
A TELEMEDICINE SYSTEM FOR IMPROVED REHABILITATION
OF STROKE PATIENTS
Steffen Ortmann and Peter Langend
¨
orfer
IHP, Im Technologiepark 25, D-15236 Frankfurt, Oder, Germany
Keywords:
Telemedicine, Rehabilitation, Stroke, Body area network, Quality of life.
Abstract:
Analysis showed that costs of long-term care for stroke patients have increased from 13% to 49% of overall
costs in average in recent years. Therefore there is an urgent need for devising an effective long-term care
and rehabilitation strategy for stroke patients, which will involve the patients actively in the process. The
goal of our approach is the development of a telemedicine system which supports ambulant rehabilitation at
home settings for stroke patients with minimal human intervention. This system will combine state-of-the-art
monitoring devices forming a wireless Body Area Network that enable simultaneous measurement of multiple
vital parameters and currently executed movements that are particularly of interest from a Stroke rehabilitation
point of view. It will empower the patient to do more for fast recovery than today and provides clinical experts
with data not available today. By that, it leads also to a better understanding of the stroke recovery process,
higher recovery speed and thus, to reduced healthcare cost while improving patients’ quality of life.
1 MOTIVATION
Stroke is hitting about 2 Million people per year in
Europe (Kirchhof et al., 2009). For these persons the
effect of stroke is that they lose certain physical and
cognitive abilities at least for a certain time period.
More than one third of these patients, i.e., more than
670,000 people, return to their home with some level
of permanent disability leading to a significant reduc-
tion of quality of life which affects not only the pa-
tients themselves but also their relatives. Thus, the
manifesto of the Stroke Alliance for Europe (Stroke
Alliance for Europe, 2008) calls on ”all European
Governments to improve the availability of short and
long-term rehabilitation to enable all stroke survivors
to have access to life changing support.” Further,
”telemedicine systems for management of stroke” are
considered to become a key technology to cope with
expected challenges in future stroke care.
There is a strong need to improve the ambulant
care model, in particular, at the home settings, involv-
ing the patients into the care pathway, for achieving
maximal outcome in terms of clinical treatment as
well as quality of life. In addition to the dramatic ef-
fect of stroke for individuals, it has a strong impact
on our society as well. The total cost of stroke in the
EU was calculated to be over 38 billion in 2006. This
figure included healthcare costs (about 49% of the to-
tal cost), productivity loss due to disability and death
(23% of the total cost) and informal care costs (29%
of the total cost) (Kirchhof et al., 2009).
The prevalence of ageing in the European soci-
eties will lead to an increased number of people suf-
fering from stroke. For example, (Foerch et al., 2008)
predicts that the number of stroke patients in Hessen,
Germany; will increase from 20,846 in 2005 to more
than 35,000 in 2050 which equals to an increase of
nearly 70% within the next four decades. Experts pre-
dicted an increase of even 2.5 times (Go et al., 2001;
Miyasaka et al., 2006) leading to an enormous pres-
sure on the healthcare systems in terms of cost. The
effect on the healthcare cost might be even more sig-
nificant, since the current trend suggests also the ratio
of young and healthy persons to elderly persons to
decrease, so that the informal care cost will be shrink-
ing and thereby directly leading to increased direct
healthcare cost. This will become a real burden for
our economies.
We have just started an EU-funded research
project, called StrokeBack, which addresses both of
the sketched problem areas. The goal of this project is
the development of a telemedicine system which sup-
ports ambulant rehabilitation at home settings for the
stroke patients with minimal human intervention. In
the following, we will introduce objectives and meth-
ods to be investigated by StrokeBack before conclud-
270
Ortmann S. and Langendörfer P..
A TELEMEDICINE SYSTEM FOR IMPROVED REHABILITATION OF STROKE PATIENTS.
DOI: 10.5220/0003871502700274
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2012), pages 270-274
ISBN: 978-989-8425-88-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

ing with an outlook on the facts and preliminary re-
sults that we expect to have available soon.
