
A MULTI-CRITERIA SORTING APPROACH FOR DIAGNOSING
MENTAL DISABILITIES
Paulo Freitas
1
, Carlos Henggeler Antunes
2
and Jorge Dias
1
1
Institute of Systems and Robotics, University of Coimbra, Coimbra, Portugal
2
INESC Coimbra, University of Coimbra, Coimbra, Portugal
Keywords: Multi-criteria models, Outranking methods, ELECTRE TRI, Mental disabilities, Alzheimer disease.
Abstract: A multi-criteria model tackled by an outranking method devoted to the sorting problem is presented to
support decision making in assessing individual mental disabilities using information required in the
Clinical Dementia Rating scale. This diagnosis process is a critical factor for adapting treatments to the
current stage of the disease and improving health care and quality of life. The criteria required in the
Clinical Dementia Rating scale have been considered as an input for developing our multi-criteria model,
the output of which is the classification of each individual under evaluation in a pre-defined ordered class
(category) as an indicator of the revealed level of mental disabilities. A method based on the exploitation of
an outranking relation for the sorting problem is used to compare the individual information according to
multiple evaluation criteria with reference profiles (specified standards) that define the boundaries of the
classes. This methodological approach is substantially different from the ones based on the aggregation of
the different criteria using weighted-sums to produce a “common value” measure. The method requires
meaningful technical parameters, such as weights (herein perceived as true importance coefficients of the
multiple evaluation aspects), distinct thresholds to ascertain the outranking classification, and a cutting level
establishing the exigency of the classification. A realistic example using the decision support system Iris is
presented to illustrate the results.
1 INTRODUCTION
Decision making processes are daily tasks associated
with several contexts in people's life. In health care
decisions, inadequate evaluations may lead to bad
judgments and consequently result in inappropriate
treatments and negative health effects. Therefore,
sound models and methodologies shall be developed
to support making the best decisions when handling
with situations concerning people's health care in
face of multiple, often conflicting, evaluation
aspects. A specific area that requires feasible and
reliable diagnosis is associated with dementia
assessment and treatments. In these cases the
diagnosis decision support process is generally
divided in several stages and is based on multiple
criteria to reach a comprehensive evaluation. This
type of decisions is increasingly important due to the
growth of life expectancy, which is accompanied by
an increasing prevalence of health impairments and
mental-health problems such as dementia (Hendrie,
1998). Early and accurate identification of
individuals who are at a high risk of developing
dementia is regarded as a research priority. This
identification followed by effective interventions
may significantly contribute to reducing the
prevalence and incidence of dementia diseases,
improving the quality of life both of the patients and
their caregivers, and making a more efficient use of
the resources needed to provide adequate
institutional and home health care. The process of
early identification assumes even greater importance
knowing that there are already treatments to help
slowing the disease progression and prevention
strategies including lifestyle changes (Roberson and
Mucke, 2006). The DESCRIPA Study (Vissera et
al., 2008) presents an evaluation over three years of
a set of clinical criteria for further analysis of which
variables best predict dementia, in particular
Alzheimer’s disease. Functional impairment in
people in risk of dementia has been studied to
understand what are the indicators associated with
the disease’s progress (Wilkins et al., 2007).
392
Freitas P., Henggeler Antunes C. and Dias J..
A MULTI-CRITERIA SORTING APPROACH FOR DIAGNOSING MENTAL DISABILITIES.
DOI: 10.5220/0003752303920398
In Proceedings of the 1st International Conference on Operations Research and Enterprise Systems (ICORES-2012), pages 392-398
ISBN: 978-989-8425-97-3
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

The aim of this work is to develop a multi-
criteria model and use a multi-criteria method based
on an outranking relation to provide decision support
in the diagnosis of dementia related diseases of
individuals according to the assessment of their
mental status. Taking as a basis the Clinical
Dementia Rating (CDR) scale, a tree of criteria has
been developed to encompass all the relevant aspects
for a comprehensive assessment. A multi-criteria
method devoted to the sorting problem and a
computer package for helping the analysis have been
selected. This decision aid approach expects to
receive data (the performance of each individual
according to each criterion) from an external
assessment system. Other inputs include the
technical parameters required by the methodological
component. The output consists in the assignment of
each individual to a pre-defined ordered category
associated with the physical/mental status of the
individual.
