
USABILITY PROBLEMS IN A HOME TELEMEDICINE SYSTEM
Anders Bruun and Jan Stage
Department of Computer Science, Aalborg University, Selma Lagerlöfs Vej 300, DK-9220 Aalborg East, Denmark
Keywords: Home telemedicine, Usability evaluation, Usability problems.
Abstract: Home telemedicine systems have the potential to reduce health care costs and improve the quality of life for
many patients, including those suffering from chronic illness. This requires that the systems have
functionality that fulfils relevant needs. Yet it also requires that the systems have a high level of usability in
order to enable their users to employ the required functionality, especially if the target user group is elderly
people. This paper reports from a usability evaluation of a home telemedicine system. Five elderly persons
carried out specified tasks with the system, and based on that we identified usability problems with the
system. The problems are presented, analysed in relation to 12 different usability themes and related to
results from other evaluations of similar systems.
1 INTRODUCTION
There is growing interest in devices for home
telemedicine. At world level, the life expectancy will
increase from 2005 to 2050 to 67 years, and in
developing countries to 76.5 years (UN, 2006). This
has considerable consequences for healthcare
budgets. Another key challenge is that the number of
people with chronic illness is increasing and, due to
frequent checkups at hospitals, these patients face
reduced quality of life, as they have limited freedom
to perform their daily activities.
The aim of home telemedicine is to reduce health
care costs and at the same time increase the quality
of life for patients. Home telemedicine systems
allow patients to conduct measurements from their
own home (e.g. glucose measurements for diabetes
patients) and send the results to the hospital. Other
systems put even more emphasis on self-
management by supporting patients to take care of
their own treatment. If home telemedicine systems
are successful, they will reduce the workload of
medical staff at the hospitals and in the patients’
home, and relieve the patients from visits to the
hospital or even hospitalization (Kaufman et al.,
2003).
For home telemedicine systems to be successful,
they must be safe and provide the required
functionality. Many researchers have inquired into
these aspects. Unfortunately, there are numerous
examples of systems that fail despite having the
right functionality, because the prospective users
cannot use the system for its intended purpose. A
problematic or incomprehensible user interface is a
typical source of such problems.
Usability is a measure of the extent to which
prospective users are able to apply a system in their
activities (Rubin, 1994). A low level of usability
means that users cannot work out how to use a
system, no matter how elaborate its functionality is
(Nielsen, 1993).
The potential of home telemedicine systems can
only be realized if the systems have a high level of
usability. Thus a high level of usability is a
prerequisite for achieving savings on the healthcare
costs and a better quality of life for the patients
through use of home telemedicine systems. A high
level of usability is particularly important when the
main user group is elderly people, who may be
constrained by motor, perceptual, cognitive and
general health limitations (Fisk and Rogers, 2002)
and, in addition, may have a low level of computer
literacy.
1.1 Usability Evaluation of Health Care
Systems
A number of research activities have studied home
telemedicine systems and frameworks that aid in
reducing the societal and individual costs of
chronically ill elderly. The focus here has been on
the functionality that is required from such systems.
Examples are technology for ubiquitous biological
monitoring using mobile phones, wearable sensory
302
Bruun A. and Stage J. (2010).
USABILITY PROBLEMS IN A HOME TELEMEDICINE SYSTEM.
In Proceedings of the Third International Conference on Health Informatics, pages 302-309
DOI: 10.5220/0002744603020309
Copyright
c
SciTePress

devices, multi modal platforms, framework and
architectural descriptions and literature reviews of
observed medical effects (Eikerling, et al., 2009;
Fensli and Boisen, 2008; Jaana and Paré, 2006;
Pascual et al., 2008; Sasaki et al., 2009; Sashima et
al., 2008; Souidene et al., 2009; Taleb et al., 2009).
The target user group of these systems is primarily
elderly people.
Kaufman et al. (2003) conducted a case study
where a home telemedicine system for elderly
diabetes patients was evaluated through interviews,
cognitive walkthrough and field usability testing.
The evaluated system featured video conferencing,
transmission of glucose and blood pressure readings,
email, online representation of clinical data and
access to educational materials. The study focuses
on a methodology for conducting usability
evaluation. It also provides a basic overview of
barriers such as individual competencies, system
usability issues and contextual variables. Two user
examples of these barriers are provided.
A significant number of studies deal with health
care systems where the target user group is
professional medical staff. This includes evaluation
of the usability of desktop, mobile and other
healthcare systems with the aim of reducing medical
errors introduced by technology. Examples are
systems designed for supporting handheld
prescription writing, decision support, ordering of
lab tests, patient records, family history tracking etc.
(Ginsburg, 2004; Johnson et al., 2004; Kushniruk et
al., 1996; Kushniruk and Patel, 2004; Kushniruk et
al., 2005; Linder et al., 2006; Peleg et al., 2009;
Peute and Jaspers, 2007).
