
Off-the-Person Electrocardiography
Hugo Pl
´
acido da Silva
1
, Carlos Carreiras
1
, Andr
´
e Lourenc¸o
1,2
and Ana Fred
1
1
IT - Instituto de Telecomunicac¸
˜
oes, Av. Rovisco Pais, 1, 1049-001 Lisboa, Portugal
2
ISEL - Instituto Superior de Engenharia de Lisboa, R. Cons. Em
´
ıdio Navarro, 1, 1959-007 Lisboa, Portugal
Keywords:
Electrocardiography, Off-the-Person, Taxonomy, Instrumentation, Experimental Evaluation.
Abstract:
Electrocardiography (ECG) methods are still mostly bound to hospital and short-time data acquisition settings.
Still, a paradigm shift is emerging, in which everyday technology is increasingly capable of measuring ECG
signals in a more pervasive manner. This is paving the way for systems that can better analyze and adapt to
perceived changes in the health status or behavior of the user. In this paper we present a taxonomy for the
intrusiveness of ECG data acquisition systems, describe a sensor design for what we call the ”off-the-person”
approach, and provide a discussion of the main challenges posed by these new methodologies. Our work is
targeted at pervasive electrocardiography through signal acquisition at the hand palms or fingers, by providing
a simplified sensor setup that can be integrated into virtually any object with which the person interacts with.
Experimental results show that data acquired using our proposed approach is highly correlated with data
obtained through conventional methods.
1 INTRODUCTION
The first practical implementation of what we known
today as Electrocardiography (ECG) appeared around
1887 and is credited to Augustus Waller, a British
physiologist that was able to record the electrical ac-
tivity of the human heart using non-invasive meth-
ods, and provided the first known systematic ap-
proach to the study of the electrical properties of
the heart (Besterman and Creese, 1979). Questions
surrounding the clinical applicability of the signals
and limitations of the measurement instrumentation
used at the time made the ECG have a slow start.
It was not until 1906 that a more widespread accep-
tance and use occurred. The groundbreaking work by
Willem Einthoven provided significant advances both
in terms of the measurement methods and signal char-
acterization, enabling the ECG to be more clearly un-
derstood. His work was recognized in 1924 through
the Nobel Prize in Medicine, several years after the
initial experimentations in the field (Barold, 2003).
Nowadays, the ECG is a perfectly established and
mainstream technique, and it provides vital informa-
tion for the diagnosis and observation of a wide array
of complex cardiovascular problems that include ar-
rhythmias, myocardial ischemia, prolonged QT inter-
val, among many others (Drew et al., 2004)(Chung,
2000). Most importantly, early detection of changes
in the cardiac patterns is crucial to anticipate severe
and long lasting problems, and to develop preven-
tive clinical interventions. Standard clinical prac-
tices are still based on short-term ECG data; the most
widespread approach is the 12-lead ECG for momen-
tary assessment in a clinical setting (∼ 1 minute of
data), and in selected cases, Holter monitors are used
for ∼ 24 hour assessment in an ambulatory setting.
In this paper, we present a taxonomy for the intru-
siveness of ECG data acquisition methods, together
with an off-the-person sensor design targeted at data
acquisition in a pervasive framework. Our work was
not devised with the purpose of replacing existing
data acquisition procedures. Instead, our goal is to
complement current practices with a simplified sen-
sor setup that can be introduced in multiple aspects of
the everyday life of patients or even of healthy sub-
jects, as a way of enabling a more comprehensive as-
sessment of cardiovascular parameters, and potenti-
ating preventive interventions. The rest of the paper
is organized as follows: Section 2 describes a taxon-
omy for the intrusiveness of ECG data acquisition ap-
proaches; Section 3 describes our off-the-person sen-
sor approach, highlighting the main technical options;
Section 4 provides an experimental comparison be-
tween the off-the-person approach and medical-grade
equipment; and finally, Section 5 outlines the main
conclusions.
99
Plácido da Silva H., Carreiras C., Lourenço A. and Fred A..
Off-the-Person Electrocardiography.
DOI: 10.5220/0004647700990106
In Proceedings of the International Congress on Cardiovascular Technologies (IWoPE-2013), pages 99-106
ISBN: 978-989-8565-78-5
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

2 A TAXONOMY FOR ECG DATA
ACQ. INTRUSIVENESS
Given the bioelectrical nature of the cardiac activ-
ity, the voltage potential differential is the most com-
monly used ECG measurement principle. Still, other
approaches can be used to sense the cardiac activity,
such as capacitive and mechanical methods. Despite
the underlying operating principle, several devices
have emerged over the years, that enable ECG signal
acquisition, and which we have classified according
to the intrusiveness level of the hardware setup with
respect to its placement on the body of the user. Fig-
ure 1 shows an overview of our taxonomy.