Furthermore, this enables to carry out a long
term analysis of the individual historical data, which
may establish a correlation between the model's
output and the actual situation. Our approach is
aimed at providing a tool for helping technical staff
in charge of diagnosing dementia diseases to support
making the best decisions, increasing the accuracy
and reliability of the evaluation.
The assessment of dementia diseases has been
traditionally made using the aggregation of different
perspectives of evaluation (criteria) by means of
some type of scoring and weighted-sum approaches
thus transforming the performances of the entities
under evaluation according to the different criteria
into a “common value” score (Robert et al., 2010).
We believe that in most cases, as in the one under
study herein, it is sufficient for analysis and provides
more confidence on the results the assigning of the
entities under evaluation (individuals) to pre-defined
ordered categories of merit rather than producing a
single numerical figure. Furthermore, a more
detailed analysis within each category is possible
whenever it is considered useful to improve the
discrimination of the evaluation model.
In this setting it is important to appraise the
entities using known standards or profiles.
Moreover, it is also convenient to evaluate entities
on an “as they come” basis. This capability of
evaluating each individual in absolute terms
according to reference profiles, and not just in
comparison with their peers, as well as the need to
include evaluation aspects expressed in different
units using different types of scales (also
qualitative), can be accomplished using the
ELECTRE TRI method (Mousseau, Slowinski,
Zielniewicz, 2000). The ELECTRE TRI method is
adequate for our assessment problem because it does
not require controversial (scale-dependent) weight
specification in order to obtain a single score for
each individual and allows the definition of standard
profiles (establishing the frontiers between the
categories) with which each individual is compared.
Those profiles may be updated for further
adjustments as required by distinct practical
situations. This type of evaluation model can bring
advantages to support medical staff in the
assessment of dementia diseases in comparison with
some traditional processes of applying pre-defined
scoring scales.
Other approaches based on multi-criteria models
and methods have been proposed in the literature,
specifically to assist the process of diagnosing
Alzheimer's disease. The work presented in (Castro,
Pinheiro, Pinheiro, Tamanini, 2011) proposes a
hybrid model combining influence diagrams and
multi-criteria methods to compare the values for
each entity in a set and then perform a rank within
the group. Bayesian Networks are used in (Pinheiro,
Castro, Pinheiro, 2008) to serve as a modelling tool
for aiding in decision making for the diagnosis of
Alzheimer’s disease. In (Castro et al., 2011; Pinheiro
et al., 2008; Filho, Pinheiro, Coelho, Costa, 2009)
good overviews about related works for this area are
presented, proposing approaches for decision aiding
models applied to medical activities. Moreover, the
performance achieved applying methods based on
ELECTRE IV and a genetic algorithm is presented
in (Filho, Pinheiro, Coelho, 2009; Filho, Pinheiro,
Coelho, Costa, 2010). Experiments have been made
(Costa, Filho, Coelho, Pinheiro, 2009; Filho et al.,
2009) to compare the accuracy and effectiveness of
different multi-criteria decision aid methods with
different data sets, the conclusions pointing out to
some changes in the results for the same models.
The paper is organized as follows. Section 1
provides the interest and motivation of this study.
Section 2 presents a brief overview about multi-
criteria outranking methods and the software
package used in this work to accomplish the goals
previously defined. In section 3 the multi-criteria
model and the design of the overall approach are
presented. Section 4 describes some illustrative
results obtained using a case study. Finally,
conclusions are drawn and future work is outlined in
section 5.