The research results presented here represent
significant work on the needed functionality of home
telemedicine systems as well as on methods for
evaluating the usability of such systems. There is
also considerable work on usability problems
experienced with systems that are targeted at the
medical staff. Yet much less efforts have been
devoted to identification of usability problems in
systems targeted at patients.
1.2 Objective
In this paper, we present a study where we evaluated
the usability of a home telemedicine system targeted
at elderly people. The aim was to better understand
key usability problems that such users experienced
when using home telemedicine systems. A better
understanding of these problems is vitally important
for future design of home telemedicine systems with
a high level of usability.
In the following we describe the home
telemedicine system and the usability evaluation we
conducted with a group of elderly people (section 2).
Section 3 presents the results with focus on key
usability problems experienced by the users with this
specific system. In section 4, we discuss these
usability problems in relation to results found in
other studies in order to emphasize more general
problems for home telemedicine systems targeted at
patients. Finally, section 5 provides the conclusion.
2 METHOD
In this section, we describe our usability evaluation
of the home telemedicine system.
2.1 Usability Evaluation
System. The system was a telemedicine system
intended for home use by elderly people to monitor
their health. It included a Health Care System device
(HCS) for data collection and transmission with a
display, a speaker and four buttons for interaction,
see Figure 1. As the manufacturer of the HCS
wishes to remain anonymous we do not provide a
reference to the system evaluated.
Y
N
Figure 1: Sketch of the data collection and transmission
device (HCS) of the evaluated healthcare system.
With secondary devices such as blood pressure
meter, blood sugar meter and scales, users are able
to conduct measurements at home and transfer these
to the HCS via Bluetooth, an infrared link or a serial
cable. At regular intervals, the device also asks the
patients various pre-programmed questions
regarding their health.
The system automatically transfers collected data
to a health care center, where a nurse, doctor or
other person is monitoring the health for a group of
elderly patients. The system is sent to the patients in
a package with a manual.
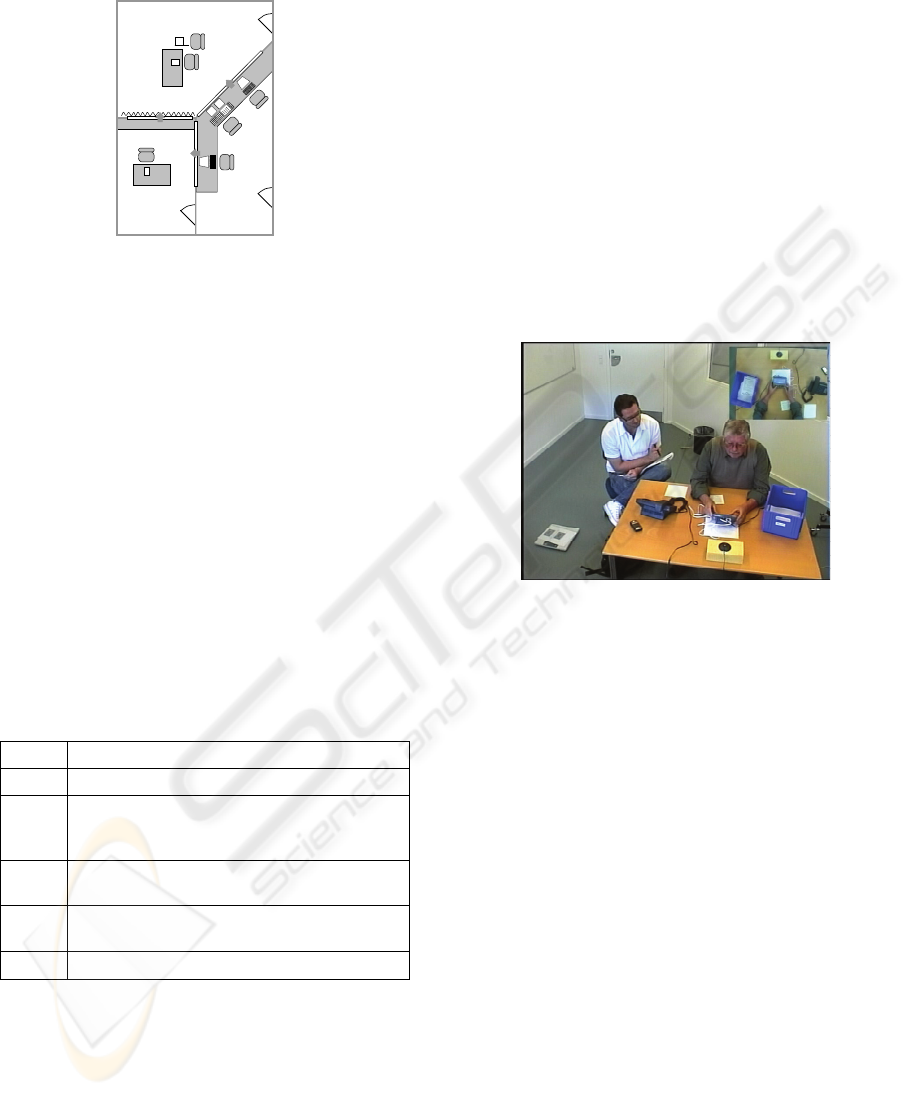
Setting. The tests were conducted in a usability
laboratory, see Figure 2. In Subject room 1, a test
participant was sitting at the table operating the
system. The test monitor was sitting next to the
participant, see Figure 3. Two data loggers and a
USABILITY PROBLEMS IN A HOME TELEMEDICINE SYSTEM
303
technician who controlled cameras and microphones
were in the control room during all tests.