2 OBJECTIVES
The StrokeBack project aims at increasing the reha-
bilitation speed of stroke patients while patients are in
their own home. The benefit we expect from our ap-
proach is twofold. Most patients feel psychologically
better in their own environment than in hospital and
also rehabilitation speed is improved. In addition, we
aim at exploiting the increased motivation of patients
when exercising with a tool similar to a gaming con-
sole. The ability of doing high quality exercises with-
out the need of being directly monitored by a physio-
therapist helps to reduce healthcare cost through min-
imisation of expensive human contact hours. Cur-
rently the quantity of hours performing occupational
(ergotherapeutic) and physiotherapeutic sessions are
restricted to payable effort for patient’s accommoda-
tion, transport or visit of therapists in the patient’s
home. StrokeBack aims at providing new technical
means and service structures to enable patients to en-
hance their healthiness by increasing the number of
training sessions while still being monitored by the
system. By ensuring proper execution of physiother-
apy trainings in an automated guided way, modulated
by appropriate clinical knowledge and in supervised
way only when necessary, StrokeBack empowers the
patients to exercise much more and at better quality
than it is possible today. By that StrokeBack improves
rehabilitation speed, and quality of life of the patient.
The StrokeBack concept will be complemented by
a Patient Health Record (PHR), in which rehabilita-
tion exercises, training measurements and vital data
of the patients will be stored. Thus, the PHR provides
all necessary information medical and rehabilitation
experts need to evaluate rehabilitation success, e.g. to
deduce relations between selected exercises and re-
habilitation speed of different patients, as well as to
assess the overall healthiness of the patient. In addi-
tion, the PHR will be used to provide the patient with
mid-term feedback, e.g., her/his rehabilitation speed
compared to average, as well as improvements over
last day/weeks, in order to keep patients motivation
high.
To summarise, the project goals are achieved by
investigating the following key objectives:
• Telemedicine supervision of rehabilitation exer-
cise.
• Continuous monitoring of impact of the exercises
also in ”normal” life situations.
• Integration of telemedicine rehabilitation and Per-
sonal Health Records for improved long term
evaluation of patient recovery.
• Providing feedback to health care professionals
on the impact of rehabilitation exercises.
Our system will empower the patient to do more
for fast recovery than today, it provides clinical ex-
perts with data not available today and by that it leads
also to a better understanding of the stroke recovery
process, higher recovery speed and thus, to reduced
healthcare cost while improving patients’ quality of
life.
3 APPROACH
Very recently gaming consoles have gained a lot of
attention when being used in the area of rehabilitation
(Anderson et al., 2010; Decker et al., 2009; Deutsch
et al., 2009; Gargin and Pizzi, 2010; John et al., 2009;
Miller, 2007). All publications report on very good
results in terms of speed of the rehabilitation process
and especially patient motivation (Sik-Lanyi et al.,
2005; Sik-Lanyi et al., 2006). A first evaluation has
shown that even though the majority of the publica-
tions deal with ”normal” rehabilitation process, e.g.,
after surgery, that similar results hold true for stroke
patients as well (Saposnik et al., 2010).
But most of the published articles about and envi-
sioned applications for computer-aided rehabilitation
of patients have revealed one major drawback. Since
these approaches target to train fine motor skills only,
they require the patients to already possess, or have
recovered up to, a certain level of mobility (Ander-
son et al., 2010). By that, these solutions cannot be
applied to patients having limited mobility such as
spasticity or partial palsy what is the major issue for
patients affected by stroke. These patients cannot be
asked to hold a sensing device by hand or to exercise
by stand. In contrast to that, StrokeBack aims to al-
ready assist in early stage of rehabilitation enabling
highly affected patients to profit from our proposed
monitoring system as well. Our system is designed
for ambulant use and targets to be adjustable to the
abilities of the patient - a patient-centric approach.
For example, it can be used by hemiplegic, paretic
patients as well as wheelchair users, too. By that we
intend to shorten the full time, stationary rehabilita-
tion and treatment program and allow patients to be
reintegrated into normal life as early as possible.
