
CHARMing Clinical Pathways
Modeling of Clinical Pathways based on the Goal-Oriented Ontological
Framework CHARM
Satoshi Nishimura
1
, Genma Nishijima
1
, Yoshinobu Kitamura
1
, Munehiko Sasajima
1,2
,
Toshihiro Takeda
3
, Yasushi Matsumura
3
and Riichiro Mizoguchi
4
1
The Institute of Scientific and Industrial Research, Osaka University, 8-1 Mihogaoka, Ibaraki, Osaka, 567-0047, Japan
2
YMP-Mundus Corporation, YMP Tanimachi Building Minami-kan 10F, 1-1-14 Izumi-cho, Chuoh-ku,
Osaka, 540-0019, Japan
3
Department of Medical Informatics, Graduate School of Medicine, Osaka University, 2-15 Yamada-oka, Suita,
Osaka, 565-0871, Japan
4
Japan Advanced Institute of Science and Technology, 1-1 Asahidai, Nomi, Ishikawa, 923-1292, Japan
Keywords: Action Model, Clinical Pathways, Knowledge Representation, Ontology Engineering.
Abstract: Much procedural knowledge in the medical domain, such as clinical practice guidelines, nursing manuals,
and clinical pathways (abbreviated to CPs), is documented and shared. This paper concentrates on the CP,
which represents a standard time-sequence of actions carried out by clinical staff for each disease. With the
aim not of replacing the conventional form of CPs in a clinical setting but of facilitating description and
revision of knowledge by knowledge managers, we have proposed CHARM, which is a goal-oriented, tree-
structured model based on an ontology of actions. The aim of the work described in this paper is to confirm
the practical ability of CHARM to represent medical actions in CPs in a computer-interpretable way, using
eight real CPs in Osaka University Hospital. CHARM trees in terms of actions defined clearly in the
ontology explicitly represent goals of actions, i.e., why the actions should be needed, and so on, which are
implicit in the conventional CPs. We also confirmed the benefits of CHARM for describing/revising CPs by
the knowledge mangers in a comparison of the actions in CPs, such as finding commonality among CPs,
easy comparison of CPs from a goal-oriented perspective, and explanation of the reasons for differences.
1 INTRODUCTION
In the medical domain, large amount of procedural
knowledge is documented in clinical practice
guidelines, nursing manuals, and clinical pathways
(abbreviated to CP hereafter). CPs and clinical
practice guidelines describe standard (prescriptive)
actions, unlike the record of real actions performed
on a patient, which is descriptive. In this research,
we currently focus on the former.
The ultimate goal of this research project is to
manage procedural knowledge about medical
practice in a unified framework in which these
several kinds of knowledge are stored. We attempt
to use CHARM as the unified modeling framework,
which has been proposed by the authors. (Nishimura
et al., 2013). We aim to integrate the similar
knowledge in nursing manuals, clinical practice
guidelines, and CPs into CHARM trees (hereinafter
called as knowledge model) to systematically handle
it in a consistent manner. We expect that the
framework will be used as follows.
(1) Knowledge managers describe the knowledge
models in CHARM trees and revise them for their
improvement by comparing the trees. They are
leading medical doctors for medical informatics in
hospitals, experienced nurses, and/or experts in
medical societies with knowledge engineers in
information science.
(2) Clinical staff read the knowledge models in a
clinical setting. They, especially, novice nurses,
consult the models as standard actions to be
performed in practical clinical situations.
(3) Novice nurses as learners read the knowledge
models as right sequences of actions to be performed
in education and/or training situations.
This research aims mainly at the use cases of (1)
and (3). In these use cases, we expect the benefits of
211
Nishimura S., Nishijima G., Kitamura Y., Sasajima M., Takeda T., Matsumura Y. and Mizoguchi R..
CHARMing Clinical Pathways - Modeling of Clinical Pathways based on the Goal-Oriented Ontological Framework CHARM.
DOI: 10.5220/0004747002110221
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2014), pages 211-221
ISBN: 978-989-758-010-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

CHARM trees in describing, revising and learning
the knowledge as described below. In the use case
(2) which is not our main aim and not discussed in
this paper, the unified model is transformed into the
conventional representation forms (e.g., the table-
style form of CPs). Thus, in clinical practice, the
medical staff can read the unified knowledge in the
conventional forms familiar to them.
CHARM is a modeling framework of procedural
knowledge based on ontology engineering, aimed at
promoting knowledge sharing and knowledge
inheritance among medical workers (Nishimura et
al., 2013). CHARM, which is an abbreviation of
Convincing Human Action Rationalized Model
(Nishimura et al., 2013), is designed to represent
human actions in a goal-oriented manner. A
CHARM tree clarifies the goal of actions. The terms
used in a CHARM tree are defined based on an
ontology of actions and make the meaning of actions
computer-understandable to some extent. A
CHARM tree explicates the reason for performing
the action by clarifying the goal. Alternative ways of
achieving the goal are also made explicit.
The authors have confirmed the practical
benefits of CHARM for describing and learning the
nursing actions, which corresponds to the use cases
of (1) and (3) above. In the collaborative study
involving nurses, several nursing manuals in a
certain hospital were described based on CHARM.
As the knowledge managers in the use case (1), the
experienced nurses confirmed the benefits of
CHARM in integration of the nursing guidelines in
different hospitals (Nishimura et al., 2013).
Moreover, for the learners in the use case (3),
software designed to browse CHARM trees on tablet
computers has been developed and has been applied
to the training of novice nurses in hospitals
(Sasajima et al., 2013).
There have been some research efforts for
modeling the knowledge of medical procedures in
computer interpretable manner, such as Asbru
(Shahar et al., 1998), PROforma (Sutton and Fox,
2003), GLIF (Boxwala et al., 2004), and SAGE (Tu
et al., 2007). They aim to assist doctors in making
decisions by automatic reasoning based on computer
interpretable models. The aim of our research
project is not the same as theirs, but promoting
knowledge sharing and knowledge inheritance
through using CHARM trees.
In this paper, as the first step to build the
management framework, we discuss description of
existing CPs in the CHARM trees. We also
demonstrate the benefits of CHARM in the use case
(1) above. We try to show that the use of CHARM
helps the knowledge managers compare the CPs
when they want to revise CPs for improvement.
A CP provides a standard medical procedure to
optimize length of hospital stay (Pearson et al.,
1995), to minimize delays and excessive resource-
consumption and to maximize the quality of care
(Zander K., 1988, Coffey et al., 2005). There are
some reports about improvement of outcomes and
reduction of the length of stay thanks to CPs (Hauck
et al., 2004, Madan et al., 2006). Every et al. have
recommended the use of CPs in clinical settings
(Every et al., 2000). Compared with other
representation methods, a CP in a tabular form has
two features. One is a clear representation of time
points (days) on the X axis and the kinds of actions
on the Y axis. The other is representation of the goal
of actions within one day or several days as an
“outcome”. In a CP, however, intermediate goals of
each action are not described.
The authors aim not at replacing the
conventional CP forms with CHARM in the clinical
setting but at facilitating the creation and revision of
CPs by the CP authors as the knowledge manager.
We do not suppose that the doctors and the nurses
use the CHARM trees in the clinical setting.