Subject Room 1
Sub
j
ect
Room 2
Control
Room
curtain
operator
Figure 2: The setting in the usability laboratory.
Participants. The system was evaluated with 4 male
and 1 female users. It should be noted that in the
area of Human Computer Interaction it is customary
to conduct formative usability evaluations using 5
test participants as this, from a cost/benefit point of
view, is the most feasible. This number is based on
studies conducted by Nielsen and Landauer (1993)
showing that by using 5 test participants evaluators
are able to identify 85 % of the total number of
usability problems.
Since the system primarily is intended for use by
elderly people, we selected test subjects ranging
from 61 to 78 years of age. None of them had
previous experience with this or any similar system.
Their experience in using electronic equipment in
general varied; two were novices, two were slightly
experienced and the last was experienced.
Table 1: Task assignments used in the usability tests.
Task # Task
1
Connect and install the HCS and secondary devices.
2
Transfer the data from the blood sugar meter to the
HCS. The blood sugar meter is connected using a
cable.
3
Measure the weight and transfer the data from the
scale to the HCS.
4
A new wireless blood sugar meter is used. Transfer
the data from this to the HCS.
5
Clean the equipment.
Six usability evaluators were involved, all
graduate students specializing in human-computer
interaction and working on their master thesis. They
were all experienced in conducting usability
evaluations. None of them had worked with health
care systems before, and none of them knew the
product in advance. In the evaluation, one of them
served as test monitor in all five tests, and two
served as loggers.
Procedure. Before the test started, the test
participants were asked to fill in a questionnaire with
demographic information. The test monitor then
introduced the system and evaluation procedure.
This included an introduction to the think-aloud
protocol. The tasks were given to the test subjects
one at a time. The test monitor’s job was primarily
to ensure that the test participants were thinking
aloud and give them advice if they got completely
stuck in a task. There were five tasks, see Table 1.
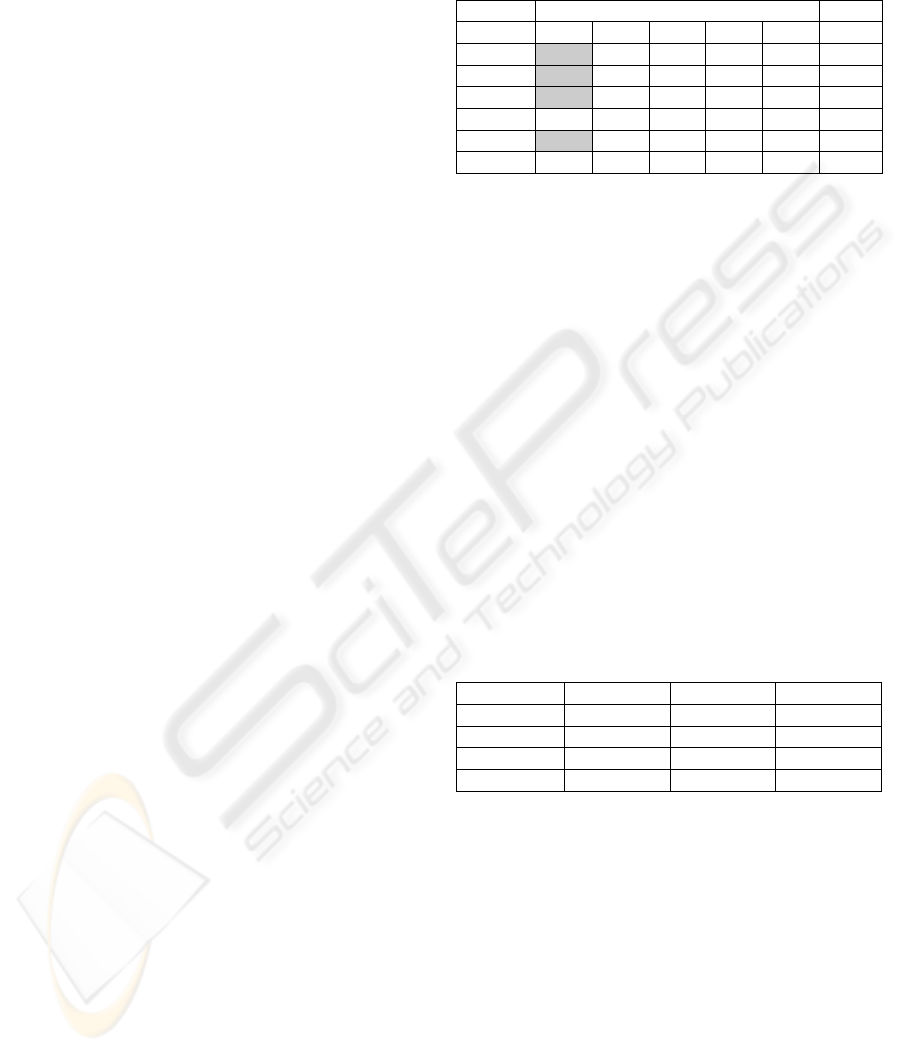
Data Collection. All test sessions were recorded
using video cameras and a microphone. The videos
showed the HCS screen and a small picture in
picture with the user’s face, see Figure 3. We
recorded a total of four hours of video. Two loggers
made written log files during the tests.