A MULTI-CRITERIA SORTING APPROACH FOR DIAGNOSING MENTAL DISABILITIES
393
2 THE ELECTRE TRI METHOD
The ELECTRE TRI method is a member of the
ELECTRE (Elimination and Choice Translating
Reality) family of multi-criteria methods (Roy,
1996). ELECTRE methods are based on the
construction and exploitation of an outranking
relation (“outranking” having the meaning of “is at
least as good as”). ELECTRE TRI is devoted to the
sorting (classification) problem, which consists in
assigning each entity under evaluation to one of a
pre-defined set of ordered categories (C
1
,…,C
k
),
according to several evaluation criteria g
j
(j=1,…,n).
Each entity object of evaluation (individual) is
described through a vector of multi-criteria
performances. The categories are defined by
specifying reference profile vectors (b
0
,…,b
k
), being
each reference profile b
h
(h=1,…,k-1) the upper
bound of category C
h
and the lower bound of
category C
h+1
.
The assignment of each entity a
i
to a category C
h
is done by comparing its value in each criterion to
the corresponding reference profiles. The method
assigns each entity to the highest category such that
its lower bound is outranked by a
i
. The outranking
relation is verified by comparing a credibility index,
computed by using the differences in performance
and the criterion weights, with a cutting level
λ
(
λ
∈
[0.5,1]), which defines the “majority requirement”
and consequently the exigency of the classification.
In ELECTRE methods weights shall be
perceived as true coefficients of importance of the
criteria (their “voting power”), which are scale-
independent, i.e. not linked to the scales in which
each criterion is measured. This is a totally different
interpretation of weights with respect to weights
used as technical parameters for translating the
scores in each criterion into a global score. For
further details about ELECTRE TRI see (Mousseau
et al., 2000).
The ELECTRE TRI method requires the
specification of a set of technical parameters (which
convey meaningful preference information): the
reference profiles defining the categories (b
0
,…,b
k
),
the criterion weights w
j
, the cutting level (
λ
), a set of
indifference (q
j
), preference (p
j
) and veto (v
j
)
thresholds for each criterion g
j
and reference
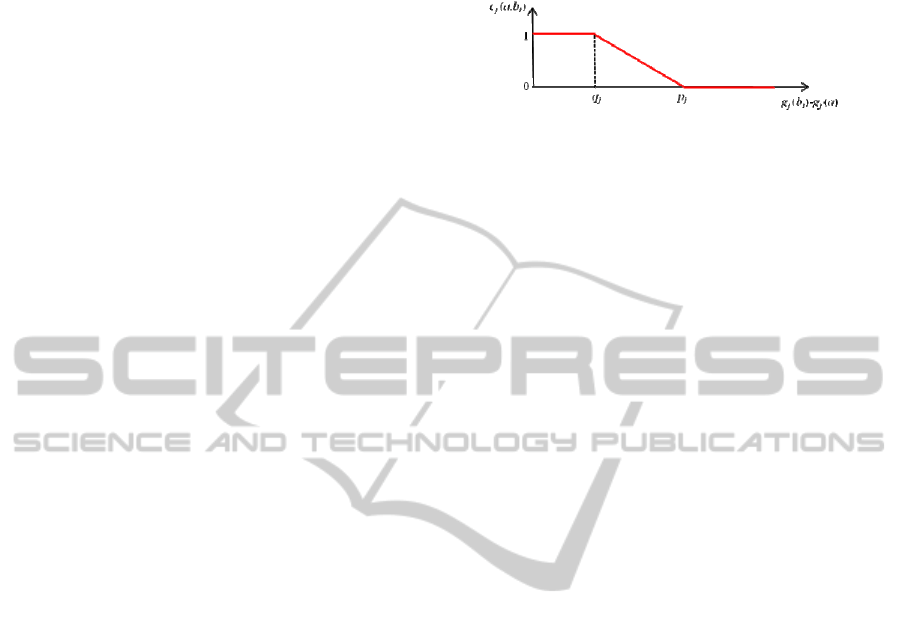
profiles. Indifference and preference thresholds
characterize the acceptance of imprecision in the
judgment by considering two entities as indifferent
when their individual performances in each criterion
g
j
differ less than a specified amount q
j
. The
transition from indifference to preference is not
sharp but changes linearly from q
j
to p
j
, this being
captured by the criterion concordance index c
j
.