2.1 In-the-Person
Devices is this category are placed inside the body
of the person, and are generally used only in extreme
clinical scenarios to monitor or address medical con-
ditions. The devices are surgically placed inside the
body with measurement leads attached directly to the
heart, enabling the continuous monitoring of its be-
havior and the delivery of electrical impulses when-
ever a deviation from a normal cardiac pattern is de-
tected. Nowadays, most devices enable the exter-
nal access and remote monitoring of basic parameters
both by clinicians and patients.
One class of devices are the Implantable systems,
of which artificial cardiac pacemakers are the most
widely known example; these are used to compensate
for shortcomings of the electrical conduction system
of the heart, due to degenerative or pathological con-
ditions (Timperley et al., 2008). Modern implantable
devices can have extremely compact and lightweight
form factors, an example of which is the HD-X11 sys-
tem from Data Sciences International
1
, with 2.2 g and
a volume of just 1.4 cm
3
.
Another class of devices can be defined as Min-
imally Invasive, which includes implantable loop
recorders (ILR); albeit being placed inside the body
of the person, these are only applied subcutaneously,
through a simple medical procedure that typically
only requires local anesthesia, and enable the contin-
uous recording of the cardiac activity.
2.2 On-the-Person
The most common approaches to ECG measurement
used nowadays work by attaching a device, or some
of its components, externally to the body surface.
1
http://www.datasci.com/products/implantable-telemetry
Currently, devices designed to be used in an on-
the-subject approach are perfectly commoditized, and
range from medical-grade equipment to personal use
and self-monitoring devices for heart rate assessment
in sports and wellbeing activities (e.g. Polar Wear-
Link+
2
).
Standard ECG devices can be classified as Sta-
tionary systems. Devices in this category are typi-
cally characterized by workbench and bedside mon-
itors for medical use, and require the placement of
12 or more leads mounted on the chest and limbs, al-
though configurations with a lower number of leads
can also be found. Other properties of these devices
include the fact that they generally need conductive
paste or gel to lower the skin impedance, and that the
patient is bound to a limited physical space.
New developments in signal acquisition technolo-
gies greatly improved the usability, and enable more
practical approaches that fall into the class of Am-
bulatory systems. In the clinical domain, Holter
monitors are used for ambulatory cardiac assessment.
These are devices in which less measurement leads
are used, and a partial recording of the activity of
the heart is made in an internal memory, typically
over the course of 24 hours. Recently, there has also
been an increasing interest in integrating ambulatory
ECG sensing into portable devices, as shown by the
EPI Life ”Doctor in Your Pocket”
3
, claimed to be
the first ECG-enabled mobile phone, and also by the
AliveCor
4
monitor, proposed as a clinical diagnosis
tool, and which enables real-time ECG measurement
on the iPhone/iPad when the subject places the acces-
sory on the chest.
Within ambulatory systems, a vast amount of
work has been done around t-shirt and other wearable
form factors, such as the VitalJacket from BioDevices
5
. Another smart t-shirt is evaluated in (de Isla et al.,
2011), in which the measurement leads are embedded
into the fabric as a way of achieving a more practical
acquisition setup. In (Chi et al., 2010), the authors
present a comprehensive review of capacitive sensor
technologies that can be applied to a chest strap or
t-shirt to monitor the cardiac activity. A wearable
device designed as a necklace is described in (Silva
et al., 2011b), which uses dry Ag/AgCl electrodes and
enables heart rate measurement on the user’s neck.
2
http://www.polar.com/en
3
http://epimhealth.com.sg
4
http://www.alivecor.com
5
http://www.biodevices.pt
CARDIOTECHNIX2013-InternationalCongressonCardiovascularTechnologies
100
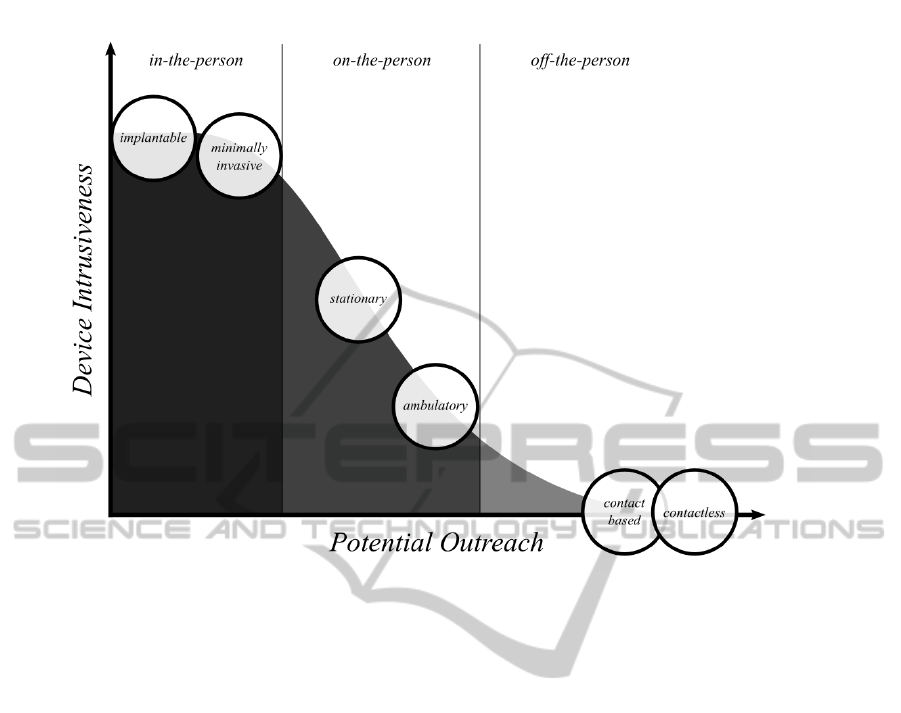
Figure 1: Overview of the intrusiveness and potential outreach of ECG data acquisition systems.