Figure 3: A test participant and the test monitor. The
picture is from the video recording. The small picture in
the upper right hand corner shows the interaction.
Data Analysis. The data analysis was carried out
separately applying two different analysis methods:
Video Based Analysis (VBA) and Instant Data
Analysis (IDA), see the following two subsections.
The purpose of using two methods was to get as rich
and extensive a problem list as possible. Each team
employed the procedure described below.
The problem lists from the VBA and IDA
analysis were merged into a total list of identified
usability problems. The test monitor and the data
logger from IDA and the three evaluators from VBA
did this. Disagreements were discussed until
consensus was reached. In cases where the VBA and
IDA lists did not have the same categorization for a
particular problem, the proper categorization was
discussed until agreement was reached. In this
process, some problems were split into more
detailed problems or merged with other problems.
2.2 Video-based Analysis (VBA)
The Video-Based Analysis was conducted in
accordance with Rubin (1994). The three evaluators
HEALTHINF 2010 - International Conference on Health Informatics
304
analysed the video material individually and made a
list of identified usability problems. The severity of
each problem was also categorised as either
“critical”, “serious” or “cosmetic” (Molich, 2000).
The three lists of usability problems were
discussed in the team and merged into one list of
VBA problems. When there was disagreement or
doubt whether problems should be combined or
split, or how they should be categorized, the video
material was reviewed and discussed until
agreement was reached. This included agreement
about the test subjects who experienced each
problem. To measure the evaluator effect, we
calculated the any-two agreement. The result was
40.2%, which is well above the minimum of 6% and
close to the 42% maximum found in other studies
(Hertzum and Jacobsen, 2003).
2.3 Instant Data Analysis (IDA)
The test monitor, one of the data loggers and a
facilitator, who did not observe the tests, conducted
this analysis immediately after all test sessions were
completed. The analysis was conducted according to
the IDA method (Kjeldskov et al., 2004).
The IDA analysis involved three steps:
brainstorm, task review and note review. During
these steps, the facilitator noted and organized all
usability problems on the whiteboard as they were
identified by the test monitor and the logger. After
completing the third step, the problems were
categorized as “critical”, “serious” or “cosmetic”
with the same definition as in the VBA analysis.
Finally, the test monitor and logger left, and the
facilitator wrote up the list of usability problems
from the notes on the whiteboard. The list was
validated and corrected by the test monitor and data
logger the following day.
3 RESULTS
This section describes the usability problems we
identified in the evaluation of the HCS device.
3.1 Task Completion Time and Rate
Table 2 provides an overview of the time it took
participants to complete each task. A grey cell
indicates that a particular participant was unable to
solve this task on his/her own and therefore received
significant help from the test monitor; this is referred
to as task completion rate. All users spent more time
completing task 1 (connection and installation)
compared to any other task, and 4 out of the 5 users
could not complete this task without help.
Table 2: Task completion time and completion rate.
Task
User 1 2 3 4 5 Total
1
33:25 10:10 08:47 07:37 01:15 1:01:14
2
33:44 09:34 04:30 04:54 01:00 53:42
3
28:25 02:26 02:45 05:08 01:24 40:08
4
18:43 02:43 04:24 04:07 01:19 31:16
5
26:05 01:06 03:31 04:45 00:41 36:08
Average
28:09 05:12 05:35 05:18 01:08 45:22
There are noticeable differences between the
time each participants spent on completing the other
four tasks. For task 2, the time varies between 1 and
10 minutes. If a user is facing problems, it is very
difficult to recover. For tasks 3, there is almost a
similar variation. For tasks 4 and 5, there is very
little variation. Tasks 2 and 4 are the same except
that task 2 is with a wired device, while task 4 is
with a wireless device. The difference may be due to
the wireless connection, however there may also be
a learning effect from task 2 to 4.
3.2 Identified Usability Problems
Table 3 shows the number of critical, serious and
cosmetic problems identified using the VBA and
IDA evaluation methods. By merging the VBA and
IDA problem lists we identified a total of 51
usability problems.
Table 3: Number of identified usability problems.