The StrokeBack concept puts the patient into the
centre of the rehabilitation process. It aims at exploit-
ing the fact the patients feel better at home, that it has
A TELEMEDICINE SYSTEM FOR IMPROVED REHABILITATION OF STROKE PATIENTS
271
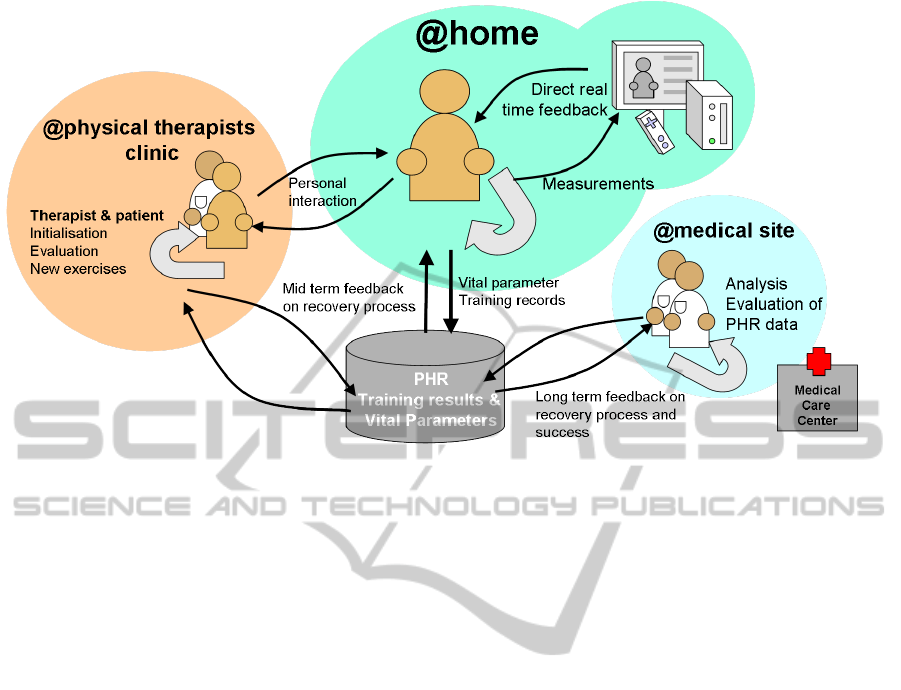
Figure 1: The StrokeBack rehabilitation cycle follows a patient-centric approach. The patient exercises at home while being
monitored by the StrokeBack system. The exercise schedule and the exercise results are supervised by ambulant physical
therapist care. All data are stored in the PHR to gather long term feedback on the rehabilitation progress.
been shown that patients train more if the training is
combined with attractive training environments. Fig-
ure 1 illustrates how we think the vision of such a
patient centric approach can come true. First the pa-
tients will learn physical rehabilitation exercises from
a therapist at the care centre or in a therapists’ practice
(left part of Figure 1). Then the patients will do the
exercises at home (middle part of Figure 1) and the
StrokeBack system will monitor their execution and
provide real time feedback on whether the execution
was correct or not. In addition, it records the train-
ing results and vital parameters of the patient. These
data will be analysed by medical experts (lower right
part of Figure 1) for assessment of the patient recov-
ery. Also the patient will get midterm feedback on
her/his personal recovery process. In order to ensure
proper guidance of the patient also the therapist will
get information from the PHR to assess the recovery
process and decide whether other training sequences
should be used, which are then introduced to the pa-
tient in the practice again.
In order to provide remote rehabilitation exercises
at gold standard level, i.e., as good as in a face-to-face
training with rehabilitation experts, we plan to exploit
the advanced features of today’s Body Area Networks
(BAN). A BAN attached to the patient enables perma-
nent monitoring of patients activity and vital parame-
ters. We aim to monitor and record the patients’ activ-
ity enabling them to regularly, maybe daily, exercise
independently from the guidance of the physical ther-
apist. With a correct instrumentation we expect to be
able to detect also unwanted additional movements.
In order to achieve a comparable monitoring by cam-
eras at least two of them need to be deployed at the
patient’s home. This is a costly solution which also
bears a privacy risk. Both issues can be solved with
our BAN based solution.
As one possible application, the physical thera-
pist has to look after the patient once a week only to
exploit the level of rehabilitation, to analyse the re-
sults of last exercises based on recorded data and to
take corrective action if necessary. Further, the physi-
cal therapist may show new exercises and configure a
new exercise schedule. By that, we intend to boost the
rehabilitation process at home. Finally, it allows the
physical therapists and the medical experts to get de-
tailed insights into kind and number of exercises the
patient executes during absence of the care persons.