CPs work well for doctors and nurses who
understand the goal of their actions in clinical
settings. However, some problems may occur to CP
authors, who create and revise CPs. It is difficult to
reuse the parts of a CP when the CP author creates
other CP. In CPs, the time points of the actions and
the rough goals are represented, but the relationships
between actions are not clear. In other words, the
dependency between actions is not clear, so it is
difficult to reuse the parts of the CP. In order to
revise the CPs, it is useful to compare the same
medical procedures which are performed in different
department of a hospital. It is easy to compare the
procedure from a sequence-oriented viewpoint when
the CP author uses the CPs. However, the viewpoint
may not facilitate the CP author to detect the rational
differences because the goals of the actions are not
clear in the CPs. Therefore, the CP author needs
his/her knowledge about the medical procedures and
that takes a load of him/her. The goals of actions
should be clear to facilitate reuse of the parts of the
CPs and comparison of the CPs. The goal of actions
connects the actions to achieve it, so the dependency
between actions becomes clear. The goal of actions
also decreases the load of the CP authors when they
compare the medical procedures in the CPs.
The aim of our study was to describe CPs in the
framework of CHARM and to confirm the following
HEALTHINF2014-InternationalConferenceonHealthInformatics
212

benefits of a CHARM-based representation of
medical actions in CPs used as knowledge sources:
(i) To represent the medical actions in CPs in a
structured way, with the terms defined clearly.
(ii) To clarify the goals of actions, which are implicit
in CPs.
(iii) To compare the medical actions between two
CPs using CHARM trees.
In this research, we built CHARM trees from
eight real CPs used in a hospital. From the results,
the first and second benefits above were confirmed.
Then we compared some CHARM trees and
identified common structures among the trees.
Through this comparison, the third benefit was
confirmed.
This paper is organized as follows. In Section 2,
we introduce CHARM as a representation
framework and describe the contents of real CPs,
and we also explain the method used to build
CHARM trees from CPs. In Section 3, we confirm
the benefits of CHARM. First, we identify
commonalities among CPs, and next, we compare
CPs using CHARM trees. In Section 4, we discuss
the differences between our framework and other
related studies. Finally, in Section 5, we conclude
this paper and mention some topics of our future
work.
2 DESCRIPTION OF CLINICAL
PATHWAYS BASED ON
CHARM
2.1 Charm
CHARM is a goal-oriented, tree-structured model
based on an ontology of actions. Although there is
no common definition of “ontology”, an ontology in
knowledge engineering can be generally defined as
“a system (systematic, operational and prescriptive
definitions) of fundamental concepts and
relationships which shows how a model author
views the target world, and which is shared in a
community as building blocks for models”
(Mizoguchi, 2003). In this project, the roles of the
ontology are to define modelling concepts and to
provide a controlled vocabulary for actions as
discussed below.
A concrete model based on CHARM is called a
CHARM tree. An action is interpreted as a state
change of an object and is described using one of a
number of action terms (verbs) that are defined in
the ontology of actions. A single action is realized
by a sequence of detailed (fine-grained) actions. In
this context, a single action as a state change is
interpreted as a goal of the sequence. Hereafter, we
use the term “achieve” to mean that the sequence
realizes the action as a state change. We
conceptualize the reason why the single action can
be achieved by the sequence as “a way of action
achievement”. The crucial point is detachment of
“what is achieved (state change caused by the
action)” and “how to achieve (way of action
achievement)”. This detachment of what to achieve
and how to achieve it reduces the number of actions
to be defined, which allows us to define a small set
of actions as a controlled vocabulary. When two or
more ways can be applied to achieve an action, those
ways are in an OR relationship. A way of action
achievement explains the necessary conditions to be
applied and a reason why the way is applicable.
The ontology of actions defines an action as a
state change of an object. The state change
represents only “what is achieved” and excludes
“how it is achieved”. This definition enables us to
detach a way of action achievement from an action.
The ontology also provides terms to be used in a
CHARM tree. The controlled terms are used as
verbs in a CHARM tree and combined with an
object (a target thing) to represent a concrete action
clearly.
Figure 1 shows a CHARM tree that represents
actions for emptying the digestive tract of a patient
before a surgical operation on a digestive organ.
This goal is described as an action “decrease
contents of digestive tract” as the top node of the
CHARM tree (node number 1 in Figure 1). This
node 1 action can be achieved by a sequence of the
Figure 1: A partial CHARM tree for decreasing contents
of digestive tract.
Decrease
contentsof
digestivetract
Egestthe
contentsof
digestivetract
frompatient’s
body
Promoting
egestionway
Egestthe
digestive
content
patient
Placeenema
solutionin
thepatient’s
body
Decrease
dietaryintake
Prohibiting
ingestionway
Decrease
dietary
intake
patient
…
doctor
Givemeal
skipping
orderto
patient
enemaway
…
Concentration=50%
Volume=60ml
1
2
3
4
5
6
8
AND
OR
:AddedAction
:Prescription
:Nutrition
Legends
:Wayofaction
achievement
Timepoint=pre‐operation
onJanuary8th
Timepoint=January8th
Doer
Attributeof
anaction
7
CHARMingClinicalPathways-ModelingofClinicalPathwaysbasedontheGoal-OrientedOntologicalFramework
CHARM
213
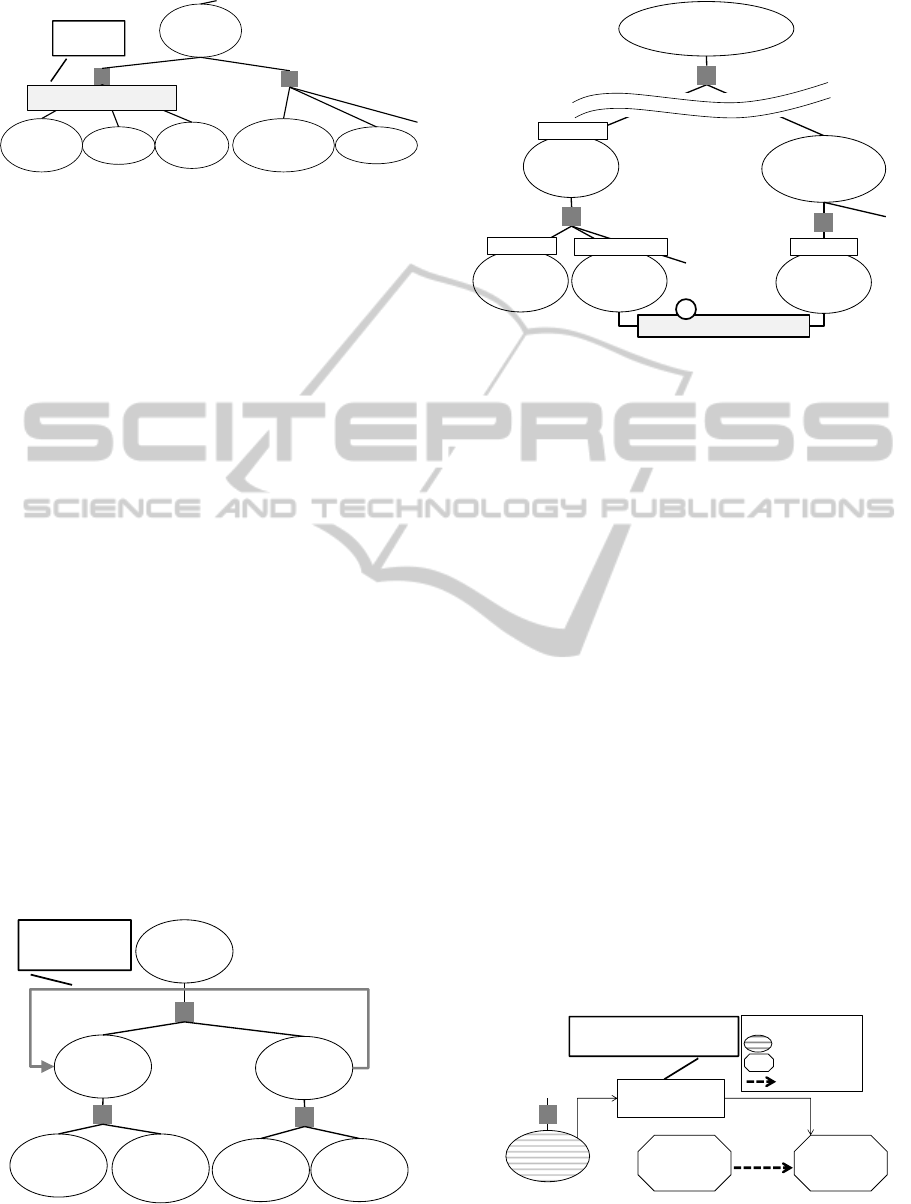
Figure 2: Representation of constrain in a CHARM tree.
