
Stabilization of Endoscopic Videos using Camera Path from Global
Motion Vectors
Navya Amin, Thomas Gross, Marvin C. Offiah, Susanne Rosenthal, Nail El-Sourani
and Markus Borschbach
Competence Center Optimized Systems, University of Applied Sciences (FHDW),
Hauptstr. 2, 51465 Bergisch Gladbach, Germany
Keywords:
Medical Image Processing, Endoscopy, Global Motion Vectors, Local Motion Estimation, Image Segmenta-
tion, Video Stabilization.
Abstract:
Many algorithms for video stabilization have been proposed so far. However, not many digital video stabiliza-
tion procedures for endoscopic videos are discussed. Endoscopic videos contain immense shakes and distor-
tions as a result of some internal factors like body movements or secretion of body fluids as well as external
factors like manual handling of endoscopic devices, introduction of surgical devices into the body, luminance
changes etc.. The feature detection and tracking approaches that successfully stabilize the non-endoscopic
videos might not give similar results for the endoscopic videos due to the presence of these distortions. Our
focus of research includes developing a stabilization algorithm for such videos. This paper focusses on a spe-
cial motion estimation method which uses global motion vectors for tracking applied to different endoscopic
types (while taking into account the endoscopic region of interest). It presents a robust video processing
and stabilization technique that we have developed and the results of comparing it with the state-of-the-art
video stabilization tools. Also it discusses the problems specific to the endoscopic videos and the processing
techniques which were necessary for such videos unlike the real-world videos.
1 INTRODUCTION
Invasive diagnostics and therapy makes it necessary
for the surgeon or scientist to insert and move the
endoscopic devices within the inner parts of the hu-
man body. Based on the organ to be diagnosed, the
endoscopic procedure is classified as Bronchoscopy
(Daniels, 2009), Laryngoscopy (Koltai and Nixon,
1989), Gastroscopy, Laparoscopy (Koltai and Nixon,
1972), Rhinoscopy (University of Tennessee Col-
lege of Veterinary Medicine, 2012) and Colonoscopy.
Visualization of stable videos by physicians is very
essential during surgery. But the videos generated
during endoscopy are very distorted and shaky due
to the camera shakes occurring during insertion of
an endoscopic apparatus into the human body, the in-
ternal body movements (Breedveld, 2005) like heart-
beat, expansion and contraction of the organs as a
response to stimuli as well as secretion of body flu-
ids like saliva, mucus, blood etc. Miniaturization
of the endoscopic devices also adds to the distor-
tions. This makes it difficult for the surgeon to di-
agnose or operate. Hence, processing and stabiliza-
tion of such videos becomes necessary to overcome
such problems. Many mechanical video stabiliza-
tion systems are available for endoscopic video stabi-
lization commercially. These physical means of sta-
bilisation use either a gyroscope or some other self
stabilizing hardware device which holds the camera
(Chatenever et al., 2000). But the drawback is that
they are large, consume a lot of energy and are ex-
pensive. Another stabilzation system developed by
Canon also stabilizes before the video is converted
into digital data requiring larger and heavier cam-
era making it challenging for endoscopic cameras
(Canon, 1995). Digital video stabilization system is
a better, cheaper and compact alternative for the en-
doscopic purposes. Among the available state-of-the-
art digital video stabilization tools Adobe’s video sta-
bilization algorithm, which was subject to continu-
ous development in recent years, is one of the cur-
rent state-of-the-art stabilization algorithms. Adobe’s
algorithm is based on the well-known Kanade-Lucas-
Tomasi feature tracking (KLT) method, which detects
features in a start frame and tracks them over sev-
eral successive frames. The tracked feature point co-
130
Amin N., Gross T., C. Offiah M., Rosenthal S., El-Sourani N. and Borschbach M..
Stabilization of Endoscopic Videos using Camera Path from Global Motion Vectors.