Figure 1 illustrates the computation of the criterion
concordance index when comparing alternative a,
and the profile b
i
for criterion g
j
.
Figure 1: Criterion concordance index.
The veto thresholds are quite relevant in our case
study because they capture “non-compensatory”
situations in which a very bad performance in any
criterion prevents an entity of being classified in the
best category or even force it to be classified in the
worst category independently of having very good
performances in all other criteria. In general,
practical evaluation models require the consideration
of a certain level of non-compensation, at least for
some criteria.
The assignment classification provided as result
of ELECTRE TRI is the desired indicator of the
disease progress level for each individual. In this
paper, we assume that the input data (the
performance of each individual in any criterion
expressed in a quantitative or qualitative scale) must
be supplied by an external system and/or medical
inputs. It is advisable that an expert panel, for
instance a medical board, could supply the technical
parameters (reference profiles, weights and
thresholds) referred to above. The overall decision
support approach will be discussed in detail in
section 3.
3 AN APPROACH BASED ON AN
OUTRANKING METHOD
Multi-criteria analysis methods are largely
unexploited so far on health care, particularly in
classification processes using medical information.
In our work, a multi-criteria approach using the
ELECTRE TRI method is proposed to deal with a
model that can use behavioural and cognitive data to
infer about the mental and physical state of
individuals.
The keystone of this study has been the
development of a comprehensive multi-criteria
model encompassing all the fundamental axis of
evaluation. The structuring phase is an essential step
to reach a stable multi-criteria evaluation model
from a generally “messy situation” through a process
of unveiling and refinement procedure of a
ICORES 2012 - 1st International Conference on Operations Research and Enterprise Systems
394
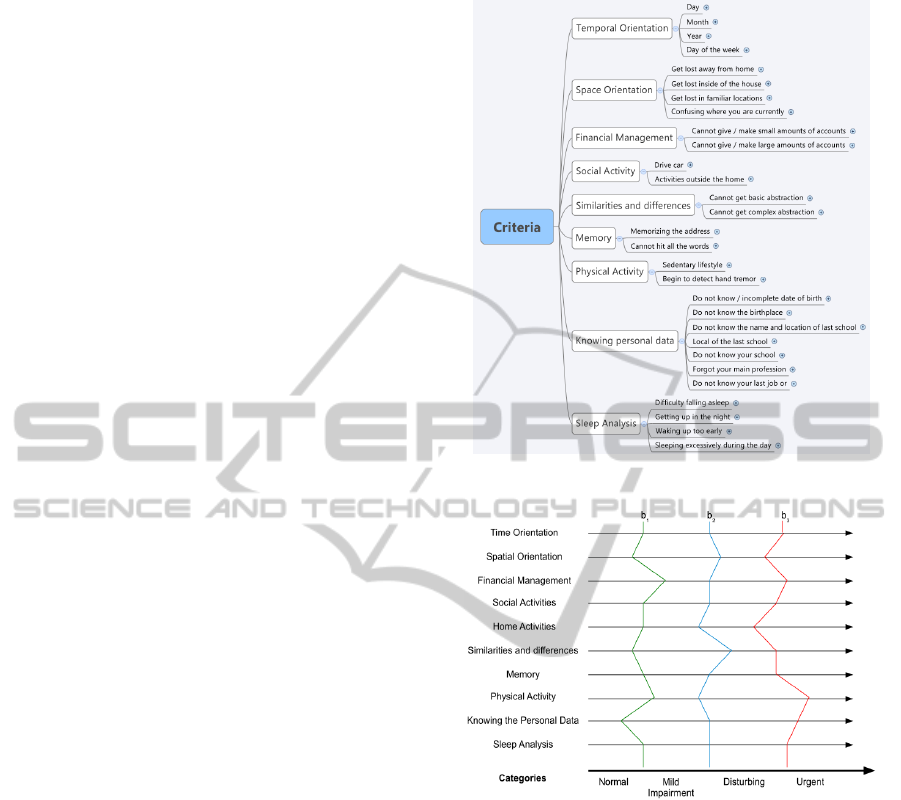
consistent family of criteria. The fundamental
criteria that we have selected (tree of criteria) to
assess any individual are depicted in Figure 2, in
which the operational criteria are inside the boxes.