The envisioned BAN can be worn by the patients
throughout the whole day, which enables comparing
actual movements in their daily life with the correct
movement patterns defined in rehabilitation exercises.
To simplify the configuration process of the system,
we will analyse and evaluate self-learning techniques
for exercise recognition, i.e., the StrokeBack sys-
tem may learn the correct behaviour (patient’s move-
ments) itself when exercises are carried out under in-
struction of the physical therapist.
We will additionally evaluate the feasibility and
requirements of using electronic Personal Health
Records (PHR) to store and document recorded data
and to remotely track the rehabilitation process, e.g.,
HEALTHINF 2012 - International Conference on Health Informatics
272

by the attending doctor. This includes the recordings
done during rehabilitation exercises and during daily
life. The recorded data will be stored and can then be
processed by healthcare professionals. The evaluation
can be used to deduce detailed information of effects
of individual exercises. This feedback can be used to
select exercises for other patients, to assess effective-
ness of exercises for specific groups of patients etc. In
addition the vital parameters can be used to assess the
healthiness of the patients which might even help to
assess the probability of a further stroke.
4 OUTLOOK
We currently work out the technical and medical ba-
sics for realising the ideas behind the StrokeBack
project. Until the conference, we will be able to
present and discuss insights into the following re-
search areas of the project:
Rehabilitation Exercises. Here, we will focus on
a couple of standard exercises that are to be imple-
mented. As it is common practise for rehabilitation
of stroke patients, these exercises will lean on move-
ments required for daily live, e.g., grasping at differ-
ent objects, lifting a cup, etc. Therefore the scope of
allowed as well as of forbidden movements have to be
determined for each exercise. The most difficult task
to be considered is the fact that every type of exercise
has to be individually adapted to the needs and capa-
bilities of the patient. To enable such patient-centric
individualisation, we intend to experiment with self-
learning techniques that would allow the system to
monitor all movements made when the patient is ex-
ercising under supervision of a physical therapist. By
that, the system can learn the ”ideal” or correct exe-
cution of the exercise and hence, can give adequate
assistance when the patient is exercising alone.
Measurement Methods. Based on the exercises to
be implemented, kind of movements and required key
evaluation data are assessed, upon which the kind
of sensors, e.g., for measuring acceleration and ro-
tation, and their placement on the human body are
determined. Suitable body tracing modelling algo-
rithms will be developed to enable feasible real-time
training. In general, the sensor system should not
only be able to determine correctness of exercises but
must rather be able to autonomously detect wrong or
evasive movements the patient may carry out. Our
idea is to extent the WSN with an Electro-Myo-Gram
(EMG) sensing system for providing static/dynamic
muscle activity monitoring. For example, such sys-
tem would allow detecting hidden evasive movements
in the shoulder or neck when moving the arm, which
are not detectable by acceleration sensors only.
Human Computer Interaction. Human-to-
computer interfaces have to be designed for both
patients and therapists. This means using the system
must be intuitive, clear and self explanatory! On
the one side, the methods for initialisation and
introduction of exercises must be useable not only
by computer specialists but especially by physical
therapists. Here, the self-learning techniques of the
system should properly deal with these issues. On the
other side, our system is to be designed especially for
elderly people, since the majority of patients suffering
from stroke is older than 50 years. Consequently,
the training programs must be kept very simple and
attractive to keep the motivation high. We will follow
a ”what you do is what you see” philosophy, where
each movement of the patient is displayed also on
the monitor in front of the patient. We intend to
use avatar interfaces to which the patient interacts
with like in a computer game, i.e., the patient’s
avatar executes the same movements in real time. In
addition, we would like to exploit known increased
learning effects in rehabilitation, which occur when
providing optical inputs for the patient in addition
to the movements executed. Finally, the system can
replay correct exercise execution at any time, even if
no physical therapist or medical staff is present.