2.3 Off-the-Person
One of the challenges that has recently started to be
more prominently addressed in the state-of-the-art, is
the improvement of the sensor acceptability into what
can be defined as an off-the-person approach, given
that the sensors are integrated in objects with which
the subject regularly interacts with. The rationale be-
hind this approach is that, unlike the on-the-person
methods, in which the user needs to wear the sensor
or perform a voluntary action to have the sensor in
contact with his body, in this case the sensor is inte-
grated in a pervasive manner, so that the user does not
need to change his/her normal interaction patterns.
Within this trend, one of the categories comprises
Contact Based systems. An example can be found
in previous work by our team (Silva et al., 2011a),
where a bipolar sensor with virtual ground and dry
electrodes was proposed for ECG data acquisition at
the hand palms or fingers. The main advantage is that
these methods can be easily integrated into everyday
items without impacting on the user’s routines. Ap-
plications for such devices include ECG monitoring
while the person is working at a computer keyboard,
holding a game station controller, the steering wheel
of a car, and many others items, enabling its use in
a pervasive electrocardiography framework, and pro-
moting novel long-term monitoring paradigms.
The off-the-person approaches also comprise
Contactless systems; this class includes capacitive
and mechanical methods, which albeit not being ca-
pable of measuring the tradicional ECG signal, mea-
sure an ECG-like activity. Capacitive sensors mea-
sure the small time-varying electric fields associated
with the bioelectric activity of the heart (Chi et al.,
2010)(Martins et al., 2011). These sensors do not re-
quire direct contact with the body of the user, and can
be designed to measure the ECG at distances of ∼ 1
cm or more, even with clothing in-between the body
and the sensor, enabling its integration in the back
of a chair, in a car seat, or other analogous items.
Mechanical sensors measure heart-related events by
sensing the small vibrations propagated to the body
surface after the contraction of the cardiac muscula-
ture. This technique is known as ballistocardiogra-
phy or seismocardiography, and current approaches
are based either on accelerometers or electromechan-
ical films (Postolache et al., 2010).
These novel approaches are aligned with the lat-
est trends in medical applications of technology. As
Eric Topol states in his book (Topol, 2012), the fu-
ture of healthcare will inevitably lie on the infiltra-
tion of medical devices into our daily lives, collecting
more data about the human being over longer periods
of time, and reasoning about these large volumes of
data. This is the very essence of pervasive health.