The fundamental criteria, which are dealt with by the
method, are derived from a set of sub-criteria
identified in the structuring phase. The score of any
individual in each fundamental criterion results from
a weighted aggregation of the scores in the
corresponding sub-criteria. Typically, each sub-
criterion is measured in a qualitative scale according
to the frequency of occurrences using three levels
with the associated meaning of: “it never happens”,
“it happens sometimes”, and “it happens very often”.
An external system is responsible for providing
the performance of each individual according to
each evaluation criterion in a given measurement
scale. A group of experts, or medical board, provides
the technical parameters required by the method.
This can be done in an iterative way for model
calibration purposes.
The establishment of a pattern of behaviours that
is indicative of the disease status, which can be
parameterized, conveys the information to define the
reference profiles that define the boundary of the
classes. These profiles have been specified by means
of scales used in Neuroscience, Psychology, and
other related areas, to select which type of
behaviours should be used in the evaluation of the
mental state of the individual. The CDR scale is one
of the most well-known scales used in the process of
Alzheimer’s disease diagnosis. This type of scales is
applied as questionnaires, which raise the
subjectivity issue when the patient or the caregiver is
answering to them. The subjectivity inherent to
answering the questionnaires is somehow mitigated
by means of the use of the indifference, preference
and veto thresholds in the operational framework of
ELECTRE TRI.
Four categories (classes) have been identified to
which any individual will be assigned based on the
information about his/her mental and physical
performances:
• Urgent (earlier medical intervention is
required).
• Disturbing (medical accompanying is needed).
• Mild Impairment (attention shall be paid to
evolution).
• Normal (no need to be followed on a regular
basis).
Figure 2: Criteria tree.
Figure 3: Categories and reference profiles.
If judged necessary more classes can be
considered to increase discrimination between
statuses. This would imply to define more technical
parameters associated with new reference profiles.
Figure 3 outlines graphically the categories
bounded by the reference profiles, which each
individual is compared with. The reference profiles
are displayed in Figure 3 just for illustrative
purposes of how categories are defined and they do
not represent the actual values used in the
experiments whose results are presented in section 4.
Table 1 presents each reference profile (b
1
, b
2
and b
3
) and the corresponding criterion performance
(by this order in each criteria), which may be
considered as “reference individuals” establishing
the frontier between the categories.
A MULTI-CRITERIA SORTING APPROACH FOR DIAGNOSING MENTAL DISABILITIES
395
Table 1: Criteria and Reference Profiles.
Criteria Reference Profiles (b
1
, b
2
, b
3
)
Temporal
Orientation
- Do not know the current day
- Often does not know the day of the
week
- Do not know the current day of the
week
- Often does not know the month
- Does not know the month
or
- Often does not know the year
Space
Orientation
- Often gets lost away from home
- Lose yourself away from home
- Often lost in familiar locations
- Often confused where currently is
- Confused where currently is
- Often gets lost inside of the house
Financial
Management
- Cannot give / make accounts of large
amounts
- Cannot give / make accounts of small
amounts
- Lose track of the money
Social
Activity
- Often does not drive car
- Left driving car
- Decrease in activities outside home
- Lack of activities outside home
Similarities
and
differences
- Slight decrease in the level of
abstraction
- Cannot get basic abstraction
- Often does not know
Memory
- Failure at the address details
- Cannot say all the words
- Often misses the address
Physical
Activity
- Decrease in motor activity
- Sedentary lifestyle
- Begins to detect hand tremor
Knowing
personal data
- Does not know the birthplace
- Does not know the name and location of
the last school
- Does not know / incomplete date of
birth
- Does not know his education level
- Does not know the last job
or
- Forgot the main profession
Sleep Analysis
- Issues falling asleep
- Waking up too early
- Sleeping excessively during the day
- Getting up in the night
In order to classify the validity of the outranking
relation between the individual and the reference
profiles is assessed, thus determining the assignment
of the individual to one of the categories. In Table 1
the reference profiles are presented in terms of the
meaning associated with the scores in each criterion
and not actual values, using the CDR scale as a
guideline.
