
IS E-HEALTHCARE CHART CONTRIBUTORY TO PATIENT
SAFETY?
Kiyomu Ishikawa, Takeshi Tanaka, Minoru Ikeuchi and Hidehiko Tsukuma
Department of Healthcare Informatics and Hospital Systems Management,
Hiroshima University Hospital, Hiroshima, Japan
Keywords: E-Healthcare Chart, Questionnaire Survey, Medical safety, Provision of training opportunities.
Abstract: Toward 503 hospitals evaluated by Japan Council Health Care (JCHC), the questionnaire survey was
conducted and analysed according to 2 groups of pre-2005 and post-2006 system introduction. As the result,
it was found that despite with the annual improvement in the e-healthcare chart system function, both
information system and users’ operation were insufficient with concern of medical accidents: About sixty
per cent of the hospitals have experienced information-system-related harmful incidents. Among the
hospitals that implemented information security education of health information system, 60% had triggered
harmful incidents, and preavoid experience. In contrast, 40% of hospitals without information security
education had triggering experience. We found preavoid experiences in 70% of those reported no preavoid
experiences. There is a possibility that the organizational development for information literacy raises the
consciousness of users towards harmful incidents through the accumulation of information on such
incidents.
1 AIM
E-healthcare Chart or EHR has been developed as
the key medium to support individual lives by
means of multi-occupational networking. Today, it
could be the core tool in team healthcare process.
While, according to the survey of 273 public and
national hospitals (together 144,019 beds) from
January to June, 2009, 172 facilities reported fatal
medical accidents (JCQHC). Here, based on “The
survey of the development and issues on the
computerization of medical process” of the hospitals
included in the study, the experience rates of
harmful incidents are compared with the provision
of training opportunities.
2 METHOD
The internet-based questionnaire survey was
conducted from July to August, 2009, and 1488
target hospitals which had been authorized to meet
the functional criteria by Japan Council for Quality
Health Care (JCQHC) were asked to fill in the forms
with both multiple choice and open questions.
The focus was “the relation between the
occurrence of harmful incidents or prevention
experience, management organization and training
system.”
The following topics were analyzed.
a. The introduction status of a health care
information system
b. The status of the education of the hospital
personnel for the use of the healthcare
information system
c. Is healthcare chart monitored to check the
risk of harmful incidents?
In Japan, the Ministry of Health, Labor and
Welfare enacted “the guidelines for safety
management of health information systems” (Japan
Ministry of Health, Labour and Welfare in 2005. In
order to find the effects of the guideline
enforcement, the target hospitals were classified into
2 groups, one that included hospitals with systems
introduced before 2005, and the other with hospitals
that introduced the system later.
3 RESULT
3.1 The Introduction Status of Heath
Information System
Answers were received from 503 hospitals (33.8%).
430
Ishikawa K., Tanaka T., Ikeuchi M. and Tsukuma H..
IS E-HEALTHCARE CHART CONTRIBUTORY TO PATIENT SAFETY?.
DOI: 10.5220/0003846904300433
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2012), pages 430-433
ISBN: 978-989-8425-88-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)
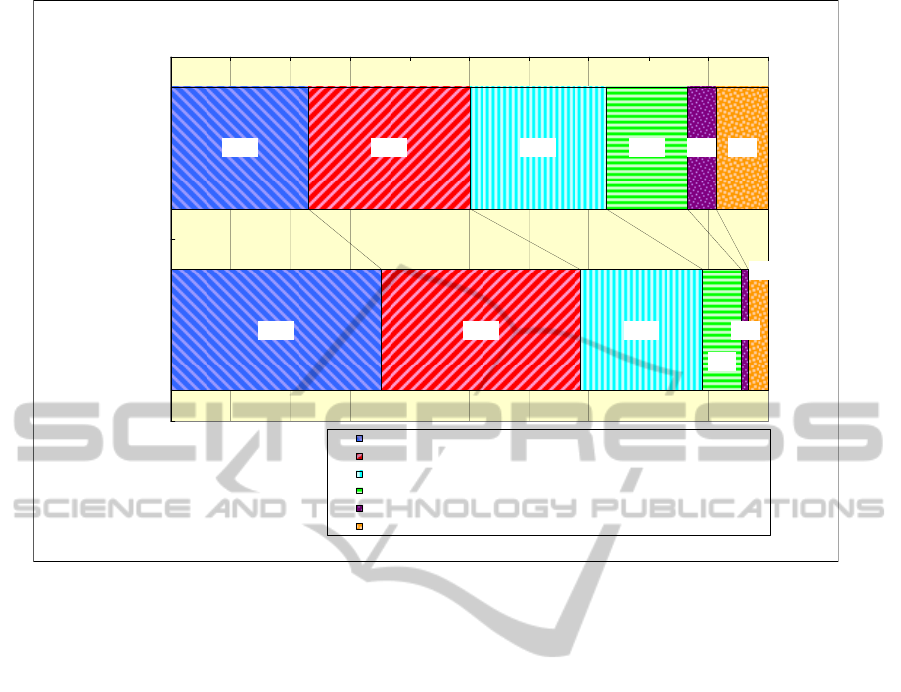
Figure 1: The confirmation function ordering receipt.