actions described in nodes 2 and 3 in Figure 1. Node
1 represents a goal to be achieved by nodes 2 and 3.
Node 1 is called the whole action, whereas nodes 2
and 3 are called sub-actions. Furthermore, action 2
can be achieved by using the promoting egestion
way (node 4). The promoting egestion way explains
that an enema solution helps the body egest the
contents of the digestive tract as a reason why the
way can achieve the goal. A CHARM tree also
represents attributes of actions. For example, the
concentration of the enema solution is 50% and its
volume is 60 ml, as shown in part 6 of Figure 1.
Time points of actions, such as “pre-operation on
January 8th” are also represented as attributes of
actions as shown in part 7 of Figure 1.
The constraints about (conditions for adopting) a
specific way of action achievement can be also
represented with the node of the way of actin
achievement. For example, the head-tilt-chin-lift
way for moving tongue root must not be applied to
the patient whose cervical cord is injured. In Figure
2, the rectangle node under the way node denotes
this constraint. The constraints about actions are also
represented in the same form.
A complex order of actions can be also
represented in a CHARM tree. First, we explain how
to represent the repetition of actions. Figure 3 shows
a part of CHARM tree about chest compression.
When s/he compresses a patient’s chest, s/he needs
Figure 3: Representation of repetition in a CHARM tree.
Figure 4: Representation of parallel actions in a CHARM
tree.
to repeat 30 times pushing and recoiling the chest as
one cycle. In order to represent the repetition, there
is a link between the action node “contract the heart”
and the action node “expand the heart”. The link
denotes that the action “contract the heart” should be
performed if the actions are not performed less than
30 times. Second, a CHARM tree can also
represents medical procedures which are performed
in parallel by the link. In Figure 4, a CHARM tree
denotes a procedure of clinical staff after
anaphylactic shock occurred. The clinical staff
receives the emergency call gather and the nurse,
who stands by the patient stops dripping infusion
which causes anaphylactic shock in parallel. The
parallel sequence is represented by the link between
the actions as shown in part 1 of Figure 4. The link
denotes that the action “move to the site of the
patient” and the action “stop dripping the infusion”
are performed in parallel.
A CHARM tree can also represent a relationship
between actions and side effects. As shown in Figure
5, the “assessing nausea” action is for assessing the
side effect of anticancer agents. This relation is
represented as a link and clarifies the reason why a
member of the medical staff assesses nausea.
Figure 5: Representation of relationship between action
and side effect.
Movetongue
root
Openmouth
Move
chinup
Maketwohand
contacttothe
mandible
Head‐tilt‐chin‐liftway
Jawthrust
maneuverway
Constraint
oftheway
Gentlymove
headtoback
Movetongue
root
Constraint:Patientstate
≠cervicalcordinjury
Movethe
bloodtothe
brain
Makethe
pressureforce
existenton
thechest
Expandthe
heart
Contractthe
heart
Recoilthe
chest
Chestcompressionway
Makehands
contactto
thechest
Repetitionconstraint:
Lessthan30times
Decrease
thepressure
force
Thelinkdenotes
therepetitionof
actions.
Changethepatient’s
statebetterfrom
anaphylacticshock
...
Canbeperformedinparallel
1
Transmitthe
informationto
clinicalstaff
NurseA
Movetothe
siteofthe
patient
Clinicalstaff
Makeclinical
staffcloserto
thepatient
NurseA
Decreasethe
causativeagentof
anaphylactic
shock
Stopdripping
theinfusion
NurseA
Nausea
Assess
nausea
Chemotherapypathway
…
Activationof
vomitingcenter
byanticancer
agent
Assess
thesideeffect
:Test
:Sideeffect
:Causalrelation
Legend
Thelinkdenotesthe
relationbetweenan
actionandasideeffect
HEALTHINF2014-InternationalConferenceonHealthInformatics
214
The features of CHARM trees can be summarized as
follows.
1) A controlled vocabulary representing actions is
clearly defined and makes the meanings of actions
clear.
2) CHARM trees can make the goals of actions
explicit.
3) CHARM trees can clarify the reason why the way
is applied and make it easy to compare alternative
ways of action achievement.
The first feature is based on the ontology of
actions. The ontology includes controlled action
terms. The controlled terms define the meanings of
actions and thus help us compare actions. The
second feature is making the goals of actions
explicit. The whole action is interpreted as the goal
of the action. The relationship between an action and
other effects also explains why the action is
performed. The third feature is based on a way of
action achievement. Alternative ways of action
achievement may exist, and several ways are shown
under the whole action node. This makes it easy to
compare the ways. The way of action achievement
explains the reason why sub-actions can achieve the
goal, so as to make it clear why the way is applied.
This feature helps us understand alternative ways
and compare CPs easily.