4 SOME ILLUSTRATIVE
RESULTS
In order to test our model, data of 20 individuals
have been used associated with persons in various
stages. We have used the Iris software (Dias and
Mousseau, 2003) to implement our method and to
test it in distinct scenarios. The data contain
information about selected individuals with a very
good mental state, others displaying intermediate
disease indicators, and others with a bad diagnosis.
That is, the entities under evaluation have been
selected to span a wide set of conditions to illustrate
the operation of the multi-criteria model coupled
with the Iris package implementing a version of
ELECTRE TRI.
Initially, all the technical parameters required by
the method (see sections 2 and 3) have been
specified: definition of the categories in which the
individuals will be classified; preference,
indifference and veto thresholds for each criterion
and reference profile; criterion weights; cutting
level. Although this specification process may seem
to impose a significant burden on the decision
makers, these parameters are essential to bear their
experience and insightful information into the
sorting procedure. Usually these parameters are
elicited from decision makers with the aid of an
analyst with expertise on the methodological
component to ease the elicitation process. Moreover,
some of these parameters can be preset (according to
experience in previous studies). For instance,
indifference and preference thresholds may be
established as percentages (e.g., 2% and 10%,
respectively) of the value ranges in each class.
Figure 4 presents the results obtained using the
Iris package for the cutting level λ=0.5. This means
that a “simple majority” of criteria supporting the
outranking relation is required. The left column
displays the 20 entities under evaluation (individual
0-19) and each column C1–C4 is associated with a
category (ordered from the worst to the best one):
C1 – Urgent; C2 – Disturbing; C3 – Mild
Impairment; C4 – Normal. The partially coloured
matrix displays the assignment of each entity to a
category. The darker cells represent the assignment
proposed by Iris for each individual, which is
associated with a central combination of parameters.
The lighter cells represent the other possible
assignments, which are obtained for other feasible
combinations of parameters under certain constraints
(in this case, criterion weights that may vary within
intervals).
ICORES 2012 - 1st International Conference on Operations Research and Enterprise Systems
396
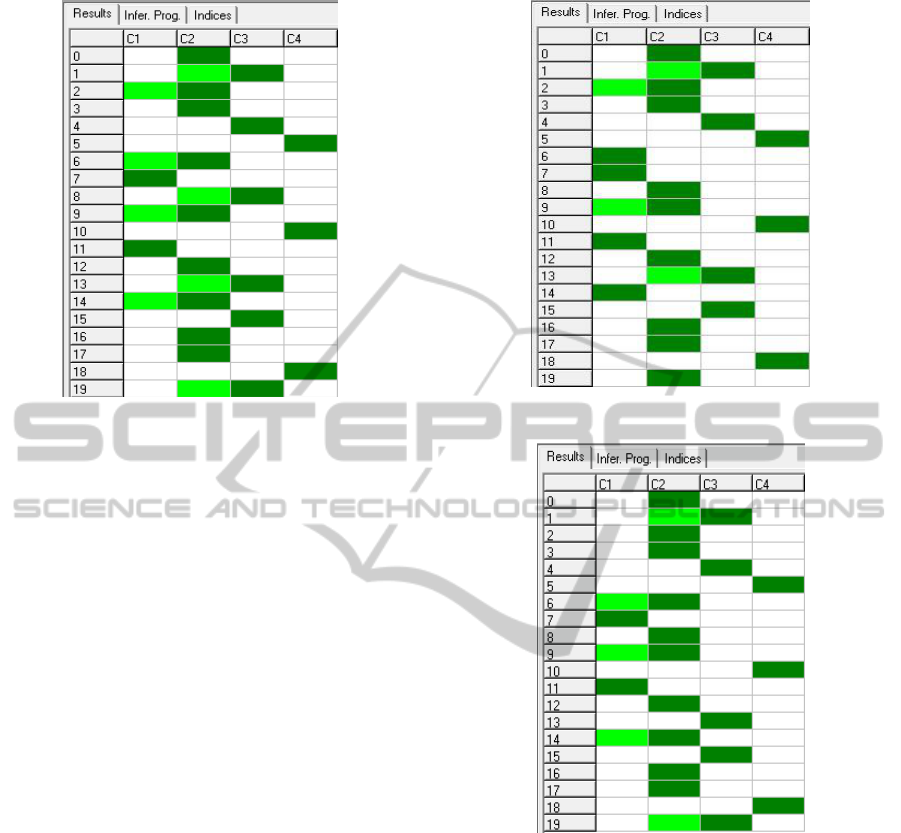
Figure 4: Assignments with λ=0.5.
Analyzing Figure 4, we can conclude, for
example, that individual 0 is restricted to category
C2 – Disturbing (all sets of weights lead to this
result). Individual 1 is assigned to category C3 –
Mild Impairment according to the central parameters
but he/she can also be sorted into category C2 (since
this is feasible for other parameter combinations).