In summary, the StrokeBack main goal is to an-
imate stroke patients to do more for fast recovery
themselves. Our system provides just technical assis-
tance empowering stroke patients to reach their own
rehabilitation goals with adequate means. Last but not
least, the StrokeBack system provides detailed feed-
back about the rehabilitation progress to the patient
and medical care staff as well. From the medical view,
it provides a unique chance to monitor the effects of
various exercises in details. This enables to document
the effectiveness of single exercises when applied to
different patients suffering from various impairments
and hence, it provides stroke experts with high reso-
lution data and knowledge not available today.
ACKNOWLEDGEMENTS
The StrokeBack research project is supported by the
European Commission under the 7th Framework Pro-
gramme through Call (part) identifier FP7-ICT-2011-
7, grant agreement no: 288692.
A TELEMEDICINE SYSTEM FOR IMPROVED REHABILITATION OF STROKE PATIENTS
273

REFERENCES
Anderson, F., Annett, M., and Bischof, W. (2010). Lean
on wii: Physical rehabilitation with virtual reality and
wii peripherals. Annual Review of CyberTherapy and
Telemedicine, 8:181–184.
Decker, J., Li, H., Losowyj, D., and Prakash, V. (2009). Wi-
ihabilitation: rehabilitation of wrist flexion and exten-
sion using a wiimote-based game system. Governor’s
School of Engineering and Technology Research Jour-
nal.
Deutsch, J., Robbins, D., Morrison, J., and Bowlby, P.
(2009). Wii-based compared to standard of care bal-
ance and mobility rehabilitation for two individuals
post-stroke. In Virtual Rehabilitation International
Conference, 2009, pages 117–120. IEEE.
Foerch, C., Misselwitz, B., Sitzer, M., Steinmetz, H.,
and Neumann-Haefelin, T. (2008). Die schlagan-
fallzahlen bis zum jahr 2050. Deutsches
¨
Arzteblatt,
105(26):467–73.
Gargin, K. and Pizzi, L. (2010). Wii-hab: Using the wii
video game system as an occupational therapy inter-
vention with patients in the hospital setting. Health
Policy Newsletter, 23(1):4.
Go, A., Hylek, E., Phillips, K., Chang, Y., Henault, L.,
Selby, J., and Singer, D. (2001). Prevalence of diag-
nosed atrial fibrillation in adults. JAMA: the journal
of the American Medical Association, 285(18):2370.
John, M., H
¨
ausler, B., Frenzel, M., Klose, S., Ernst,
T., B
¨
ucher, J., Seewald, B., Liebach, J., Wolschke,
M., and Klinkm
¨
uller, B. (2009). Rehabilitation im
h
¨
auslichen umfeld mit der wii fit–eine empirische
studie. Ambient Assisted Living-AAL.
Kirchhof, P., Adamou, A., Knight, E., Lip, G., Norrving, B.,
and de Pouvourville, G. (2009). How Can We Avoid a
Stroke Crisis? Oxford PharmaGenesis. ISBN 978-1-
903539-09-5.
Miller, J. (2007). Wii speeds up the rehab process. USA
Today, 15.
Miyasaka, Y., Barnes, M., Gersh, B., Cha, S., Bailey, K.,
Abhayaratna, W., Seward, J., and Tsang, T. (2006).
Secular trends in incidence of atrial fibrillation in olm-
sted county, minnesota, 1980 to 2000, and implica-
tions on the projections for future prevalence. Circu-
lation, 114(2):119.
Saposnik, G., Teasell, R., Mamdani, M., Hall, J., McIlroy,
W., Cheung, D., Thorpe, K., Cohen, L., and Bayley,
M. (2010). Effectiveness of virtual reality using wii
gaming technology in stroke rehabilitation. Stroke,
41(7):1477–1484.
Sik-Lanyi, C., Geiszt, Z., and Magyar, V. (2006). Using it
to inform and rehabilitate aphasic patients. Informing
Science: International Journal of an Emerging Trans-
discipline, 9:163–179.
Sik-Lanyi, C., Szab
´
o, J., Pall, A., and Pataky, I. (2005).
Computer-controlled cognitive diagnostics and reha-
bilitation method for stroke patients. ERCIM News,
61:53–54.
Stroke Alliance for Europe (2008). Safe manifesto. In 6th
World Stroke Congress, Vienna, Austria.
HEALTHINF 2012 - International Conference on Health Informatics
274