Off-the-PersonElectrocardiography
101
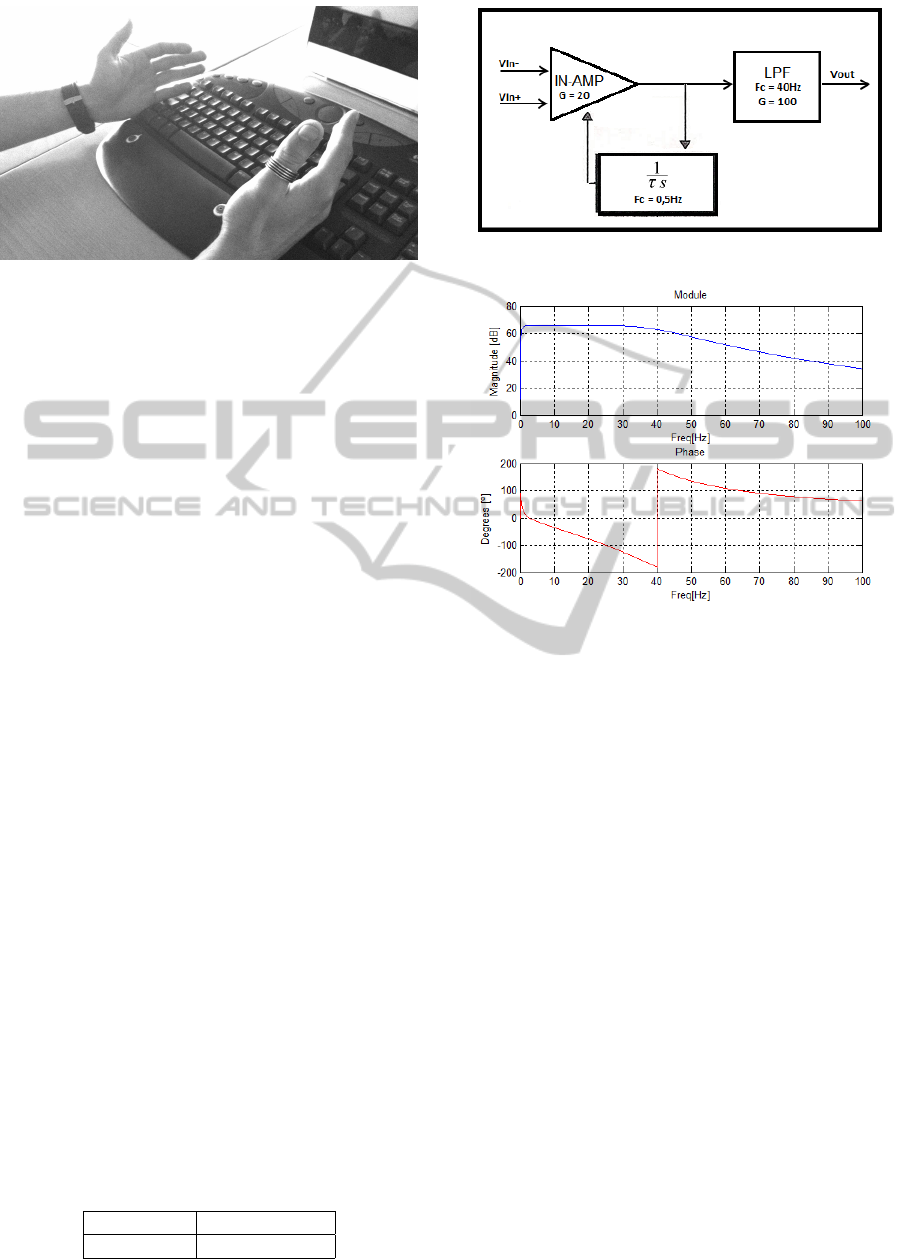
Figure 2: Contact based off-the-person sensor integrated in
a standard computer keyboard.
3 A CONTACT BASED SENSOR
FOR OFF-THE-PERSON ECG
In our work, we have been focusing on minimizing
the number of electrical contact points with the sub-
ject’s body, eliminating the need of any gel or con-
ductive paste in the interface with the skin, and devis-
ing a non-intrusive sensor system. Figure 2 shows an
example of our sensor integrated in a computer key-
board. Our tests have shown that even when com-
pared with conventional approaches in which pre-
gelled electrodes are used, this configuration provides
an output signal with adequate quality both with dry
Ag/AgCl or conductive textile electrodes, and no skin
preparation in either case.
3.1 Sensor Design
We developed analog signal conditioning circuitry
adapted to the ECG in terms of gain and bandwidth
(Malmivuo and Plonsey, 1995). Our design is single-
ended and is based on the classical voltage poten-
tial differential principle, one singularity being the
fact that the typical ground electrode is replaced by
a reference voltage produced by the circuit (generally
referred to as the ”virtual ground”). Table 1 shows
the typical physiological specifications for ECG sig-
nals (Webster, 2009); to measure the low potential
differences associated with these signals (in the mV
range), our sensor design includes a precision instru-
mentation amplifier (In-Amp) offering high common-
mode rejection (110 dB at gains greater or equal than
10). Furthermore, we use low-noise high speed op-
erational amplifiers (Op-Amp) to perform bandpass
filtering and amplification.
Table 1: Specifications of the ECG.
Range Frequency
0.5 − 4 mV 0.01 − 250 Hz
Figure 3: Block diagram of the ECG sensor design.
Figure 4: Frequency response of the ECG sensor block.
A block diagram of the circuit is shown in Fig-
ure 3. The use of dry electrodes introduces a higher
impedance and is more prone to high frequency noise;
as such, our design uses a gain of 2000 and a band-
width between 0.5-40 Hz. We have a first amplifica-
tion stage that uses an instrumentation amplifier with
gain 20, to measure the weak voltage potential differ-
ences produced by the cardiac activity and increase
their amplitude. Afterwards, an active 1st order high-
pass filter (Gain = 1; Cutoff = 0.5 Hz) is applied in or-
der to minimize the impact of low frequencies; in par-
ticular to remove modulation introduced by the res-
piratory activity. Finally, we use a 4th order Butter-
worth low-pass filter (Gain = 100; Cutoff = 40 Hz), to
limit the bandwidth of the signal to a range that dis-
cards the powerline noise, and to further increase the
amplitude of the signal in order to obtain higher def-
inition in the digital domain. The frequency response
of the sensor is presented in Figure 4.