DOI: 10.5220/0004688801300137
In Proceedings of the 9th International Conference on Computer Vision Theory and Applications (VISAPP-2014), pages 130-137
ISBN: 978-989-758-003-1
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

ordinates form the trajectory paths, which represent
the movements of a video camera. In the subsequent
step, these shake-prone trajectories are smoothed with
a smoothing method to get a shake-free video. The
algorithm includes additional steps that are described
in detail in the recent publications (Liu et al., 2011),
(Liu et al., 2009) and (Zhou et al., 2013). Another
similar method is illustrated in the algorithm which
is integrated into YouTube’s video editor and is also
based on the KLT tracking method (Grundmann et al.,
2011). The method is explained in detail in (Grund-
mann et al., 2012). Microsoft’s algorithm worked
in a slightly different way as follows (Matsushita
et al., 2005), (Matsushita et al., 2006). The motion
in the video is estimated by means of the Hierarchical
model-based block-motion algorithm. This approach
does not track the features across multiple frames to
get the trajectories, but the camera path is determined
from the movements from every consecutive frame.
These motion vectors are used to create a trajectory,
which approximate the original camera path and still
contains the unwanted camera shake. This path is
then smoothed to obtain a shake-free video. Detailed
descriptions are found in (Bergen et al., 1992).
Research has been carried out on how well cur-
rent state-of-the-art stabilization tools and algorithms
perform on endoscopic videos. Luo et al (Lu
´
o et al.,
2010) tested different feature detection algorithms on
bronchoscopic videos. Wang et al used their Adaptive
Scale Kernel Consensus Estimator to estimate better
motion model parameters (Wang et al., 2008). There
exist many video stabilization tools - commercial as
well as freeware. However, application of these tools
for stabilizing endoscopic videos proved to be ineffec-
tive: Related work still shows that even high-quality
stabilization tools like the Google’s video stabiliza-
tion algorithm by Grundmann et al. (Grundmann
et al., 2011) used in Youtube Video Editor and the
Adobe Systems algorithm by Liu et al. (Liu et al.,
2011) appeared to perform with moderate to unsatis-
factory results, although these are the best among a set
of state-of-the-art tools (Offiah et al., 2012c), (Offiah
et al., 2012a),(Offiah et al., 2012b).
2 STATEMENT OF PROBLEMS
The problems with the stabilization of endoscopic
videos are peculiar to the real world videos. In addi-
tion to the removal of high-frequency camera shakes
from normal videos, it is important that uneven cam-
era panning is aligned so that the output video looks
smooth to the viewer. High-frequency camera shakes
are also undesirable in endoscopic videos, but due
to the area of activity of an endoscope in the hu-
man body, sprawling camera movements always exist.
Also, in contrast to the real world video, endoscopic
recordings include usually no long video sequences,
but short scenes with quick image content changes.
Even small oscillating movements change the image
content to a large extent, because the image objects
are very close to the lens. Due to these circumstances
current state-of-the-art video stabilization algorithms
are not ideal for stabilizing endoscopic videos. No
long trajectories for endoscopic videos are available.
An algorithm has to be able to compensate the high-
frequency camera shake. To ensure a surgeon receives
a stable video, the removal of high-frequency shake is
the primary task of an endoscopic video stabilization
system. Involuntary movements, like movements of
body parts should not be removed whether the camera
is steady or navigating. The stabilization algorithm
by Microsoft deals with the stabilization of videos,
which determines the camera movements from frame-
to-frame. This approach is better suited for medical
videos. Adobe’s video stabilization uses the Content
Preserve Warp Technique and approximates the cam-
era movements with the information of the tracked
feature points. However, this algorithm has signifi-
cant difficulty in texture-less image regions. Only a
few traceable feature points are found to determine
an accurate approximation for the image distortion,
which can lead to a strong erroneous warp of the im-
age content. Erroneous deformation is completely in-
admissible in medical images and thus the algorithm
used by Adobe is not favourable for stabilizing endo-
scopic videos.
Fast movements occur very frequently in endo-
scopic videos. This is because the objects are lo-
cated close to the camera lens leading to a very fast
change of the image content as well as motion blur.
In such frames many feature points are lost and a va-
riety of trajectories break off abruptly for which the
tracker must be reinitialized. In comparison to the
test recordings of our laboratory, endoscopic videos
include much less image features, like edges or tex-
ture, resulting in a smaller number of detected feature
points. For this reason, long trajectories are normally
not detected in case of endoscopic videos. This is a
big disadvantage for an endoscopic stabilization al-
gorithm, in which a large number of long trajectories
for a clean stabilization is essentially required. The
tracker must therefore be re-initialized much more
frequently for a stabilized recording. Since the fea-
ture detection is the first and crucial step of video
stabilization, a maximum number of possible feature
points is required for a better image transformation
procedure. Multi-frame feature tracking approach to
StabilizationofEndoscopicVideosusingCameraPathfromGlobalMotionVectors
131
obtain long trajectories is used in the Adobe stabiliza-
tion algorithm. The long trajectories that such an al-
gorithm demands are not available in case of endo-
scopic videos. Thus, multi-frame feature tracking ap-
proach is not suitable endoscopic videos. Frame-to-
frame feature tracking as used in YouTube stabilizer
is the solution for this problem which has been used
in the current EndoStabf2f algorithm.