VBA IDA Total
Critical
14 15 14
Serious
15 13 15
Cosmetic
18 7 20
Total
47 35 51
3.3 Usability Themes
To get a better understanding of the different types
of usability problems, we have categorized them in
terms of 12 different usability themes. Below, we
briefly explain the meaning of each theme based on
Nielsen et al. (2006).
Affordance relates to issues on the users
perception versus the actual properties of an object
or interface.
Cognitive load regards the cognitive efforts
necessary to use the system.
Consistency concerns the consistency in labels,
icons, layout, wording, commands etc. on the
different screens.
USABILITY PROBLEMS IN A HOME TELEMEDICINE SYSTEM
305
Ergonomics covers issues related to the physical
properties of interaction.
Feedback regards the manner in which the
interface relays information back to the user on an
action that has been done and notifications about
system events.
Information covers the understandability and
amount of information presented by the interface at
a given moment.
Interaction styles concerns the design strategy
and determines the structure of interactive resources
in the interface.
Mapping is about the way in which controls and
displays correlate to natural mappings and should
ideally mimic physical analogies and cultural
standards.
Navigation regards the way in which the users
navigate from screen to screen in the interface.
Task flow relates to the order of steps in which
tasks ought to be conducted.
User’s mental model covers problems where
the interactive model, developed by the user during
system use, does not correlate with the actual model
applied in the interface.
Visibility regards the ease with which users are
able to perceive the available interactive resources at
a given time.
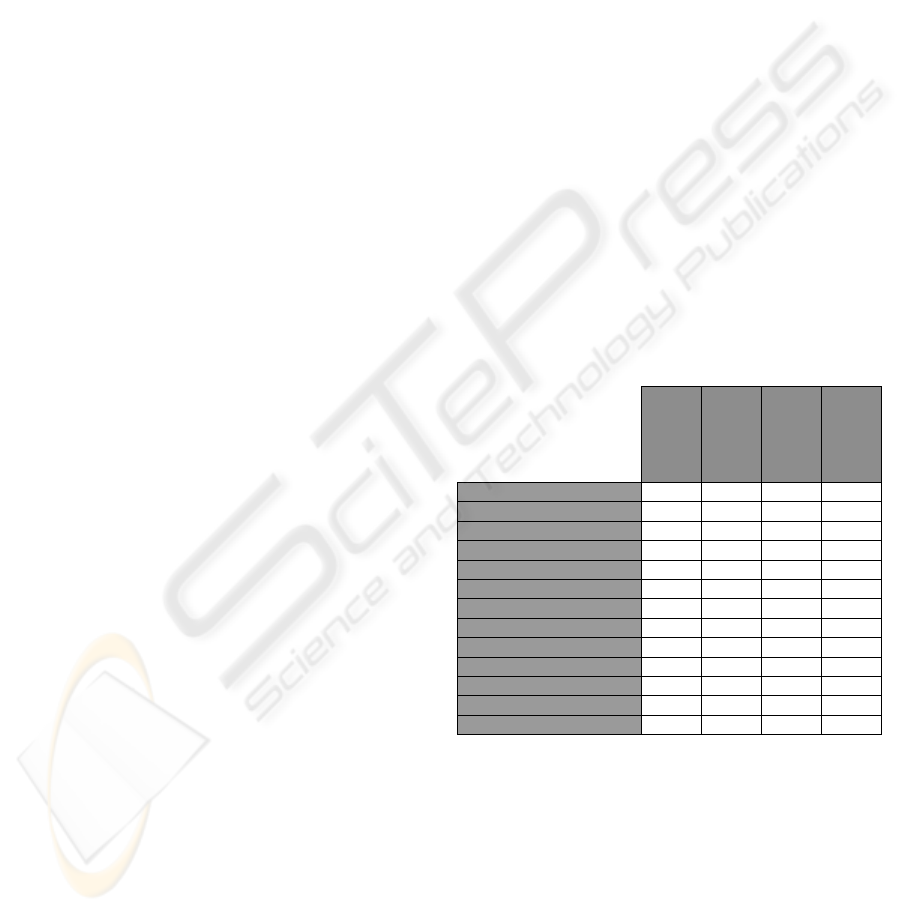
3.4 Distribution of Identified Problems
Table 4 shows the total number of identified
usability problems distributed on usability themes
and severity ratings. This shows that the users
experienced problems from almost all categories,
except cognitive load and interaction style.
The highest numbers of problems relate to
information and user’s mental model which account
for 17 and 10 problems respectively. Collectively
these themes include 53 % of all identified usability
problems of which 7 are critical, 11 serious and 9
cosmetic. The remaining 10 problems (20 %) relate
to the themes affordance (4), consistency (1),
ergonomics (2), mapping (1), navigation (1) and task
flow (1).
One of the problems related to the information
theme concerned the user manual, which illustrates
two possible ways of connecting the HCS to the
phone line. In the manual layout, the illustrations
were placed on opposite sides of an A5 brochure,
which some of the participants interpreted as a
sequence of steps. This resulted in some participants
trying to connect the device like in the first picture
and afterwards connecting the HCS as described by
the second illustration.