2.2 Clinical Pathway (CP)
A CP represents a standard sequence of actions
carried out by doctors, nurses, and other clinical
staff members for each disease, and the timing at
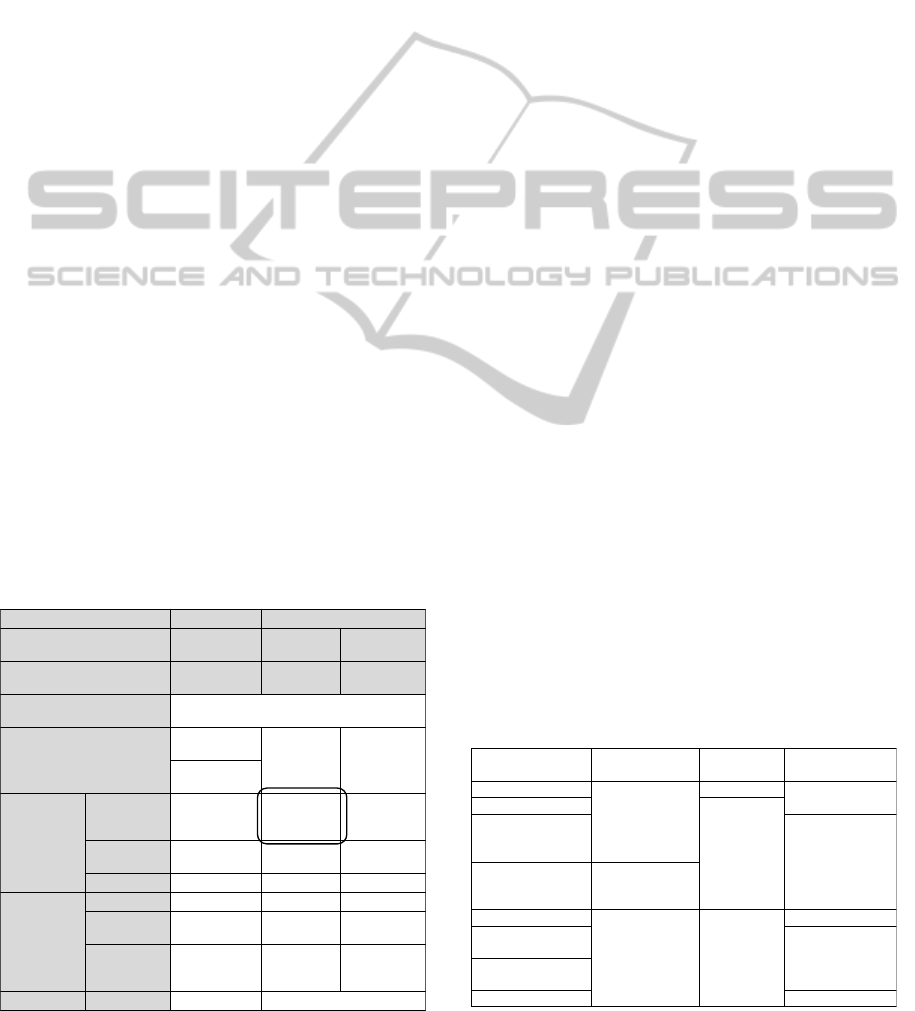
which the actions should be performed. Basically,
Table 1: A portion of the Hepatectomy CP.
CPs are represented in a tabular form. The horizontal
axis is a time scale, and the vertical axis is the kind
of action (Coffey et al., 2005). The CP methodology
is widely deployed in hospitals to minimize delays
and excessive resource-consumption and to maintain
the quality of care.
Table 1 shows a portion of the Hepatectomy CP,
which is used in Osaka University Hospital. A single
action is described in a cell, and this CP contains all
treatment actions performed in a ward during
hospitalization. The date is shown in the uppermost
row of the table, and actions described in the same
column are performed on the same day. Outcome
describes the goal of the event, and this goal is
necessary before the next event can be performed.
This represents the order relationship between
events. Furthermore, kinds of actions are shown on
the left side of the table. This indicates that actions
in the same row belong to the same kind.
2.3 Target CPs to Be Described
In this research, we described eight real CPs used in
Osaka University Hospital in CHARM trees, as
shown in Table 2. These CPs represent treatments
for cancer during hospitalization. As shown in Table
2, CPs are created in three departments, such as the
digestive surgery department. There are three kinds
of affected organs, such as the liver in the case of the
Hepatectomy CP. Ways of removing the affected
part are also different. We confirmed the
representation capability of CHARM through the
description of various CPs with medical doctors.
We built eight CHARM trees based on those
eight CPs as knowledge sources. Each CHARM tree
consists of about 360 action nodes on average.
Among them, about 100 actions are explicitly
described in the source CPs. The rest (about 260) of
the nodes were added as the goals of actions that are
implicit in the source CPs, when we built the
Table 2: CPs to be described based on CHARM.
Date January 7th January8th
Unit name
Previous dayof
operation
Pre‐operation Post‐operation
Eventname
Previous dayof
operation
Operation Operation
Hospitalization/Ambulatory
treatment
Hospitalization
Outcome
Ready forthe
operation
Nosignsof
infection
disease
No
complications
Nosignsof
infectiondisease
Treatment
Prescription Magcorol P(50g)
Kenei G
enema50%
60ml
Injection
DIVSoldem 3A
500ml
DIVSoldem
3A500ml
IVH1Soldem
3A500ml
General
Test /
Examination
Laboratorytest Hematologictest
Pathological
examination
Imaging/Physio
logical test
While
operation,
ChestX‐ray
Nutrition Morning Skipmeal
NameofCP
Hospital
department
Affectedorgan
Removal wayof
affectedpart
Gastrectomy
Digestivesurgery
Stomach
Excision
Hepatectomy
Liver
Transcatheter arterial
chemoembolization
(insurgeryward)
Chemoembolization
Transcatheter arterial
chemoembolization
(inmedicalward)
Gastroenterological
medicine
Chemotherapy
Gynecologic Uterus
Chemotherapy
Laparotomy for
malignantdisease
Excision
Laparotomy for
benigndisease
Radiotherapy Radiation
CHARMingClinicalPathways-ModelingofClinicalPathwaysbasedontheGoal-OrientedOntologicalFramework
CHARM
215
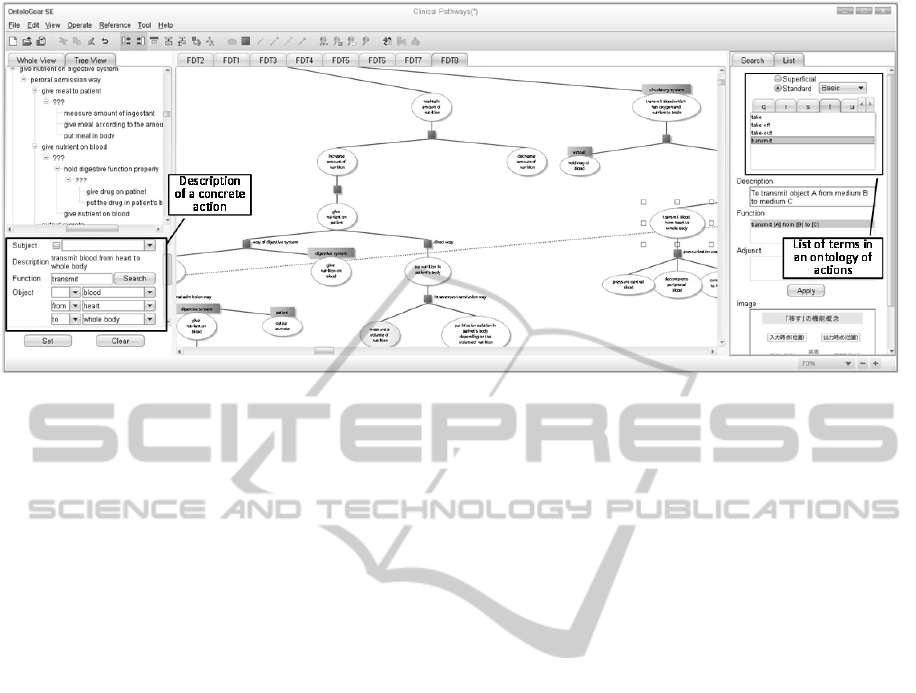
Figure 6: Screen shot of OntoloGear.
CHARM trees.