The larger scale hospitals showed the highest
answering rate. Focusing on the occupation of
answerers, clerks are listed at the top, followed by
nurses, system engineers of information
management department of hospitals.
This survey shows that above 90% hospitals
introduced health information systems. Among them
187 hospitals (41%) which introduced health
information system after 2006. Looking at the
introduction rates in relation to the size of the
hospitals we found that hospitals with over 201 beds
actively progress the computerization of an ordering
system.
Furthermore, focusing on the medical care
process from physicians’ ordering to the
confirmation of nurses’ practice after order
receiving, the systems of the post-2006 hospitals
have more advanced checking function than pre-
2005 hospitals (Fig 1).
3.2 The Relation to Harmful Incident
Among the hospitals that implemented information
security education of health information system,
59.6% (242/406) had triggered harmful incidents
and 38.4% (153/406) had not, and 61.3% (249/406)
had preavoid experiences and 38.7% (157/406) had
not.
In contrast, 38.1% (37/97) of hospitals without
information security education had triggering
experience, and 54.6% (53/71) had not. We found
preavoid experiences in 33.0% (32/97) of the
hospitals, and 67.0% of those hospitals reported no
preavoid experiences (65/97). (Fig. 2)
3.3 The Cause of Harmful Incident
The system-based harmful incidents were caused by
users operation or program imperfection rather than
system troubles such as “Input of wrong
information” (71.7%; 200/279), “No input of
necessary information” (29.4% (82/279) in the
system without warning function and 25.8%
(72/279) in disregard of warning function), and
“Impossible input due to master registration or
master maintenance imperfection” (22.9%; 64/279).
(Fig 3)
On the other hand, the cases of preavoid harmful
incidents by system operation are listed as “Patient
misconception” (68.3%; 192/281), “Dosing wrong
medicine” (56.6%; 159/281) or “Ordering of wrong
procedure or test” (31.3%; 88/281). “The prevented
Cases of Patient Misconception” are somewhat
higher in the post-2006 group.
23.0%
35.3%
27.1%
33.2%
22.8%
20.6%
13.6% 4.9%
1.2%
8.7%
6.5%
3.2%
0.0% 10.0% 20.0% 30.0% 40.0% 50.0% 60.0% 70.0% 80.0% 90.0% 100.0%
Before 2005
After 2006
Confirmation of "Ordering receipt"
Confirmation the stage from "Odering receipt" to "Pre-performance"
Confirmation of "Done"
Unable to Confirm
The others
NA
391
340
IS E-HEALTHCARE CHART CONTRIBUTORY TO PATIENT SAFETY?
431
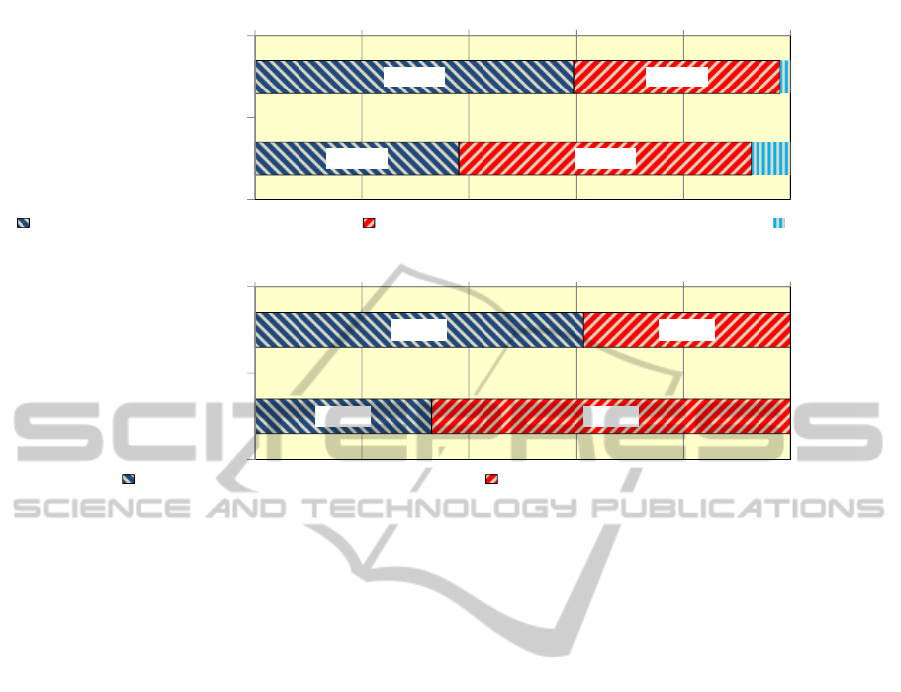
Figure 2: Relations between education and experiences of harmful incidents.