Figure 5 displays the results obtained when using
a cutting level λ=0.85, that is, increasing
significantly the exigency of the classification
derived from the outranking relation verification.
Therefore, the assignments proposed by Iris for each
entity are now “less favourable”. For example,
individual 14 was previously classified in C2, using
central parameters, and after the increase of λ his/her
assignment is restricted to C1.
More experiments have been done to analyze the
effects of changing the criterion weights for testing
scenarios in which the contribution for the
classification is not equal for all the criteria. That is,
we assume that there are criteria more important
than others, so they are given a higher “voting
power” in ascertaining the outranking relation.
Figure 6 illustrates the results obtained using a
cutting level λ=0.5 and different criterion weights
reflecting the following importance rank (in
decreasing order): “Space Orientation” and “Sleep
Analysis”; “Financial Management”; “Temporal
Orientation” and “Social Activities”; all the other
criteria. Comparing the results obtained in Figure 4
and Figure 6 we conclude that individuals 2 and 13
can now attain classes C1 and C2, respectively, and
individual 8 can just be assigned to class C2, thus
displaying the impact that criterion weight changes
can have on the final classification.
Figure 5: Assignments with λ=0.85.
Figure 6: Assignments with λ=0.5 and with different
weights.
The interactive environment provided by Iris
may be used, for instance, to assess the trend of the
progression of the disease for a given individual.
The same individual in different points in time may
be considered as different entities under evaluation
and the relative assignment is easily assessed.
Lighter coloured cells are also indicative that
individuals may be close to change to the next
categories.
5 CONCLUSIONS
This paper presents a multi-criteria model to provide
A MULTI-CRITERIA SORTING APPROACH FOR DIAGNOSING MENTAL DISABILITIES
397

decision support in the diagnosis process of
dementia cases. The model is tackled using a
methodology based on an outranking relation, which
is exploited for a sorting problem in which
individuals are assigned to categories associated
with the perceived status of the disease. Categories
are defined using references profiles with which
individuals are compared to check the outranking
relation.
This approach offers the possibility to adjust the
reference profiles as well as other technical
parameters required by the method to better suit the
different usage scenarios. The use of ELECTRE
TRI’s technical parameters may help to cope with
subjectivity issues that are present in the traditional
processes of applying pre-defined scales. This multi-
criteria approach offers a flexible methodology
capable of being adjusted according to the objectives
of medical staff in the assessment of dementia
diseases.