The CHARM trees were modeled using
OntoloGear (as shown in Figure 6), editing software
collaboratively developed by MetaMoJi Co. and the
authors (MetaMoJi Co., 2009) based on a functional
knowledge sharing framework (Kitamura and
Mizoguchi, 2003). As shown at the lower left in
Figure 6, an action is constructed from a transitive
verb and objects. The verb term is controlled in the
ontology of actions and a list of the terms is shown
at the right side of Figure 6. We can represent an
action using the terms. Thanks to the functionality of
OntoloGear, the CHARM tree data is stored in a
computer interpretable form. In the next sub-section,
we describe in detail how to model a CP based on
CHARM.
2.4 Building CHARM Trees from CPs
2.4.1 Building Process of CHARM Trees
This section explains how we built CHARM trees
from CPs. A team which consists of knowledge
engineers and medical doctors built the CHARM
trees. First, an action in each cell of each CP was
modeled as an action node of a CHARM tree. For
example, a cell “Kenei G enema 50% 60ml” appears
in the center of Table 1, as shown. We interpreted
this cell as an action of placing enema solution in the
patient’s body using the enema way shown as node 5
in Figure 1. The concentration and the volume of the
enema solution were also described. Moreover, the
kind of action was denoted by color (shaded parts in
Figure 1).
Second, we added the whole actions (goals) of
the actions written in the CP. We added these goal
actions by consulting a doctor because they were not
described in the CP. An added action is denoted by a
white node. For example, we described action 2 in
Figure 1, which is to cause the digestive contents to
be egested from patient’s body, as the goal of action
5 in Figure 1.
Third, we decomposed the goal action into sub-
actions. We checked whether the whole (goal) action
node represents the same state change as sub-actions
do. If not, we added the missing action nodes. For
example, we added action 3 in Figure 1. Action 3 is
to decrease dietary intake and is necessary for
achieving the goal action, which is to decrease the
contents of the digestive tract in the patient’s body.
Action 3 was added because the CP does not
represent how to achieve its goal. Action 8 in Figure
1, which is for achieving action 3, exists in the
source CP, and therefore, action 8 was linked to
action 3.
We repeated this process for each cell in the
source CP.
In addition, we described side effects related to
the actions in a CP, as shown in Figure 5. For
example, an action that assesses nausea is described
in the CP, and the action is performed to detect a
side effect of an anticancer agent. This side effect
was not described in the CP. We extracted them
from explanation documents given to patients in
Osaka University Hospital. The documents contain
only typical side effects, so we described only
typical side effects in the CHARM trees.
HEALTHINF2014-InternationalConferenceonHealthInformatics
216

2.4.2 Building an Upper-level Goal
Achievement Hierarchy of CHARM
Trees
Actions described in CPs are performed during
hospitalization. We interpreted the top-goal of the
actions as “changing a (diseased or injured) state of
a patient to a state in which the patient can leave the
hospital”. We identified the actions 1 to 5 in Figure
7 through considering what actions are necessary for
achieving this goal. Action 1, “maintain daily
activity”, includes a patient’s daily actions or actions
taken by staff to support patients, such as taking a
meal or cleaning a patient’s body. Action 2, “change
the state of the patient to a ready state in preparation
for the main treatment” indicates an action taken to
prepare the patient for the main treatment, such as a
surgical operation. For example, the action for
assessing a patient, such as measurement of body
temperature, in the sub-actions of action 2 is needed
to achieve the goal of recording basic data about the
patient before the operation. Action 3 “change the
state of the affected part to a treated state” indicates
a main action of treatment such as a surgical
operation and drug administration. An action related
to the main treatment is also necessary for achieving
this goal. For example, an action that measures the
body weight to determine the dose of an anticancer
agent achieves action 3. Action 4, “maintain health
condition in acute stage”, indicates an action to
maintain the patient’s state against the side effect of
the main treatment. Compared with the same
“assessing” sub-action of action 2 described above,
the assessing sub-actions of action 4 is needed to
achieve the goal of finding a variance from the
normal value. That is, the CHARM tree represents a
difference of the goals to be achieved by the same
action. Action 5, “change the state of the patient to a
state in which s/he can live after being discharged
from the hospital” indicates an action for living after
being discharged from the hospital, such as living
guidance and mental care.
Figure 7: Top section of CHARM tree.
These actions discussed above are not described in
CPs. These actions are interpreted as the top-level
goals of the actions described in CPs and are made
explicit based on CHARM. Explication of such top-
level goals differentiates the goals of the same
actions, such as the measuring actions above, from a
goal-oriented perspective.
We confirmed that CHARM is applicable to
model the contents of CPs by building CHARM
trees based on real CPs. These CHARM trees have
been approved by the co-authors who are medical
doctors. We have also confirmed the benefits of
CHARM trees, as discussed in the next section.
3 BENEFITS OF CHARM
3.1 Identifying Commonality of
Actions in CPs
As a result of modeling the eight CPs based on
CHARM, we confirmed that the upper-level goals of
the actions in the CPs have commonalities, as
discussed in Section 2.4.2. This suggests that actions
in CPs have a common goal. We also identified the
commonality shown below.
・Actions for keeping homeostasis
Actions for keeping homeostasis are described in
CPs. For example, the circulatory system of the
patient's body acts to keep homeostasis. A patient
with a failing of circulatory system must receive
assistance. Figure 8 shows a partial CHARM tree for
assisting the function of the circulatory system. The
tree clarifies which action assists what. In this
example, the use a stocking way (point 1) achieves
Figure 8: A partial CHARM tree for assisting the function
of circulatory system.
Maintain
dailyactivity
Changethestate
ofthepatienttoa
readystatein
preparationforthe
maintreatment
Changeastateof
patienttoastate
whichthepatientcan
leavethehospital
Changethestate
ofthepatienttoastate
whichs/hecanliveafter
beingdischargedfrom
thehospital
Changethe
stateofthe
affectedpartto
atreatedstate
Maintainhealth
conditionin
acutestage
Wayofdecreasing
theaffectedpart
Wayofmaking
thestateback
…
Drugadministrationway
…
Surgical operationway
…
Decreasethe
affectedpart
1
2
3
4
5
Transmit
bloodto
brain
Holdwayof
blood
Gettheblood
flowing
Transmitblood
fromheartto
wholebody
Transmitblood
fromwhole
bodytoheart
PressurizationwayPressurizationway
…
…
Decreasethe
pressureof
centralblood
Usingstockingway
Increasethe
pressureof
peripheral
blood
Increase
blood‐flow
…
1
Commonpartsof
medicalprocedures
CHARMingClinicalPathways-ModelingofClinicalPathwaysbasedontheGoal-OrientedOntologicalFramework
CHARM
217
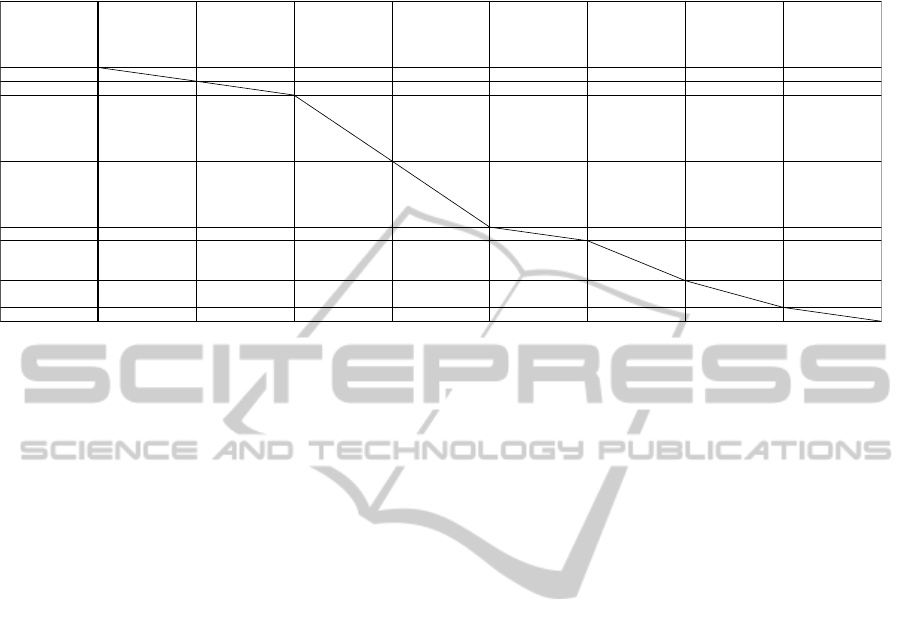
Table 3: A list of pairs of CPs that we compared (X in the cell denotes that the combination is finished to compare. Number
in parenthesis denotes distances.).