Although our sensor was specifically designed
for 1-lead differential measurement at the fingers or
hands (left / right) with virtual ground, it can also be
used in standard chest or limb locations, with the op-
tion to use a ground lead as well. Equation 1 shows
the transfer function for this sensor (V
ss
denotes the
reference voltage).
CARDIOTECHNIX2013-InternationalCongressonCardiovascularTechnologies
102
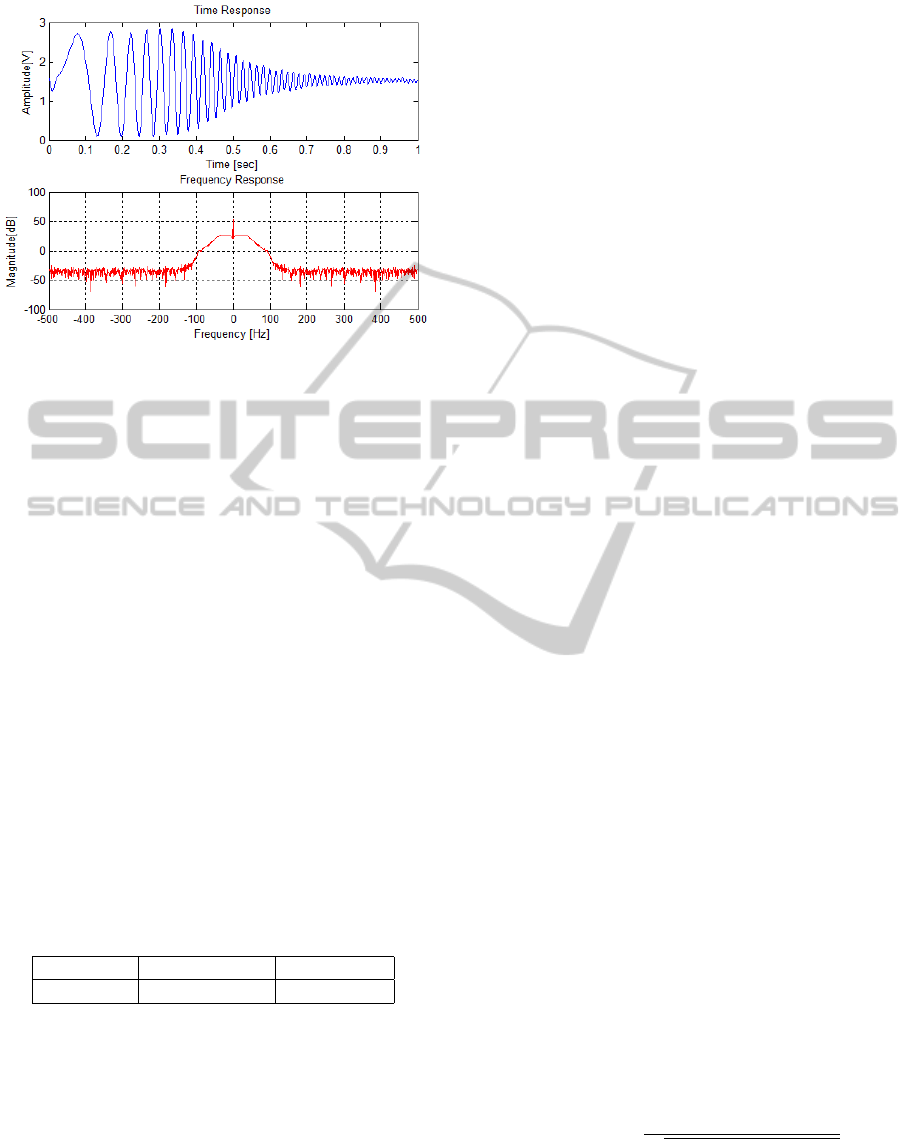
Figure 5: Time and frequency response of the ECG sensor
to the chirp signal.
V
Out
= (V
In+
−V
In−
) × 2000 +V
ss
(1)
3.2 Experimental Characterization
Tests were performed to characterize the quality of
the analog front-end in terms of Signal-to-Noise
Ratio (SNR), Signal-to-Noise Ratio plus Distortion
(SINAD), and Total Harmonic Distortion (THD). In
all experimental tests, the signals were generated us-
ing an Agilent 33220A function generator, and ac-
quired using an analog-to-digital converter (ADC)
with 10-bit resolution, a sampling rate of 1000 Hz,
and a 3.3 V peak-to-peak dynamic range (V
pp
) (Guer-
reiro et al., 2013). The function generator used in our
experiments is not able to accurately generate wave-
forms in the near-millivolt range, and as such, to char-
acterize the real response of the analog circuit, we re-
duced its gain to 100 (Gain = 1 at the In-Amp), ensur-
ing an output signal between 0 −3.3 V , that is, within
the dynamic range of the ADC.