4 DISCUSSION
4.1 The Occurrence / Prevention of
Harmful Incident and Staff
Education
When the survey results mentioned from 3.1 to 3.3
are compared with the past case (Ishikawa et al.,
2007), (though the answering hospitals and
answerers were different), it is supposed that e-
Healthcare chart has become well-established as the
standard tool in the Japanese hospitals. Especially,
due to the progress of “checking function of medical
process”, it will shortly meet the functional
requirements as information infrastructure for use
inside the hospital. It is also supposed that the
system with the Bar-code-used matching function
between patients and medical practice became more
popular. Nevertheless, the present survey did not
provide the definite evidence that the functional
improvement has contributed to prevention of
harmful incidents.
As shown in Sec. 3.2 (Fig 2), there is a
possibility that the organizational development for
information literacy raises the consciousness of
users towards harmful incidents through the
accumulation of information on such incidents.
4.2 The Occurrence / Prevention of
Harmful Incident and Staff
Education
According to 3.3 (Fig 3), the causes of human issues
are mainly input error related causes and master
troubles. In order to settle these issues, from the
view point of another questionnaire survey by
JCQHC (JCQHC, 2009), it is crucial to classify
cases into “(1) Careless mistakes” and “(2) Common
and organizational issues”. Furthermore, the cases of
“Careless mistakes” need to be examined whether
there are possibilities of improvement by means of
warning in case of wrong input of names, quantity,
and item selection or pick up of mandatory input
items and warning to check mandatory input.
Under the on-going rapid computerization, the
partnership building between vendors and users will
be the key for designing the practical measures
based on the integrated examination outcomes of
multiple hospitals and rapidly implementing the
measures identified in the software.
Through this study, it was found that harmful
incidents do not always result from information
system-based hardware or software troubles. They
are related with the human factors included in the
medical process.
59.6%
38.1%
38.4%
54.6%
0% 20% 40% 60% 80% 100%
Hospitals with
security education
Hospitals without
security education
Harmful Incidents was triggered Harmful Incidents was not experienced Others
N=406
N=97
61.3%
33.0%
38.7%
67.0%
0% 20% 40% 60% 80% 100%