an action that increases the pressure of the peripheral
blood vessels, whose overall goal is to transmit
blood to brain. We consider that these actions (as
shown in dotted line in Figure 8) will appear in other
medical procedures because the actions for keeping
homeostasis are not uncommon in medicine.
Actually, such actions appear in all eight CPs.
However, it would take a lot of time to describe
all actions related to keeping homeostasis because
this would be equivalent to describing all functions
of the human body. In this study, we described only
actions related to the actions in the CPs, and we
found that these were enough for representing
actions performed during hospitalization.
3.2 Comparison of CPs using CHARM
Trees
CHARM trees explicate the knowledge implicit in
CPs. We compared CPs using CHARM trees in
order to confirm the benefits of CHARM.
Table 3 shows pairs of CPs that we compared. In
the uppermost row of the table and the left side of
the table, the name of CP is shown. X in a cell
shows that the comparison between CPs, whose
names are shown in the uppermost row and the left
side column, was finished. The number in
parenthesis is the number of differences of actions in
the CPs. We compared CPs in which treatments
were different and which were created by different
departments. We calculated the distances
(differences) of the action nodes in the CHARM
trees using TED (Tree Edit Distance) (Zhang and
Shasha, 1989), and these are shown in parentheses in
Table 3. TED is a method of describing the distance
(difference) between tree-structured data and
represents the cost of editing operations that
transform one tree into another. The editing
operations are renaming, deleting, and inserting.
From the results of the comparison, the CHARM
trees explain the reason why there are differences in
CPs. Moreover, it is easier to find some differences
than with a comparison based on CPs because the
goal and the relation of actions can be clarified
based on CHARM. The following sub-sections
explain such benefits using real examples.
3.2.1 Difference between Ways to Achieve
the Same Goal
The goal of actions is described as the whole action
node, and the way of action achievement is clearly
represented in a CHARM tree. When there are a
number of ways to achieve the same goal, these
ways are placed under the whole action node and are
linked with it. It is not easy to understand whether or
not the goals of actions in CPs are the same based on
CPs. CHARM trees help us compare actions because
CHARM clarifies the goal of actions. Figure 9
shows that a partial CHARM tree represents the
difference between ways to achieve the same goal
when we compare Hepatectomy CP and
Gastrectomy CP.
In order to achieve the same goal of giving
nutrition to blood (as shown in 1 of Figure 9), the
intravenous transfusion way (as shown in 2 of
Figure 9) is applied in the Hepatectomy CP, whereas
the intravenous hyper alimentation way (as shown in
Gastrectomy Hepatectomy
Transcatheter
arterial
chemoemboli‐
zation (insurgery
ward)
Transcatheter
arterial
chemoemboli‐
zation (in
medicalward)
Chemotherapy
Laparotomyfor
malignant
disease
Laparotomyfor
benigndisease
Radiotherapy
Gastrectomy
X(35)
Hepatectomy
X X(127) X(158) X(168) X(122)
Transcatheter
arterial
chemoemboli‐
zation (insurgery
ward)
X X(112)
Transcatheter
arterial
chemoemboli‐
zation (in
medicalward)
XX
Chemotherapy
X X(75)
Laparotomyfor
malignant
disease
X X(139)
Laparotomyfor
benigndisease
X X(176)
Radiotherapy
XX
Notes:
1.X;finishedtocomparetheCPs
2.(number);distancesoftheactionnodesintheCHARMtrees
HEALTHINF2014-InternationalConferenceonHealthInformatics
218
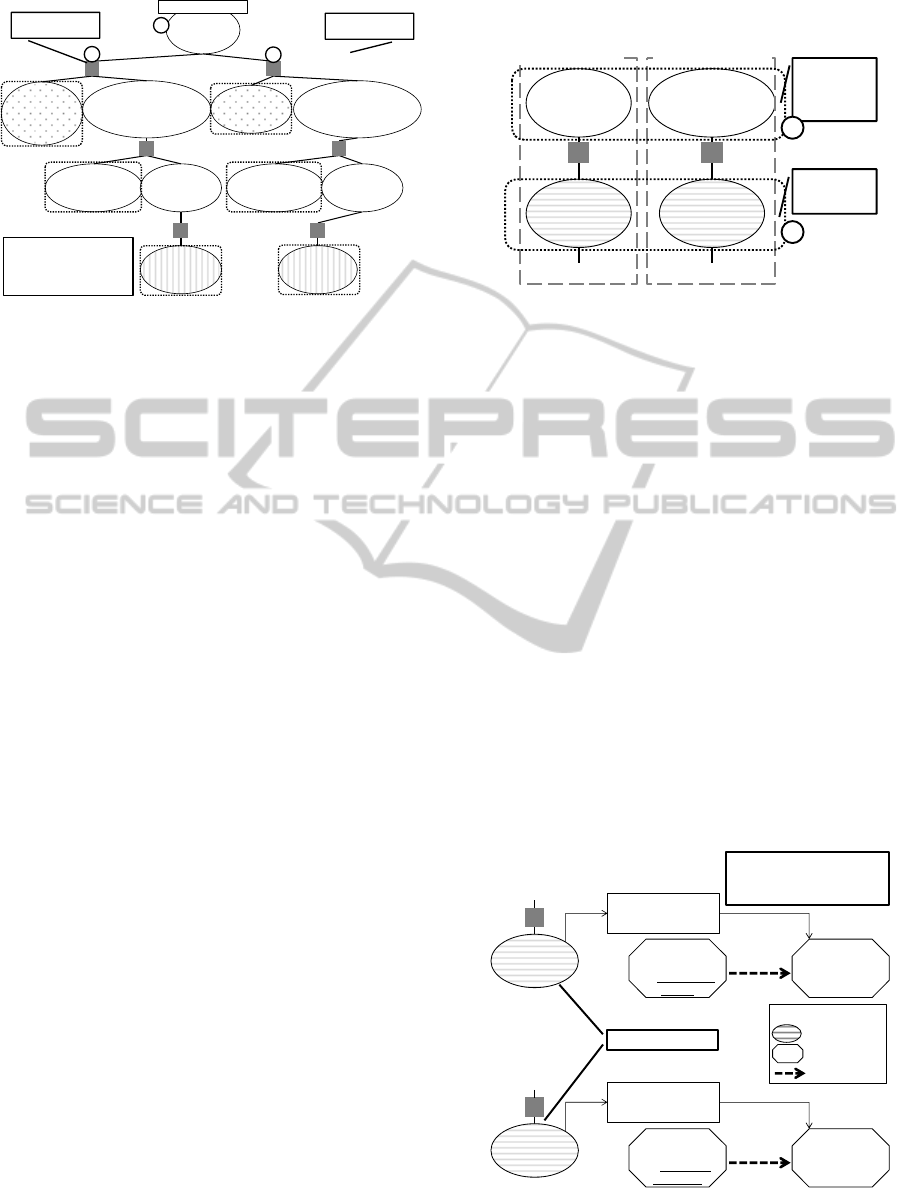
Figure 9: Difference between ways to achieve the same
goal based on CHARM tree.