3 METHODS FOR VIDEO
STABILIZATION
The limitations of the previously proposed methods
for video stabilization and the designated problems
make it necessary to develop a new algorithm suited
for endoscopic videos. The videos are processed to
get rid of the meta-data, like text information in the
video frame and to determine the shape of the image
content if it has a circular, a polygon or a full frame
format (no black areas in the video frames). If the
video contains a circular output format or unwanted
text areas, then these regions are segmented and re-
moved prior to stabilization. These steps fall into the
area of image processing and significantly contribute
to a better video stabilization.
3.1 Image Preprocessing
Because of different endoscopic types, the quality and
output format of the video recordings are significantly
different. The endoscopic content in the videos can
be circular, rectangular or polygonal (Gershman and
Thomson, 2011). Furthermore, endoscopic videos
can not only contain image information but also ar-
eas with text. These are located either outside, dis-
played on the edge or within the video frame (Fig-
ure 2). The preprocessing step aims at achieving an
improved quality and information content of medical
images. This does not necessarily mean a visual im-
provement of the image material but an improvement
of the results with respect to subsequent processing
steps. For example, preprocessing enhances the qual-
ity of the videos to enable an improved and more ro-
bust feature detection in the frame. The following de-
scribes preprocessing steps which are included in our
video stabilization algorithm.
3.1.1 Segmentation of Undesirable Image
Regions
Some endoscopic videos contain meta-data like time
or year of capture or type of endoscopy inside the
video content. Text that appears in the video stays in
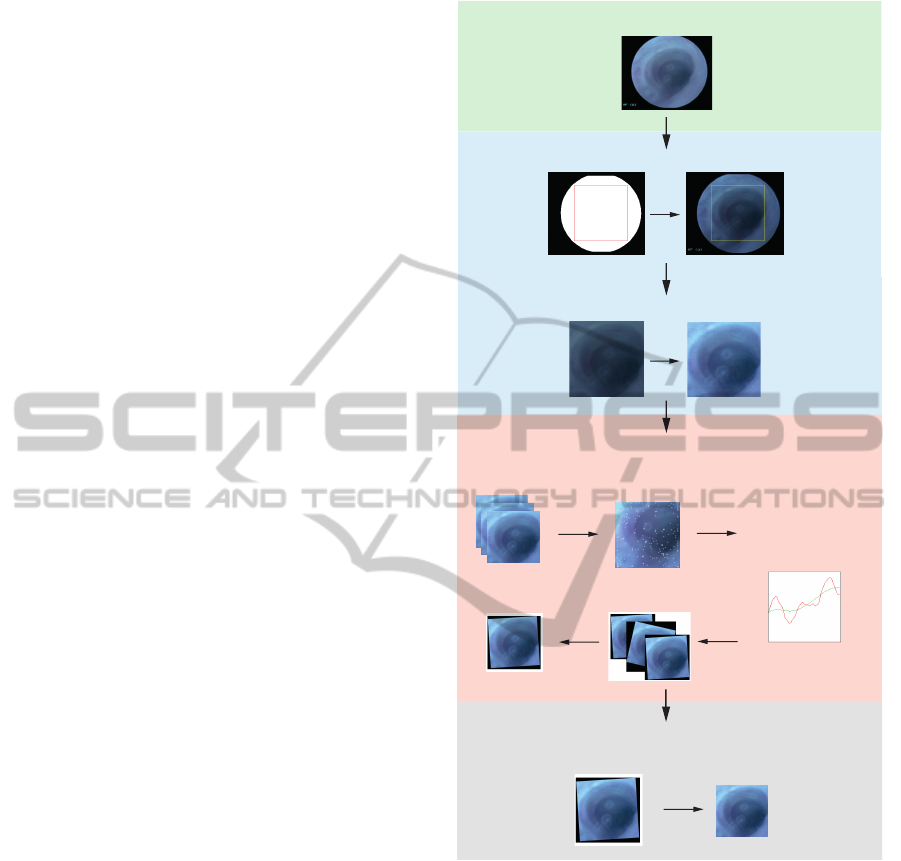
Original video
Preprocessing 1: Segmentation steps
Preprocessing 2: Image Enhancement
Video Stabilization Process
Frame 1 - n
1. ME: Feature Tracking &
Global Motion Estimation
2. Smoothing &
Motion Compensation
3. Image Composition
Stable Video
Optional: Additional Steps
Cut out black reagion
Figure 1: Video Stabilization workflow.