Table 2: Dynamic specifications.
SNR [dB] SINAD [dBc] THD [dBc]
44.54 42.49 -46.74
For this test we injected a synthesized chirp wave
spanning the 0 −100 Hz frequency range, with 1 sec-
ond duration, 28 mV peak-to-peak, and offset of V
cc
/2
(V
cc
being the supply voltage). Figure 5 shows the fre-
quency response of our ECG circuit; as shown in the
top figure, the output signal of the circuit is a chirp
wave with ≈ 2.8 V peak-to-peak (V
pp
) and with at-
tenuation in the low and high frequencies, a natural
response of the bandpass filter that we have used. To
characterize the dynamic specifications of the circuits,
we used a synthesized sine wave with a frequency of
24 Hz, 28 mV peak-to-peak (V
pp
), and offset of V
cc
/2;
in Table 2 we summarize the results.
4 MEDICAL-GRADE VS.
OFF-THE-PERSON LEADS
One of the open questions in our off-the-person ap-
proach, with acquisition at the hands, is the relation
between the signals obtained with this type of sensor,
and those obtained with medical-grade stationary on-
the-person equipments, which are the gold standard
for ECG measurement. In this section we provide a
comparison of both approaches.
4.1 Methodology
We conducted experimental tests involving 8 vol-
unteers (4 males and 4 females), in which simul-
taneous recordings were performed using a Philips
PageWriter Trim III ECG device, and our off-the-
person sensor design with data acquisition performed
using the Biosignal Igniter Toolkit (BIT). The Philips
equipment was used in the standard 12-lead setting
(I-III, V1-V6, aVF, aVL, aVR), with conductive paste
applied to each of the electrodes. Our sensor was used
in the virtual ground setting with dry Ag/AgCl elec-
trodes, and the subject was asked to hold one of the
electrode leads in the right hand and the other on the
left hand.
The raw data from each device was bandpass fil-
tered using the same procedure, and all the individual
heartbeat waveforms were segmented. For a detailed
description of the adopted pre-processing methodol-
ogy, we refer the reader to (Canento et al., 2013) and
references therein. We focused on determining the
morphological similarity between individual heart-
beat waveforms collected using each of the sensor de-
vices. Given that dry electrodes are used in our sensor,
and also due to the fact that the on-the-person equip-
ment uses leads scattered through different anatomi-
cal locations, the amplitude of the signals collected by
each device is affected by a variable scale factor. To
account for such differences, in this study we adopted
the cosine distance as similarity metric (Equation 2).
D
cos
(x
i
,x
j
) = 1 −
∑
n
k=1
x
i
[k]x
j
[k]
p
∑
n
k=1
x
i
[k]
2
∑
n
k=1
x
j
[k]
2
. (2)
Off-the-PersonElectrocardiography
103
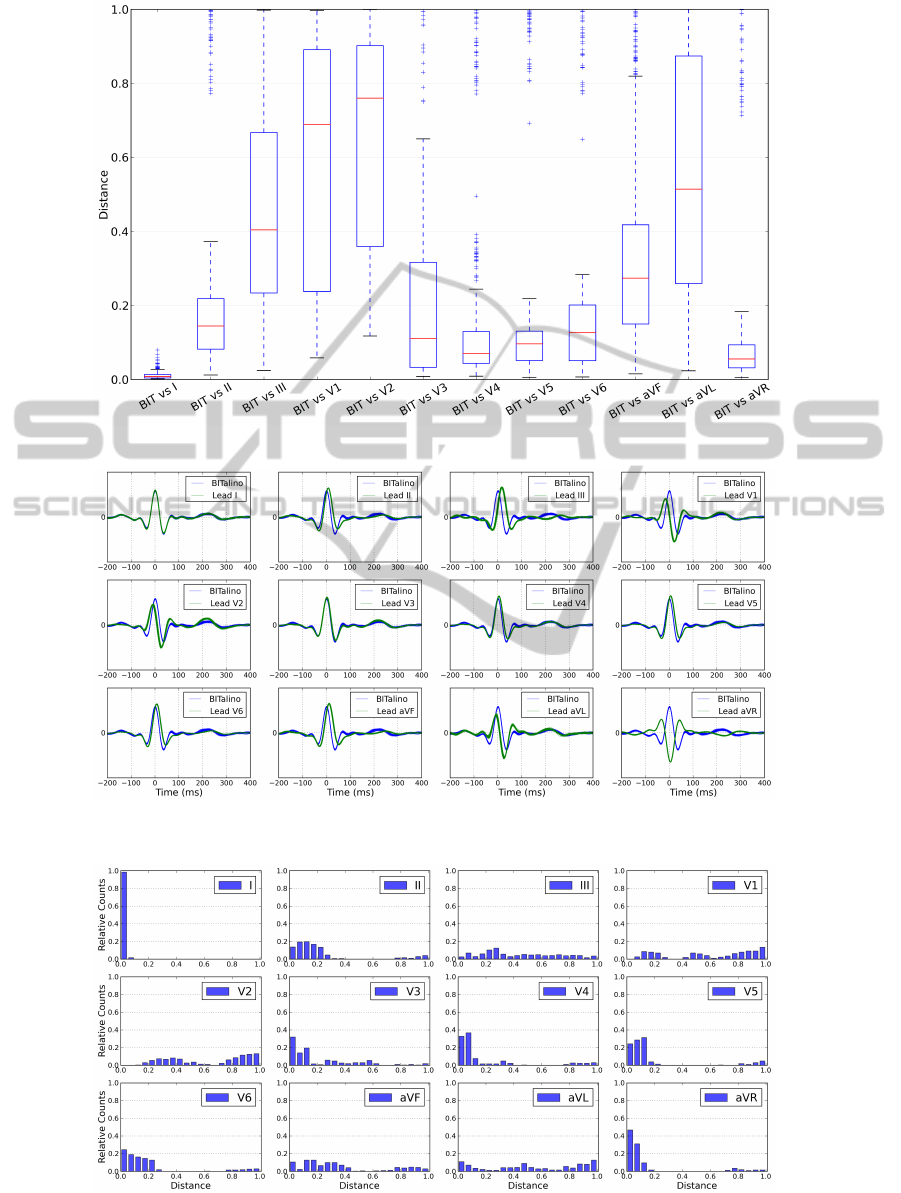
Figure 6: Boxplot of the distance between the off-the-person and each of the medical-grade leads.
Figure 7: Example of the segmented heartbeat waveforms obtained with the off-the-person and each of the medical-grade
leads for one of the tested subjects.
Figure 8: Histograms of the waveform distance between the off-the-person and each of the medical-grade leads.
CARDIOTECHNIX2013-InternationalCongressonCardiovascularTechnologies
104

4.2 Results