3 of Figure 9) is applied in the Gastrectomy CP.
Both way 2 and way 3 in Figure 9 achieve action 1.
The action “estimating the required nutrition” and
the action “putting infusion solution in the body” are
described separately in the CPs. It is not easy to
understand the reason why estimating actions are
different from each other. Since we built CHARM
trees, we could compare the actions from a goal-
oriented perspective and understand that the
difference between these CPs is the difference of
ways of action achievement.
A medical doctor who is one of the co-authors of
this paper considers that there is no medical
justification for this difference, and that the selection
of the ways seems to be done based on only
convention. This suggests that there is room to
discuss the justification for the selection of the ways
of action achievement, and CHARM trees can help
us in this point.
3.2.2 Difference of Goals to Be Achieved by
the Same Action
The same action in CPs might achieve different
goals. Here, we give an example in a comparison
between the Transcatheter arterial
chemoembolization CP and the Chemotherapy CP.
Both CPs contain the “assessing numbness” action
(as shown in part 1of Figure 10). A comparison
using the CHARM trees of these CPs helps us
understand the difference of the goals. As shown in
Figure 10, the shaded nodes denote similar actions in
different CPs, but goals (as shown in part 2 of Figure
10) of these actions are different. The goals that are
implicit in the CPs are made explicit in the CHARM
trees. Furthermore, when one revises a CP, the
explicitness of the goals of the actions helps him/her
understand the intention of the author of the original
version.
Figure 10: Difference of goals to be achieved by the same
action based on CHARM trees.
3.2.3 Difference of Side Effects Related
to the Same Action
The same action in CPs might have different reasons
why the action should be done. Figure 11 shows an
example in a comparison between the Chemotherapy
CP and the Radiotherapy CP. Both CPs contain the
same “assessing nausea” action. These actions,
however, have different side effects related to them.
In chemotherapy, a patient may feel nausea as a side
effect of an anticancer agent. In radiotherapy, a
patient may feel nausea as a side effect of radiation
exposure. Each assessing action in the CPs is done
in order to detect one of these side effects. The
ability of CHARM to clarify the relationship
between actions and side effects helps us understand
this difference.
In addition to the differences discussed thus far,
we found some other differences, such as differences
of both the goal and the performed actions. CHARM
Figure 11: Difference of side effects related to the same
action based on CHARM trees.
Estimatethe
volumeof
peripheral
parenteral
nutrition
Putinfusionsolution
inpatient’sbody
dependingonthe
volumeofnutrition
Makewayfrom
skintoperipheral
veinexistent
Putinfusion
solutionin
patient’sbody
UsingSolyugen way
PutSolyugen F
inpatient’s
body
Givenutrition
toblood
digestivesystem
Intravenoustransfusionway
Infusionway
Estimatethe
volumeof
centralvenous
nutrition
Putinfusionsolution
inpatient’sbody
dependingonthe
volumeofnutrition
Makewayfrom
skintocentralvein
existent
Putinfusion
solutionin
patient’sbody
UsingSoldem way
PutSoldem 3A
inpatient’s
body
Intravenoushyper
alimentationway
Infusionway
1
2
3
From
Hepatectomy CP
From
Gastrectomy CP
Note:
Nodesinrectanglewith
dottedlinedenote
differencesbetween
theCPs.
Assessfunction
ofnervous
system
Assess
numbness
…
Assess
inhibitionof
bloodflow
Assess
numbnessof
stabside
…
Different
part
between
theCPs
Similar
actionsin
theCPs
Transcatheter arterial
chemoembolization
CP
ChemotherapyCP
2
1
Nausea
Assess
nausea
RadiotherapyCP
…
Activationof
vomitingcenter
byradiation
exposure
Assess
thesideeffect
Test
sideeffect
Causalrelation
Legend
Nausea
Assess
nausea
ChemotherapyCP
…
Activationof
vomitingcenter
byanticancer
agent
Assess
thesideeffect
Thesameactions
Note:
UnderlinedtextinItalic
formdenotesadifferent
partbetweentheCPs.
CHARMingClinicalPathways-ModelingofClinicalPathwaysbasedontheGoal-OrientedOntologicalFramework
CHARM
219

trees can help us find not only superficial differences
of actions in CPs, but also implicit differences, such
as differences of the goals and relationships.
4 RELATED WORK
A number of groups have been developing computer
interpretable guideline model, such as Asbru (Shahar
et al., 1998), PROforma (Sutton and Fox, 2003),
GLIF (Boxwala et al., 2004), and SAGE (Tu et al.,
2007). They aim to develop guideline-based point-
of-care decision support systems. The systems make
alerts and reminders to assist doctors in making
decisions by automatic reasoning based on computer
interpretable models in the flowchart-style form. As
discussed in Introduction, we aim at supporting not
point-of-care decision by medical staff but
knowledge description and revision by the
knowledge managers. For such knowledge
management, our model has some benefits discussed
thus far. In the flowchart models used in the
guideline models above, the temporal order of
actions is mainly described and the goals of actions
are in many cases implicit. Externalizing the implicit
knowledge, such as goals can facilitate revision of
procedures. CP authors can easily detect the point to
revise in a CP.
Hurley et al. have developed a CP ontology in
order to represent actions in CPs in a computer
interpretable way (Hurley and Abidi, 2007). Hu et al.
have also developed a CP ontology and proposed a
system connected with a conventional EMR
(Electronic Medical Record) system (Hu et al.,
2012). Hurley et al. have identified concepts and
attributes that appear in CPs and developed a CP
ontology. They have confirmed the representation
capability by describing five real CPs based on this
ontology. Their ontology is specialized for CPs,
which are time-sequence-oriented way. Thus, their
models based on the ontology are structured in the
same way as CPs, that is, time-oriented. On the other
hand, our study is based on an ontology of general
actions, which is goal-oriented. Thus, our CHARM
tree clarifies explicit knowledge, such as goals and
relations of actions, which are implicit in CPs. Since
our ontology is not specialized for CPs, CHARM
can describe medical actions extracted from other
knowledge sources, such as clinical practice
guidelines and nursing manuals, and can thus handle
them seamlessly.