Future developments include using previous
examples of classified individuals to infer new
reference profiles and classification assignments,
analyze thoroughly the reliability of considering
“non-central” classifications in the output results as
tendency indicators, perform tests with other multi-
criteria decision aid methodologies to conclude
about the reliability achieved when using different
approaches.
REFERENCES
Castro, A., Pinheiro, P., Pinheiro, M., Tamanini, I. (2011).
Towards the Applied Hybrid Model in Decision
Making: A Neuropsychological Diagnosis of
Alzheimer's Disease Study Case. International
Journal of Computational Intelligence Systems, 4, (1),
652-656.
Costa, N., Filho, A., Coelho, A., Pinheiro, P. (2009).
Selecting prototypes for two multicriteria
classification methods: A comparative study. World
Congress on Nature & Biologically Inspired
Computing. 1702 – 1707.
Dias, L., Mousseau, V. (2003). IRIS – Interactive
Robustness Analysis and Parameters Interference for
Multicriteria Sorting Problems (Version 2.0). User
Manual, Document 1/2003 INESC Coimbra.
http://www.inescc.pt/documentos/DocInt_1_2003.pdf
Dias, L., Mousseau, V.( 2003). IRIS: A DSS for Multiple
Criteria Sorting Problems. Journal of Multi-Criteria
Decision Analysis,12, 285-298.
Filho, A., Pinheiro, P., Coelho, A. (2009). Towards the
Early Diagnosis of Alzheimer’s Disease via a
Multicriteria Classification Model. Proceedings of the
5th International Conference on Evolutionary Multi-
Criterion Optimization. Springer, 393-406.
Filho, A., Pinheiro, P., Coelho, A., Costa, N. (2009).
Comparison of two prototype-based multicriteria
classification methods. IEEE Symposium on
Computational Intelligence in Multi-Criteria
Decision-Making, 133 – 140.
Filho, A., Pinheiro, P., Coelho, A., Costa, N. (2010).
Comparison of Two MCDA Classification Methods
over the Diagnosis of Alzheimer's Disease.
Proceedings of the 4th International Conference on
Rough Sets and Knowledge Technology. Springer,
334-341.
Hendrie, H. (1998). Epidemiology of dementia and
Alzheimer’s disease. American Journal Geriatric
Psychiatry, 6, S3–S18.
Mousseau, V., Slowinski, R., Zielniewicz, P. (2000). A
user-oriented implementation of the ELECTRE-TRI
method integrating preference elicitation support.
Computers & Operations Research, 27, 757-777.
Pinheiro, P., Castro, A., Pinheiro, M. (2008). A
Multicriteria Model Applied in the Diagnosis of
Alzheimer's Disease: A Bayesian Network. IEEE
International Conference on Computational Science
and Engineering, 15–22.
Roberson, E., Mucke, L., 2006. 100 Years and Counting:
Prospects for Defeating Alzheimer’s Disease. Science,
314, 781-784.
Robert, P., Ferris, S., Gauthier, S., Ihl, R., Winblad, B.,
Tennigkeit, F. (2010). Review of Alzheimer’s disease
scales: is there a need for a new multi-domain scale for
therapy evaluation in medical practice?. Alzheimer’s
Research & Therapy, 2(24).
Roy, B. (1996). Multicriteria Methodology for Decision
Analysis. In Kluwer Academic Publishers, Dordrecht.
Vissera, P., et al. and DESCRIPA study group. (2008).
Development of Screening Guidelines and Clinical
Criteria for Predementia Alzheimer’s Disease.
Neuroepidemiology, 30 (4), 254-265.
Wilkins, C., Wilkins, K., Meisel, M., Depke, M.,
Williams, J., Edwards, D. (2007). Dementia
Undiagnosed in Poor Older Adults with Functional
Impairment. The American Geriatrics Society, 55 (11),
1771–1776.
ICORES 2012 - 1st International Conference on Operations Research and Enterprise Systems
398