A problem related to the user’s mental model
was identified during connection of the Bluetooth
scale where participants were looking for a cable to
connect this to the HCS, thereby exhibiting that they
did not know how to connect these two devices.
14 problems relate to the themes feedback and
visibility (7 in each theme) and account for 27 % of
the total number of problems. 4 of these problems
are critical, 3 serious and 7 cosmetic.
One of the problems with missing feedback was
identified when participants had answered all of the
pre-programmed questions. When the questions
were completed, the display showed the idle screen
with the company logo and did not provide feedback
to the users of whether they were finished or not.
This resulted in some of the users looking for a way
to finish and others thought they needed to answer
more questions.
A visibility related issue concerned the volume
buttons on the HCS. A participant wanted to
manipulate the volume and could not find the button,
and therefore he tried pressing all other buttons on
the device (“Y”, “N”, up and down) but with no
result.
Table 4: Total number of identified problems distributed
according to usability themes and severity.
Critical
Serious
Cosmetic
Total
Affordance
2 2 4
Cognitive load
Consistency
1 1
Ergonomics
2 2
Feedback
1 3 3 7
Information
5 8 4 17
Interaction style
Mapping
1 1
Navigation
1 1
Task flow
1 1
User’s mental model
2 3 5 10
Visibility
3 4 7
Total
14 15 20 51
3.5 Connection and Installation
As illustrated in Table 2 above, the task completion
times and completion rates indicate that connection
and installation of the HCS (task 1) was particularly
tedious and problematic.
Table 5 shows the distribution of usability
problems on themes, but only for task 1. Thus it
represents a subset of the numbers in Table 4. This
illustrates that 32 of the 51 problems (63 %) were
identified during connection and installation of the
HEALTHINF 2010 - International Conference on Health Informatics
306
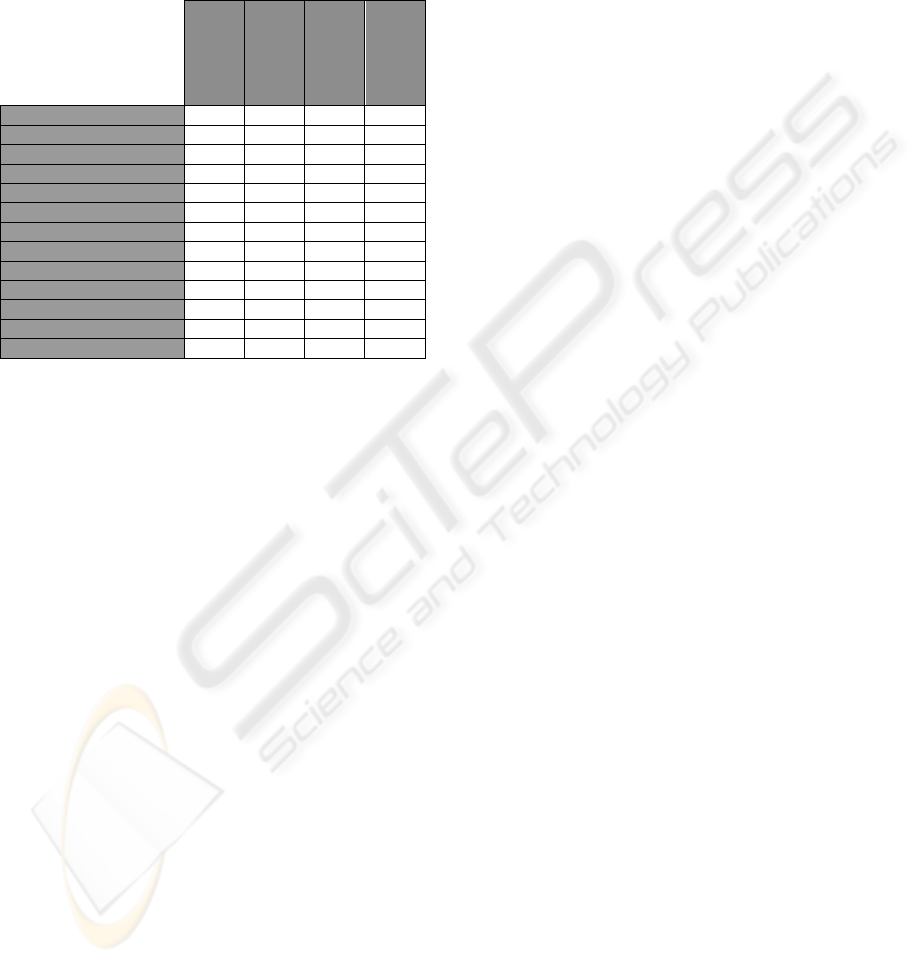
device (task 1). Almost all critical and serious
problems were found during this task where 11
usability problems out of a total of 14 (79 %) are
critical, 12 out of 15 (80 %) serious and 9 out of 20
(45 %) cosmetic.