the same position throughout the video which could
be a disadvantage for a robust feature tracking. The
video in Figure 2 (Original Video Frame) contains
text information in the video frame. The strongest
features are detected only at this region in the video.
For this reason, a segmentation step is required to seg-
ment and remove the text information from the video
(See figure 2):
1. Create an averaged image from random video
frames. This serves as the input image for the bi-
nary mask. Many images are used randomly and
the image pixels of the video frame are averaged.
The areas containing endoscopic image informa-
tion are brighter. The dark black border around
VISAPP2014-InternationalConferenceonComputerVisionTheoryandApplications
132

the video image contains dark to black pixels and
hence is darker than the region containing endo-
scopic content. A better definition for creating the
binary mask is guaranteed.
2. Create a binary mask with chosen threshold.
3. Image processing steps: edge detection, dilation,
erode, segmentation and selection of the actual
endoscopic image content.
4. Reduce the size of the circular mask with x per-
cent to get a tolerance to the blurred edges of the
original video frame existing in some cases.
5. Optional: identification of the maximum square
area within the video screen for better feature de-
tection.
Finally, one gets a video frame mask showing only
the important medical image content. Surrounding
regions are excluded. Another algorithm was im-
plemented, which automatically finds the maximum
square area within the video frame. (See Figure 2).
3.1.2 Removal of Grid Distortions from
Fiberglass-endoscopic-videos
Another automated preprocessing step is the detec-
tion of pixel grids in the video. Videos recorded with
the fiberglass endoscopes, contain a clearly visible
image grid due to the distinctive design of the en-
doscope, that covers the entire video frame. These
highly prominent pixels of the image grid are often
detected as robust feature points. Similarly, with the
text information, these grid pixels always remain in
the same location in the video frame. A robust fea-
ture tracking is thus significantly affected. A prepro-
cessing step, using the Fourier transform, and addi-
tional image processing operations, remove the grid
from the endoscopic video.
3.2 Feature-based Motion Estimation
(ME Unit)
The movements of the endoscope are recorded us-
ing the KLT algorithm. But unlike the video stabi-
lization algorithm from Adobe and Google, this al-
gorithm does not use any anchor frames to track in-
dividual features over many frames to form feature
trajectories. Instead, the global and local motion of
the camera is determined only by successive frames,
using the KLT with our algorithm. Thus, the ME
unit determines the Global Motion Vectors (GMV)
between two adjacent frames of a video sequence.
From this frame-to-frame motion information a tra-
jectory is created, which represents the approximated
original camera path. This trajectory still contains the
undesirable camera shake. To compensate the shake,
a smoothing function is used to remove the jitters and
the irregular camera movement. The great advantage
of this method is that only two frames are needed to
determine the motion from one frame to another. For
example, in Adobe’s algorithm, 50 or more frames
are used to create a trajectory (Liu et al., 2011). As
seen in our experiments, such long trajectories do nor-
mally not appear in endoscopic videos. The crashing
of multi-frame feature tracking algorithm is described
in (Gross et al., 2014). The individual steps are de-
scribed in detail:
3.2.1 Global Motion Estimation
After the preprocessing is completed, the video stabi-
lization process begins. The first frame of the video is
read. This serves as the initialization frame for fea-
ture detection. The feature points are detected us-
ing the KLT method within the previously determined
video mask (ROI). The output represents the x/y co-
ordinates of the feature points (FPs) found. Next, the
FPs in the second frame are detected. The two sets of
feature points, each consisting of x and y coordinates
are compared, and only valid feature points (feature
point pairs) are used. Feature points which were not
found in the previous frame are discarded. The global
motion in the image is then calculated by subtracting
the feature coordinate values of the first frame from
the coordinate values of the second frame (only for
valid feature points). In each case, all detected FPs
coordinate values (separately for x and y) and motion
vectors are stored in a matrix. In the next step, the
second frame is used as the initialization frame and in
the third frame the FPs are tracked. These steps were
repeated until the entire video is processed. Always,
one frame serves as the initialization frame and the
adjacent frame serves as the tracking frame for mo-
tion estimation.