As shown in Figure 6, the signal obtained with our
off-the-person approach is clearly a lead I derivation.
The average cosine distance of nearly zero between
the off-the-person waveform and the lead I waveform
of the medical-grade device, together with the low
standard deviation across the overall set of subjects,
allow us to conclude that both signals are fully corre-
lated. This is further reinforced by the visual observa-
tion of the data; in Figure 7 we depict an overlay with
the segmented individual heartbeat waveforms for one
of the tested subjects. The off-the-person data is rep-
resented in blue, while the on-the-person data for each
of the leads is represented in green; in this case, the
off-the-person lead and the lead I data present an al-
most exact match.
Analyzing the case-by-case statistics, we are able
to observe that for some of the subjects, leads II, aVF,
aVR, and V3-V6 also exhibit a low average distance
to the waveform obtained using the off-the-person ap-
proach, and hence a high morphological similarity.
For example in Figure 7, V3 and V4 are quite simi-
lar to the off-the-person lead. The distributions of the
individual distances between our off-the-person lead
and each of the medical-grade leads for the overall
population can be found in Figure 8.
5 DISCUSSION AND FUTURE
WORK
Electrocardiography (ECG) has progressed a long
way since it was first introduced in the clinical prac-
tice. In the recent years, an increasingly growing
community has focused on improving the usability of
ECG equipment, and while most of the work has been
targeting wearable form factors (e.g. t-shirts), our
work has been pivoting towards what can be classified
as an off-the-person approach. In this paper we have
proposed a taxonomy of ECG data acquisition meth-
ods with respect to their intrusiveness level, described
an off-the-person sensor designed for ECG data ac-
quisition at the hands and fingers using dry electrodes,
and provided experimental results regarding the com-
parison between the off-the-person approach and con-
ventional medical-grade equipment.
Comparative tests have shown that the signals
obtained through our off-the-person approach are
matched to the conventional lead I derivation, and
that even without skin preparation or the use of con-
ductive paste to lower the impedance with the skin,
the morphology of the heartbeat waveform can be re-
trieved. Our work is targeted at ECG data acquisition
in a pervasive framework, by providing a simplified
sensor setup that can be used for everyday monitor-
ing. The applicability of our pervasive ECG approach
is not bound to the healthcare and clinical domains,
given that the ECG and derived measurements are
also appealing in a wide range of emerging applica-
tions, which include self-management, affective com-
puting (Medina, 2009) or even security (Lourenc¸o
et al., 2011)(Silva et al., 2013).
Future work will focus on further validating our
approach by increasing the number of tested sub-
jects, and also in the evaluation of contactless off-the-
person approaches targeting the evaluation of the rela-
tion between the signals obtained using such methods,
and the signals obtained using conventional methods.