Table 5: Identified problems related to task 1: connecting
and installing the device.
Critical
Serious
Cosmetic
Total
Affordance
1 1 2
Cognitive load
Consistency
Ergonomics
1 1
Feedback
1 1 1 3
Information
3 8 4 15
Interaction style
Mapping
1 1
Navigation
1 1
Task flow
User’s mental model
2 2 2 6
Visibility
3 3
Total
11 12 9 32
For this task, most problems also relate to
information and user’s mental model. The 15
problems with information contain all serious and
cosmetic instances and 3 of the total of 5 critical
problems were observed in task 1. When considering
the 6 problems related to the user’s mental model,
we found that all critical (2) and almost all serious
problems (2 of 3) were encountered in task 1.
The rest of the 11 problems identified in task 1
were distributed on affordance (2), ergonomics (1),
feedback (3), mapping (1), navigation (1) and
visibility (3). It is worth noting that all critical
problems relating to these themes were observed in
task 1.
As an example of an information-related
problem in task 1, most of the participants did not
understand the text “Detecting phone line” displayed
during setup. This resulted in several participants
lifting the nearby phone receiver and pressing
various buttons on the HCS.
Another example regarding information was the
term “Line”, which was represented on the back of
the device and in the manual, but it made no sense to
the participants.
One of the problems regarding the user’s mental
model was when the users, in order to install the
HCS, had to connect a cable from the phone line in
the wall to the correct port on the HCS device in
order to communicate with the remote server.
However, the participants did not know which cable
to use and some mistakenly tried to connect the
phone and the HCS.
Another problem concerning the user’s mental
model was identified when the system asked the user
to input a phone line prefix to bypass local in-
building phone numbers. In our case, the users
needed to press “0” as prefix in order to make the
HCS able to communicate with a server outside the
building. This prefix had to be selected on the HCS,
but some participants pressed “0” on the phone with
no result.
3.6 Qualitative Interviews
As part of the usability evaluation, we conducted a
post-test interview with each user. The users
emphasized that they “felt there were too many
devices and cords that needed to be connected
before the HCS was operational”. It was also stated
that the printed manual should be “redesigned and
include more and better illustrations like the ones
known from Lego and Ikea manuals”.
Comments about technical lingo emphasized that
words like “Detecting” and “Initializing” were
unknown to the participants. Some also expressed
that they needed more system feedback on what to
do;, one of the participants said: “When the device
does this and that, I need further instructions on how
to respond”. The missing feature to enable the user
to undo an action was commented by some of the
participants; one stated that “I pressed the wrong
button when setting the date, but I was unable to go
back and correct the error”.
The interviews also revealed issues not identified
during data analysis of usability problems. Most
participants noted that they received no information
about when and how the HCS was sending results to
the hospital or care center. They were unsure
whether the results were sent automatically or not.
The fonts on the display were perceived as clear
and easy to read, however, some participants
expressed that the soft menus (menus placed in the
bottom area of the display mapping to the “Y” and
“N” buttons, see Figure 1) where hard to read. This
was caused by the relatively steep edge connecting
the plastic cover and the display. The participants
felt that they had to move closer to the device when
reading the soft menu texts.
On the positive side all participants said that the
HCS had good potential. Some expressed “Once the
system is connected it would be easy to use”. They
would all prefer to use this type of device compared
to hospital visits.
USABILITY PROBLEMS IN A HOME TELEMEDICINE SYSTEM
307

4 DISCUSSION
In this section we discuss our findings in relation to
other studies with usability evaluation of health care
systems.
We have found one previous evaluation of a
system for use by patients. This is Kaufman et al.
(2003) who asked their users to solve the following
tasks using a home telemedicine unit (HTU):
Measure glucose level, make blood pressure
readings, access an educational website, send an
email and change the calendar. These tasks differ
partly from our study, but there is an overlap in the
blood glucose reading task. Although most tasks
differed, we identified some similar problems. They
identified problems related to unnecessarily complex
tasks, which can be compared to the problems we
found during connection and installation of the HCS.
Their study also revealed problems concerning non-
transparent screen transitions, which are comparable
to our problems with missing feedback. We
experienced system crashes and restarts that
frustrated several participants, and they noted issues
regarding system instability. Information-related
problems were experienced both in their study,
where the users did not understand the blood
pressure expression “212/89” referring to the
systolic and diastolic values, and in our study the
users also experienced such problems, e.g. they did
understand the terms “initializing” and “detecting”.
Mapping problems were also found in both studies.
Their users could not establish a correspondence
between a set of numbers presented one way on the
blood pressure meter and another way in the PC
application. In our case the users could not establish
a connection between illustrations in the manual and
the actual layout of the physical system. Finally,
both studies identified issues related to the user’s
mental model and visibility.