3.2.2 Local Motion Estimation
Sometimes local movements may appear in the video
which have nothing to do with the global camera mo-
tion. For example, such local movements are the re-
sult of the movement of the surgical devices. This
would affect the global motion estimation. Therefore,
these motions were explored in the second step and
were excluded from the calculation of the global mo-
tion. From all feature coordinates, a average global
mean value is calculated. This value represents the
average pixel difference of the current feature point
position and its position in the previous frame. From
the previously calculated motion vectors for each FP,
the Mean Absolute Deviation (MAD) (Sachs, 1984)
StabilizationofEndoscopicVideosusingCameraPathfromGlobalMotionVectors
133
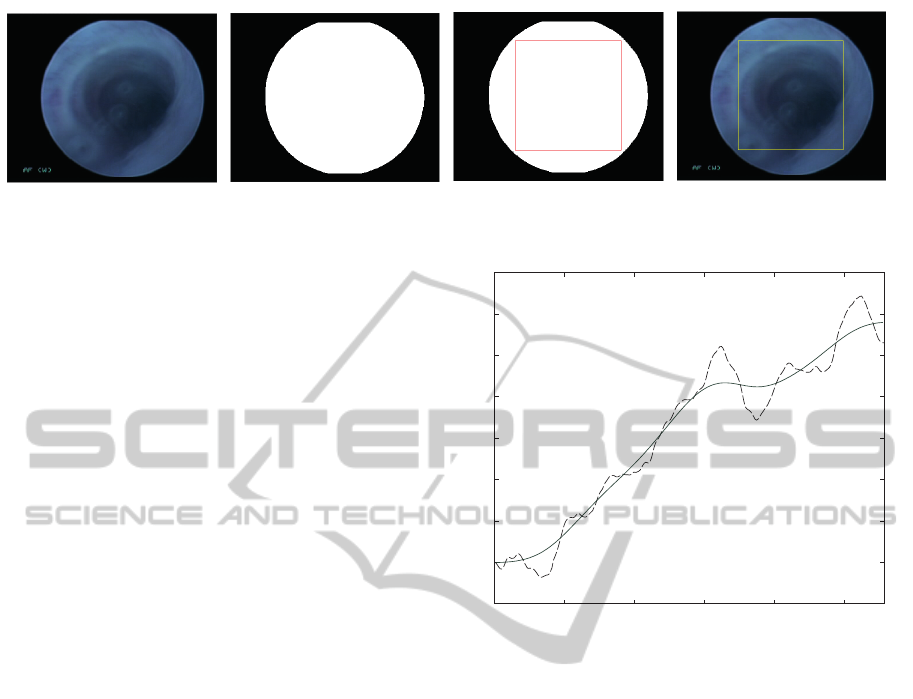
Figure 2: Segmentation workflow. Left: Original image frame. Second left: Video mask with unnecessary regions deleted.
Third left: Inscribed square region in the video mask. Right: ROI for feature tracking in the video.
is calculated. This indicates how much a FP moved
away from its previous location. This is calculated
separately for the x and y component of the motion
vectors. The values which differ in + / - the MAD
value from the mean of all x and y values are dis-
carded and not used for the subsequent calculation of
the global camera motion.
MAD = mean
i
|x
i
− mean
j
(x
j
)| (1)
3.2.3 Case Distinction
• If no FPs are found in the frames:
In some cases it may occur that no feature points
are detected, such as when individual frames con-
tain too few or texture-less regions. In this case,
global motion cannot be calculated and the global
motion of the frame is set to zero. To use the
original frame could be an unsatisfactory solu-
tion, since the path of the global movement is
interrupted and as a result, the frames begin to
jump. Hence, the motion vectors from the pre-
vious frame are used to avoid the jump.
• Creation of the camera path:
The determined and stored global motion vectors
are used to create the camera path which repre-
sents the movement in the video (see figure 3).