ACKNOWLEDGEMENTS
This work was partially funded by Fundac¸
˜
ao
para a Ci
ˆ
encia e Tecnologia (FCT) under grants
PTDC/EEI-SII/2312/2012, SFRH/BD/65248/2009
and SFRH/PROTEC/49512/ 2009, whose support the
authors gratefully acknowledge. We would also like
to thank to Hospital de Santa Marta, Dr. Rui Cruz
Ferreira, Rui C
´
esar das Neves, and Jos
´
e Guerreiro for
their technical support during the development of this
work.
REFERENCES
Barold, S. (2003). Willem Einthoven and the birth of clin-
ical electrocardiography a hundred years ago. Card.
Electrophysiol. Rev., 7:99–104.
Besterman, E. and Creese, R. (1979). Waller - pioneer of
electrocardiography. British Heart Journal, 42:61–64.
Canento, F., Lourenc¸o, A., Silva, H., Fred, A., and Raposo,
N. (2013). On real time ECG algorithms for biometric
applications. In Proc. of the 6th BIOSIGNALS Conf.
Chi, Y., Jung, T.-P., and Cauwenberghs, G. (2010).
Dry-contact and noncontact biopotential electrodes:
Methodological review. IEEE Rev. Biomed. Eng.,
3:106 –119.
Chung, E. K. (2000). Pocketguide to ECG Diagnosis.
Blackwell Publishing.
de Isla, L. P., Lennie, V., Quezada, M., Guinea, J., Arce,
C., Abad, P., Saltijeral, A., Carolina, N., Crespo, J.,
Gonz
´
alvez, B., Macia, A., and Zamorano, J. (2011).
New generation dynamic, wireless and remote car-
diac monitorization platform. Int’l Journ. of Card.,
153(1):83–85.
Drew, B. J., Califf, R. M., Funk, M., Kaufman, E. S., Kru-
coff, M. W., Laks, M. M., Macfarlane, P. W., Sommar-
gren, C., Swiryn, S., and Van Hare, G. F. (2004). Prac-
Off-the-PersonElectrocardiography
105

tice standards for electrocardiographic monitoring in
hospital settings. Circ., 110(17):2721–2746.
Guerreiro, J., Martins, R., Silva, H., Lourenc¸o, A., and Fred,
A. (2013). BITalino: A multimodal platform for phys-
iological computing. In Proc. of the 10th ICINCO
Conf.
Lourenc¸o, A., Silva, H., and Fred, A. (2011). Unveiling
the biometric potential of Finger-Based ECG signals.
Comp. Intel. and Neuroscience, 2011.
Malmivuo, J. and Plonsey, R. (1995). Bioelectromagnetism:
Principles and Applications of Bioelectric and Bio-
magnetic Fields. Oxford Univ. Press.
Martins, R., Primor, D., and Paiva, T. (2011). High-
Performance groundless EEG/ECG capacitive elec-
trodes. In Proc. of the 6th IEEE MeMeA, pages 503–
506.
Medina, L. (2009). Identification of stress states from
ECG signals using unsupervised learning methods.
Master’s thesis, Univ. T
´
ecnica de Lisboa, Inst. Sup.
T
´
ecnico.
Postolache, O. A., Girao, P. M. B. S., Mendes, J., Pinheiro,
E. C., and Postolache, G. (2010). Physiological pa-
rameters measurement based on wheelchair embed-
ded sensors and advanced signal processing. IEEE
Trans. Instrum. Meas., 59(10):2564–2574.
Silva, H., Lourenc¸o, A., Canento, F., Fred, A., and Raposo,
N. (2013). ECG biometrics: Principles and applica-
tions. In Proc. of the 6th BIOSIGNALS Conf.
Silva, H., Lourenc¸o, A., Lourenc¸o, R., Leite, P., Coutinho,
D., and Fred, A. (2011a). Study and evaluation of
a single differential sensor design based on electro-
textile electrodes for ECG biometrics applications. In
Proc. of the 10th IEEE Sensors Conference, pages
1764 – 1767.
Silva, H., Palma, S., and Gamboa, H. (2011b). AAL+: Con-
tinuous institutional and home care through wireless
biosignal monitoring systems. In Handbook of Digi-
tal Homecare, volume 3, pages 115–142. Springer.
Timperley, J., Leeson, P., Mitchell, A., and Betts, T.
(2008). Cardiac Pacemakers and ICDs (Oxford Spe-
cialist Handbooks in Cardiology). Oxford Univ. Press.
Topol, E. (2012). The Creative Destruction of Medicine.
Basic Books.
Webster, J. G. (2009). Medical Instrumentation Application
and Design. Wiley.
CARDIOTECHNIX2013-InternationalCongressonCardiovascularTechnologies
106