Hospitals with
security education
Hospitals without
security education
Experience of preavoid No experience of preavoid
N=406
N=97
HEALTHINF 2012 - International Conference on Health Informatics
432
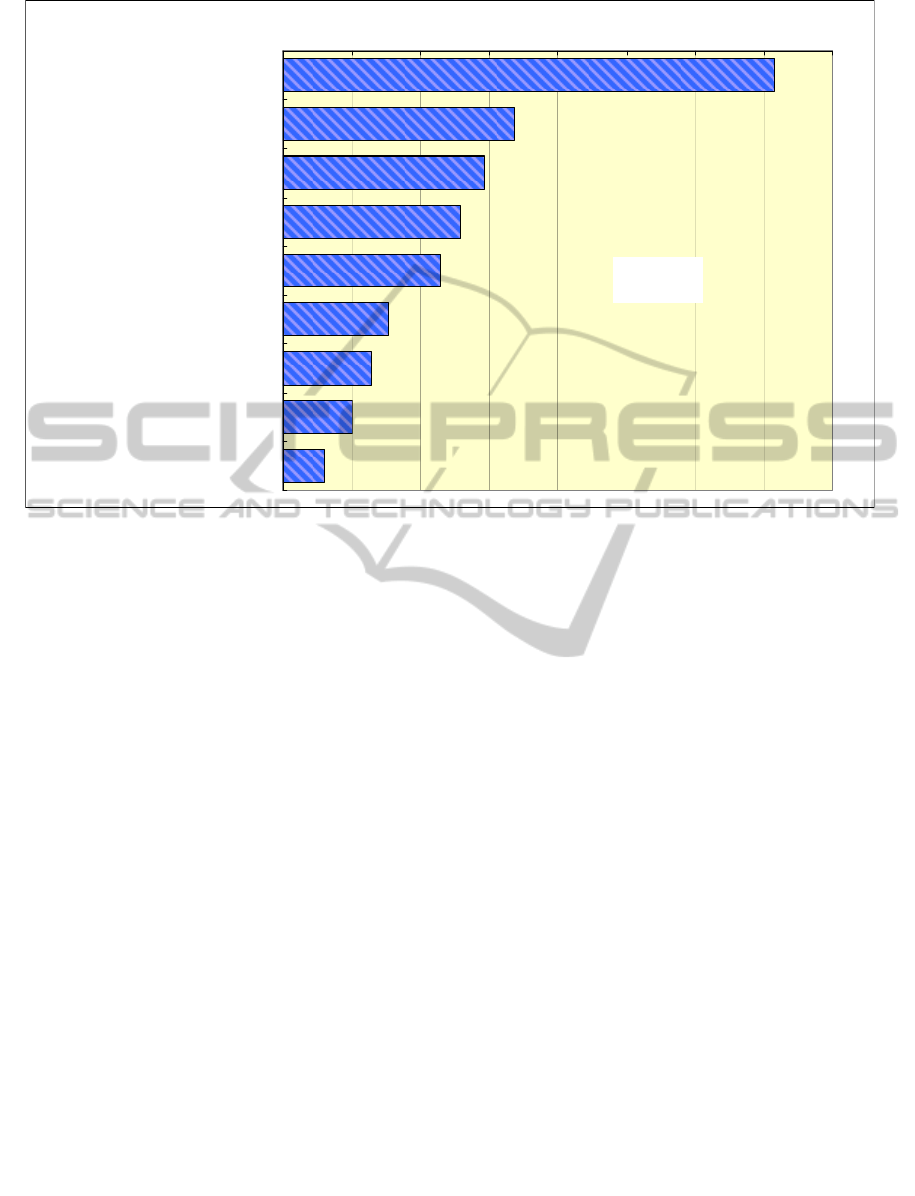
Figure 3: The Causes of Information System-Related Harmful Incidents.
5 CONCLUSIONS
The aim of the e-Healthcare Chart system
introduction has changed for this decade, and at
present the aim is not achieved completely. Three
principles of preservation by e-media including e-
healthcare chart were “Accountability”,
“Availability”, and “Storage ability” based on eight
principles of the OECD Board of Directors. It means
that in order to assure “patient safety”, the medical
quality should be improved by interactive
confirmation of medical process from ordering to
practice among multi-occupational sites. However,
despite the diverse requirements of system functions,
they are hardly achieved at present. For this aim, the
specialized usage of patient data and system
designing along with medical performance should be
prioritized.
ACKNOWLEDGEMENTS
This work was supported by the Grant-in-Aid for
Scientific Research (A) No. 21249035 of the
Ministry of Education, Culture, Sports, Science and
Technology, Japan.
REFERENCES
JCQHC, The 18
th
Report on the Medical Accident
Collection Project of JCQHC: http://www.med-safe.
jp/pdf/report_18.pdf
Japan Ministry of Health, Labour and Welfare, The
guideline on a safety management of medical informa-
tion system (the 1
st
edition): http://www.mhlw.go.jp/
shingi/2005/03/s0331-8.html
K. Ishikawa et al. “The Guideline of the Personal Health
Data Structure to Secure Safety Healthcare –The
balance between use and protection to satisfy the
patients’ needs-: Int. J. of Med. Info. Vol. 76 No. 5-6,
pp. 412-418 (2007).
JCQHC, For Making the case collection book: The
meeting material for the 3
rd
review meeting on
computerized information devices in 2009 (2009).
71.7%
33.7%
29.4%
25.8%
22.9%
15.4%
12.9%
10.0%
6.1%
0.0% 10.0% 20.0% 30.0% 40.0% 50.0% 60.0% 70.0% 80.0%
* Input of Wrong Information
Networking Trouble
* No Input of Mandatory Information
(Without Warning Function)
* No Input of Mandatory Information
(With Warning Function)
* Unable to Input (Imperfection of Master
Registration and Maintenance)
Unable to Input (System Trouble)
No Image Output (Designing Imperfection)
No Image of Mandatory Information
Others
* Human Causes
N-279
IS E-HEALTHCARE CHART CONTRIBUTORY TO PATIENT SAFETY?
433