As seen, the curve is still very irregular. The
fine irregularities of the curve represent the high-
frequency camera shake in the video, which has
to be removed.
3.3 Smoothing
In the ME step all global motion vectors of the frames
are stored, and formed into a global camera path.
The task of the smoothing part is to determine a
smoother camera path curve to ensure a shake-free
video sequence. For smoothing the camera path,
a non-parametric kernel smoothing method with the
Nadaraya-Watson estimator is used to estimate an un-
known regression function (Cai, 2001). In figure 3,
0 50 100 150 200 250
−50
0
50
100
150
200
250
300
350
Figure 3: Motion trajectory extracted from a video. The
dashed line represents the shaky camera path, the smoothed
line the unshaky camera path.
the path of the global motion is shown in comparison
to the determined smoothed motion.
3.4 Motion Compensation and Image
Composition
To obtain a stabilized video, unwanted movements
were compensated by shifting the frames from the de-
tected feature point coordinate values obtained during
motion estimation to the the values determined in the
smoothing step (Figure 4). Further the existing black
regions as shown on figure 4 which are a result of the
frame-shifts are further removed to enable better and
clean visualization of the stable video. The black re-
gions are cropped out in case of rectangular videos.
In case of circular endoscopic videos, instead of the
extra black regions there exists a problem of jump-
ing circles as a result of the motion compensation. A
stabilized endoscopic video with jumping endoscopic
content is not good for visualization. Such videos
are further masked by calculating an average mask
across the whole video. A largest circle excluding the
jumping regions is calculated and the whole video is
masked using this mask. Many post-processing tech-
VISAPP2014-InternationalConferenceonComputerVisionTheoryandApplications
134

Figure 4: Motion compensated video frame.
niques for video stabilization are applied as per re-
quirements. In case of our endoscopic videos, harsh
cropping out of the black regions cause tremendous
loss of important information. Hence, the use of this
step completely depends on the user and the require-
ment.
4 EXPERIMENTS
We compare our stabilization algorithm (En-
doStabf2f) with Youtube (YT) and Adobe (AE). No
other digital stabilizers specifically for endoscopic
videos are available. Thus we used the best perform-
ing state-of-the-art digital stabilization tools for our
comparison experiments (Offiah et al., 2012a). For
this, 11 test videos are used:
1. Two real world videos containing forward and
backward movement of the camera.
2. Nine endoscopic videos containing different types
of endoscopic distortions.
Videos are labelled according to their types (see Ap-
pendix). Videos are cropped into different sections to
obtain sub-videos containing forward and backward
movement, steady scenes, distortions like bubbles,
foreground moving objects and circular endoscopic
videos trimmed into rectangular regions. Videos are
stabilized using frame-to-frame motion estimation us-
ing KLT tracker and compensated using perspective
transformation.
The black regions in the edges which are a result of
the compensation are cropped out in case of rectangu-
lar videos. The size of the black region to be cropped
is decided on the basis of the maximum shift cal-
culated for the x and the y axis. This trimming is
done so as to make the resultant stabilized videos us-
ing our algorithm comparable to the other two algo-
rithms. Youtube scales the videos to get rid of the
black regions in the stabilized video. Adobe pro-
vides an option to apply this cropping. The exisitng
black regions would affect the calculated PSNR val-
ues. Since the presence of black regions would af-
fect the benchmarking results, these black regions are
cropped out in both Adobe and our stabilization algo-
rithm. The stabilized videos are compared across the
2 stabilization algorithms using Inter-frame Transfor-
mation Fidelity where Inter-Frame Peak-Signal-To-
Noise-Ratio (PSNR) is calculted for every stabilized
video.
5 RESULTS AND DISCUSSION
The results of stabilization vary for different types of
videos used. The Endostabf2f algorithm is designed
specifically for endoscopic videos unlike YT and AD.
