work, the computational cost of the
pseudonym scheme needs to be evaluated in
prototype eHealth systems equipped with simulated
cloud, smart cards and users. What is more, we will
continue to investigate the proposed pseudonym
scheme as to feasibility and compatibility with other
technologies in practical eHealth systems.
ACKNOWLEDGEMENTS
We would like to thank Adrian Spalka who raised
many challenges and comments from the viewpoint
of practical eHealth systems to this paper. Also we
appreciate Jan Lehnhardt for discussing with us
about the details of the scheme. What is more, he
commented on the early version of this paper and
helped with much literal work.
REFERENCES
Alemán, J. L. F., Señor, I. C., Lozoya, P. Á. O., Toval, A.,
2013. Security and privacy in electronic health
records: A systematic literature review. Journal of
biomedical informatics.
Alhaqbani, B., Fidge, C., 2008. Privacy-preserving
electronic health record linkage using pseudonym
identifiers. HealthCom 2008. 10th International
Conference on e-health Network- ing, Applications
and Services: IEEE. pp. 108-117.
Deng, M., Petkovic, M., Nalin, M., Baroni, I., 2011. A
Home Healthcare System in the Cloud--Addressing
Security and Privacy Challenges. 2011 International
Conference on Cloud Computing: IEEE. pp. 549-556.
Garets, D., Davis, M., 2006. Electronic medical records
vs. electronic health records: yes, there is a difference.
Policy white paper. Chicago, HIMSS Analytics.
Li, Z.-R., Chang, E.-C., Huang, K.-H., Lai, F., 2011. A
secure electronic medical record sharing mechanism
in the cloud computing platform., 15th International
Symposium on Consumer Electronics (ISCE): IEEE.
pp. 98-103.
Lim, C. H., Lee, P. J., 1997. A key recovery attack on
discrete log-based schemes using a prime order
subgroup. In Advances in Cryptology—CRYPTO'97,
pp. 249-263: Springer.
Löhr, H., Sadeghi, A.-R., Winandy, M., 2010. Securing
the e-health cloud. Proceedings of the 1st ACM
International Health Informatics Symposium: ACM.
pp. 220-229.
Lysyanskaya, A., Rivest, R. L., Sahai, A., Wolf, S., 2000.
Pseudonym systems. Selected Areas in Cryptography:
pp. 184-199.
McCurley, K. S., 1990. The discrete logarithm problem.
Proc. of Symp. in Applied Math. pp. 49-74.
Mell, P., Grance, T., 2011. The NIST definition of cloud
computing (draft). NIST special publication, 800
(145): 7.
Microsoft., 2007. HealthVault. www.healthvault.com.
Pfitzmann, A., Köhntopp, M., 2001. Anonymity,
unobservability, and pseudonymity—a proposal for
terminology. Designing privacy enhancing
technologies: Springer. pp. 1-9.
Rui, Z., Ling, L., 2010, 5-10 July 2010. Security Models
and Requirements for Healthcare Application Clouds.
IEEE 3rd International Conference on Cloud
Computing: IEEE. pp. 268-275.
Ruland, C. M., Brynhi, H., Andersen, R., Bryhni, T., 2008.
Developing a shared electronic health record for
patients and clinicians. Studies in health technology
and informatics, 136: 57-62.
Schneier, B., 1996. Applied cryptography. Protocols,
Algorithms, and Source Code in C/Bruce Schneier:
John Wiley, Sons, Inc.
Stingl, C., Slamanig, D., 2008. Privacy-enhancing
methods for e-health applications: how to prevent
statistical analyses and attacks. International Journal
of Business Intelligence and Data Mining, 3 (3): 236-
254.
Tang, P. C., Ash, J. S., Bates, D. W., Overhage, J. M.,
Sands, D. Z., 2006. Personal health records:
definitions, benefits, and strategies for overcoming
barriers to adoption. J Am Med Inform Assoc, 13 (2):
121-6.
ADecentralizedPseudonymSchemeforCloud-basedeHealthSystems
237