Abidi et al. represented CPs in a computer
interpretable way and integrated CPs derived from
different institutions (Abidi et al., 2009). They
identified the commonalities of three different CPs
based on the CP ontology and integrated them into
one flowchart. The integrated flowchart can be
specialized for each region of the institution. On the
other hand, in our study, we identified not
differences of regions but differences of goals and
the way of action achievement. Abidi et al. claim
that their model is convenient for the revision
management of CPs. After revision of the common
parts of the integrated flowchart that represents CPs,
they specialize the flowchart to a CP for each region,
and then the revision is reflected. On the other hand,
a CHARM tree also helps us manage knowledge.
When a conventional treatment method is abolished
and a new method is applied, we need only delete
the corresponding way of action achievement and
add a new one from a goal-oriented perspective. The
goals explicitly described in a CHARM tree help us
add new knowledge to appropriate parts of the tree.
5 CONCLUSIONS
The work described in paper shows the practical
ability of CHARM to describe medical actions in
eight real CPs in a computer interpretable way. The
built CHARM trees clearly represent knowledge that
is implicit in conventional CPs, such as goals of
actions and the ways of action achievement. The
benefits of CHARM trees include: (1) finding
commonalities among CPs, (2) allowing easy
comparison of CPs from a goal-oriented perspective,
and (3) explaining the reasons for the differences.
We face the following challenges in achieving
the ultimate goal, which is to manage procedural
knowledge about medical practice based on a unified
management framework.
Currently, the controlled vocabulary for actions
treats physical actions only. Since medical actions
affect human beings, mental health treatment is also
important. The definitions of mental actions and
their treatment will be tackled in future work.
A CP represents a typical sequence of medical
actions for each disease. On the other hand, some
treatments consist of an atypical sequence of actions.
Treatment may be different at the acute stage and the
chronic stage, such as the treatment of cardiac
failure. Moreover, the timing of switching the way
of treatment is different for each patient. Therefore,
it is not easy to create a CP for such treatment. We
will try to describe such treatment based on
CHARM. Because CHARM is a goal-oriented
representation, we expect that such treatments can
be modeled successfully.
HEALTHINF2014-InternationalConferenceonHealthInformatics
220

CPs and clinical practice guidelines describe
standard (prescriptive) actions, unlike the record of
real actions performed on a patient, which is
descriptive. We will develop a method of describing
patient records based on CHARM to manage the
entire knowledge of actions in hospitals.
REFERENCES
Abidi, S. R., Abidi, S. S. R., Hussain, S., and Butler, L.
(2009). Operationalizing Prostate Cancer Clinical
Pathways: An Ontological Model to Computerize,
Merge and Execute Institution-Specific Clinical
Pathways. Knowledge Management for Health Care
Procedures, Lecture Notes in Computer Science,
5626: 1-12.
Boxwala, A. A., Peleg, M., Tu, S., Ogunyemi, O., Zeng, Q.
T., Wang, D., Patel, V. L., Greenes, R. A., and
Shortliffe, E. H. (2004). GLIF3: a representation
format for sharable computer-interpretable clinical
practice guidelines. Journal of Biomedical Informatics,
37: 147-161.
Coffey, R. J., Richards, J. S., Remmert, C. S., LeRoy, S. S.,
Schoville, R. R., and Baldwin, P. J.,(2005). An
Introduction to Critical Paths. Quality Management in
Health Care, 14(1): 46-55.
Every, N. R., Hochman, J., Becker, R., Kopecky, S., and
Cannon, C. P. (2000). Critical Pathways: A Review,
Circulation, 101: 461-465.
Hauck, L. D., Adler, L. M., and Mulla, Z. D. (2004),
Clinical pathway care improves outcomes among
patients hospitalized for community-acquired
pneumonia, Annals of Epidemiology, 14(9): 669-675.
Hu, Z., Li, J. S., Zhou, T. S., Yu H. Y., Suzuki, M., and
Araki, K. (2012). Ontology-Based Clinical Pathways
with Semantic Rules. Journal of Medical Systems,
36(4): 2203-2212.
Hurley, K. F., and Abidi, S. S. R. (2007). Ontology
Engineering to Modelo Clinical Pathways: Towards
the Computerization and Execution of Clinical
Pathways. 20th IEEE International Symposium on
Computer-Based Medical Systems, 536-541.
Kitamura, Y., and Mizoguchi, R. (2003). Ontology-based
description of functional design knowledge and its use
in a functional way server. Expert Systems with
Applications. 24(2): 153-166.
Nishimura, S., Kitamura, Y., Sasajima, M., Williamson,
A., Kinoshita, C., Hirao, A., Hattori, K., Mizoguchi, R.
(2013). CHARM as Activity Model to Share
Knowledge and Transmit Procedural Knowledge and
its Application to Nursing Guidelines Integration.
Journal of Advanced Computational Intelligence and
Intelligent Informatics, 17(2): 208-220.
Madan, A. K., Speck, K. E., Ternovits, C. A., and
Tichansky, D. S. (2006). Outcome of a clinical
pathway for discharge within 48 hours after
laparoscopic gastric bypass. The American Journal of
Surgery, 192(3): 399-402.
MetaMoJi Co. (2009). http://metamoji.com/en/
Pearson, S. D., Goulart-Fisher, D., and Lee, T. H. (1995),
Critical Pathways as a Strategy for Improving Care:
Problems and Potential. Annals Internal Medicine,
123(12): 941-948.
Mizoguchi, R., Tutorial on ontological engineering - Part
1, 2, 3. (2003), (2004), (2004). New Generation
Computing, 21(4): 365-384, 22(1): 61-96, 22(2): 193-
220.
Sasajima, M., Nishimura, S., Kitamura, Y., Hirao, A.,
Hattori, K., Nakamura, A., Takahashi, H., Takaoka, Y.,
and Mizoguchi R. (2013). CHARM Pad: Ontology-
Based Tool for Learning Systematic Knowledge about
Nursing. Proceedings of HCI International 2013
,
pages 560-567 ISBN 978-3-642-39252-8.
Shahar, Y., Miksch, S., and Johnson P. (1998). The
Asgaard Project: A Task-Specific Framework for the
Application and Critiquing of Time-Oriented Clinical
Guidelines. Artificial Intelligence in Medicine, 14(1-
2): 29-51.
Sutton D. R., and Fox, J. (2003). The Syntax and
Semantics of the PROforma Guideline Modeling
Language. Journal of the American Medical
Informatics Association, 10(5): 433-443.
Tu, S. W., Campbell, J. R., Glasgow, J., Nyaman, M. A.,
McClure, R., McClay, J., Parker, C., Hrabak, K. M.,
Berg, D., Weida, T., Mansfield, J. G., and Musen, M.
A. (2007). The SAGE Guideline Model:
Achievements and Overview, Journal of the American
Medical Informatics Association, 14(5): 589-598.
Zander K., (1988). Nursing case management: strategic
management of cost and quality outcomes. The
Journal of Nursing Administration, 18(5): 23-30.
Zhang K., and Shasha, D. (1989). Simple Fast Algorithms
for the Editing Distance between Trees and Related
Problems. SIAM Journal on Computing, 18(6): 1245-
1262.
CHARMingClinicalPathways-ModelingofClinicalPathwaysbasedontheGoal-OrientedOntologicalFramework
CHARM
221