The stabilization by the YT stabilizer results in com-
pressed video resulting in loss of quality, automatic
region of interest selection and scaling leading to im-
mense probable loss of some important medical in-
formation. Also, no customization of the stabilization
procedure is possible as per user’s requirements. Un-
compressed, better quality video without any loss of
information is the prime necessity of medical endo-
scopic videos. Thus, YT would not be successful for
stabilizing endoscopic videos as per the requirements
of the physician. Endostabf2f successfully stabilizes
the endoscopic videos fulfilling the above mentioned
requirements. We further compared our Endostabf2f
with Adobe AE where customization of the stabiliza-
tion procedure as per requirements is possible. How-
ever, the results show that the performance of the sta-
bilization procedure is better for EndoStabf2f (see fig-
ure 5) when compared to Adobe AE stabilizer. The
videos used for benchmarking are preprocessed for
both the algorithms to enable the assessment of mo-
tion estimation and compensation. This results in bet-
ter PSNR values for AE. If the PSNR values are com-
pared without preprocessing, there is a possibility for
the values to be much lower due to the existing dis-
tortions like grid, moving circle etc. The PSNR val-
ues for the grid-removed bronchoscopic videos (g,h,l
and j) show that immense body movements in the
video affect the quality of video stabilization mak-
ing it worse. This is not in case of EndoStabf2f.
The real world video “Lab video 1” (f) which con-
tains forward and backward movements, is not well
stabilized by the AE algorithm resulting in a lower
PSNR value. On visualization, the shaky camera mo-
tion is not stabilized for a few frames. Similarly, in
case of other bronchoscopic and real world videos
(a,b,c,d and k) Endostabf2f gave better PSNR values
than AE. However, in case of the rhinoscopic video
with a steady camera (e) AE performed a bit better
StabilizationofEndoscopicVideosusingCameraPathfromGlobalMotionVectors
135

a b c d
e
f
g
h
I j k
Videos
PSNR values (in dB)
15 20 25 30 35
f2f AE
Figure 5: PSNR results for 11 videos.
than the Endostabf2f by 0.4 decibels approximately.
This might be because of the available long trajectory
for smoothening due to steady camera which usually
not frequently available in case of endoscopic videos.
Subjective assessment of the stabilized videos is re-
quired to affirm the quality of stabilized videos as re-
quired by the user. Videos stabilized by AE contain
jumps in the frame during scene change. This is ex-
treme in case of endoscopic videos since they con-
tain very frequent scene changes. Hence, visualiza-
tion of such videos misguides the surgeon prooving
to be dangerous. Our algorithm in contrast takes these
issues into account and is customized for the purpose
of endoscopic video stabilization.
There is scope for further optimization of the En-
doStabf2f algorithm with respect to motion estima-
tion using optimized algorithms which is a part of our
ongoing research. In addition, the image composition
part could be optimized to exclude the black regions
after compensation without losing too much of impor-
tant information.
ACKNOWLEDGEMENTS
This work as a part of the PENDOVISION-project is
funded by the German Federal Ministry of Education
and Research (BMBF) under the registration identi-
fication 17PNT019. The financial project organiza-
tion is directed by the Research Center J
¨
ulich. The
work was conducted under supervision of Markus
Borschbach.
REFERENCES
Bergen, J. R., Anandan, P., Hanna, K. J., and Hingorani, R.
(1992). Hierarchical model-based motion estimation.
In ECCV ’92 Proc. of the Second European Confer-
ence on Computer Vision, pages 237–252. Springer-
Verlag London, UK.
Breedveld, P. (2005). A new, easily miniaturized steerable
endoscope. IEEE Engineering in Medicine and Biol-
ogy Magazine, Volume 24:40–47.
Cai, Z. (2001). Weighted nadaraya-watson regression esti-
mation. In Statistics and Probability Letters, volume
Volume 51, pages 307–318.
Canon (1995). Optical image Stabilizer. Canon U.S.A. Inc.,
http://www.usa.canon.com/cusa/consumer/standard-
display/Lens Advantage IS, Accessed:November 5,
2013.
Chatenever, D., Mattsson-Boze, D., and Amling, M. R.
(August 1, 2000). Image orientation for endoscopic
video displays. U.S. Patent 6097423 A.
Daniels, R. (2009). Delmar’s Guide to Laboratory and Di-
agnostic Tests. Delmar - Thomson Learning.
Gershman, G. and Thomson, M. (2011). Practical Pediatric
Gastrointestinal Endoscopy (1st Edition). Wiley, John
& Sons, Incorporated.
Gross, T., Amin, N., Offiah, M. C., Rosenthal, S., El-
Sourani, N., and Borschbach, M. (2014). Optimiza-
tion of the endoscopic video stabilization algorithm
by local motion exclusion. In 9th International Joint
Conference on Computer Vision, Imaging and Com-
puter Graphics Theory and Applications, to appear.
Grundmann, M., Kwatra, V., Castro, D., and Essa, I. (2012).
Calibration-free rolling shutter removal. In Interna-
tional Conference on Computational Photography.
Grundmann, M., Kwatra, V., and Essa, I. (2011). Auto-
directed video stabilization with robust l1 optimal
camera paths. In IEEE Conference on Computer Vi-
sion and Pattern Recognition (CVPR).
Koltai, P. J. and Nixon, R. (1972). Laparoscopy-new instru-
ments for suturing and ligation. Fertility and Sterility,
Volume 23:274–277.
Koltai, P. J. and Nixon, R. (1989). The story of the laryn-
goscope. Ear, Nose, & Throat Journal 68, Volume
7:494–502.
Liu, F., Gleicher, M., Jin, H., and Agarwala, A. (2009).
Plane-based content-preservingwarps for video stabi-
lization. In SIGGRAPH 2009. ACM New York, NY,
USA.
Liu, F., Gleicher, M., Wang, J., Jin, H., and Agarwala, A.
(2011). Subspace video stabilization. ACM Transca-
tions on Graphics, Volume 30:1–10.
Lu
´
o, X., Feuerstein, M., Reichl, T., Kitasaka, T., and
Mori, K. (2010). An application driven comparison of
several feature extraction algorithms in bronchoscope
tracking during navigated bronchoscopy. In Proc. of
the 5th international conference on Medical imaging
and augmented reality, pages 475–484.
Matsushita, Y., Ofek, E., Tang, X., and Shum, H.-Y. (2005).
Full-frame video stabilization. In In Proc. Computer
Vision and Pattern Recognition, pages 50–57.
Matsushita, Y., Ofek, E., Tang, X., and Shum, H.-Y. (2006).
Full-frame video stabilization with motion inpainting.
Volume 28:1150–1163.
Offiah, M. C., Amin, N., Gross, T., El-Sourani, N., and
Borschbach, M. (2012a). An approach towards a full-
reference-based benchmarking for quality-optimized
endoscopic video stabilization systems. In ICVGIP
2012, page 65.
Offiah, M. C., Amin, N., Gross, T., El-Sourani, N., and
Borschbach, M. (2012b). On the ability of state-of-
VISAPP2014-InternationalConferenceonComputerVisionTheoryandApplications
136

the-art tools to stabilize medical endoscopic video se-
quences. In MedImage.
Offiah, M. C., Amin, N., Gross, T., El-Sourani, N., and
Borschbach, M. (2012c). Towards a benchmarking
framework for quality-optimized endoscopic video
stabilization. In ELMAR, Sep.,2012 Proceedings,
pages 23–26.
Sachs, L. (1984). Applied Statistics: A Handbook of Tech-
niques. New York: Springer-Verlag.
University of Tennessee College of Veterinary Medicine, R.
(2012). http://www.vet.utk.edu/clinical/sacs/. inter-
nal/mips/rhinoscopy.php.
Wang, H., Mirota, D., Ishii, M., and Hager, G. D. (2008).
Robust motion estimation and structure recovery from
endoscopic image sequences with an adaptive scale
kernel consensus estimator. In CVPR.
Zhou, Z., Jin, H., and Ma, Y. (2013). Content-preserving
warps for 3d video stabilization. In IEEE Conference
on Computer Vision and Pattern Recognition.
APPENDIX
Table 1: List of the videos used for stabilization.
Video Description
a Bronchoscopic staboptic video of a rat with circular content
b Bronchoscopic staboptic video of a rat with rectangular content and moving camera
c Shaky video of a hippo
d Human Rhinoscopic 2 with rectangular content and steady camera
e Human Rhinoscopic 3 with rectangular content and steady camera
f Lab video 1 with forward and backward movement
g Bronchoscopic grid removed fibreoptic video of a rat with steady camera
h Bronchoscopic grid removed fibreoptic video of a rat with moving camera and distortion (Bubbles)
l Bronchoscopic grid removed fibreoptic video of a rat with forward-backward movement of camera
j Bronchoscopic grid removed fibreoptic video of a rat with rectangular content and steady camera
k Shaky video of a tiger with jittery motion
StabilizationofEndoscopicVideosusingCameraPathfromGlobalMotionVectors
137