Kaufman et al. (2003) conducted a nonverbal
analysis through comprehensive microanalysis,
which provided further evidence on participant
experiences. As noted in the paper, nonverbal
analysis is especially useful in situations where
indexicality is challenging, e.g. where the users lack
a clear vocabulary when referencing interface
objects like “scroll bar”, “drop down menu”, “check
box”, “radio button” etc. This type of microanalysis
is important in order to cover as many usability
problems as possible. Yet it is also extremely time
consuming and expensive, which is acknowledged
by the authors.
There is a number of studies that focus on
usability evaluation of systems designed for use by
medical staff (Kushniruk et al., 1996; Kushniruk and
Patel, 2004; Kushniruk et al., 2005). In these studies,
the usability problems they have identified are
distributed over a set of usability themes with
various levels of abstraction ranging from
information content, procedure (task flow),
comprehension of graphics and text (user’s mental
model) and overall system understandability to data
entry and printing. The results from these studies
confirm that information-related problems were
observed in all of these. However, the percentage of
information-related problems differs considerably
from our study, where it is considerably higher. In
Kushniruk et al. (2005) 16% of the identified
problems are information related, while the number
is 7% in Kushniruk and Patel (2004) and Kushniruk
et al. (1996) (these are based on the same
experiment). In our results, 33% of the identified
problems were information related. For problems
regarding the user’s mental model (comprehension)
Kushniruk et al. (1996) observed 5% in this
category. In our study this was 20%, thus we
observed a relatively higher amount of this type of
usability problem. In Kushniruk et al. (2005) and
Kushniruk et al. (1996) the researchers found task
flow related problems (procedure/operation
sequence to be 15% and 6% respectively. Our study
showed a lower percentage of 2% regarding task
flow issues. The majority of issues identified in
Kushniruk et al. (2005) were visibility related with a
higher percentage of 26% compared to the 14% in
our study. Thus, considering usability themes from
systems designed for medical professionals, we
identified a relatively high number of information
related problems. This is also the case for problems
concerning the user’s mental model. On the other
hand we observed a relatively low number of task
flow and visibility related issues.
5 CONCLUSIONS
In this paper, we have presented results from a
usability evaluation of a home telemedicine system.
The purpose of this was to emphasize key problems
that designers of such systems should be aware of.
We identified the major usability problems to be
within these five categories: Difficult to connect and
install the system, the information provided is
difficult to understand, the system does not conform
to the user’s mental model, the feedback is
insufficient and the resources of the system are not
visible to the user.
This result is restricted in the sense that it is
based on a usability evaluation of a single system
with five users. However, we have compared our
HEALTHINF 2010 - International Conference on Health Informatics
308

results to the limited number of related research
results. We found a single evaluation of a system
targeted at patients, like the one we have evaluated,
and there are a few evaluations of systems targeted
at medical staff. Both types of evaluations confirm
the key problems we have identified.
This study has uncovered a surprisingly high
number of usability problems given that the system
has a fairly simple functionality. It would be
interesting to conduct usability evaluations of other
systems targeted at patients, in particular of more
complex systems. It seems like the challenges for
designers of home telemedicine systems are
significant.
REFERENCES
Eikerling, H-J., et al., 2009. Ambient Healthcare Systems -
Using the Hydra Embedded Middleware for Implementing
an Ambient Disease Management System. In
Proceedings of the Second International Conference
on Health Informatics. INSTICC Press.
Fensli, R., Boisen, E., 2008. Human Factors Affecting the
Patient’s Acceptance of Wireless Biomedical Sensors. In
Biomedical Engineering Systems and Technologies,
International Joint Conference. Springer. INSTICC
Press.
Fisk AD, Rogers WA, 2002. Health Care of Older Adults:
The Promise of Human Factors Research. In Human
factors interventions for the healthcare of older adults.
Lawrence Erlbaum.
Ginsburg, G., 2004. Human Factors Engineering:A Tool
for Medical Device Evaluation on Hospital
Procurement Decision-Making. In Journal of
Biomedical Informatics. Elsevier.
Hertzum, M. and Jacobsen, N. E.., 2003 The Evaluator
Effect: A Chilling Fact About Usability Evaluation
Methods. In International Journal of Human
Computer Interaction. Taylor & Francis.
Jaana M., Paré, G., 2006. Home Telemonitoring of
Patients with Diabetes: A Systematic Assesment of
Observed Effects. In Journal of Evaluation in Clinical
Practice. Blackwell Publishing.
Johnson, C. M., et al., 2004. A User-Centered Framework
for Redesigning Health Care Interfaces. In Journal of
Biomedical Informatics, Elsevier.
Kaufman, D. R., et al., 2003. Usability in the Real World:
Assessing Medical Information Technologies in
Patient’s Homes. In Journal of Biomedical
Informatics, Elsevier.
Kjeldskov, J., et al., 2004. Instant Data Analysis:
Evaluating Usability in a Day. In Proceedings of
NordiCHI 2004. ACM Press.
Kushniruk, A. W., et al., 1996. Cognitive Evaluation of
the User Interface and Vocabulary of an Outpatient
Information System. In Proceedings of AMIA Annual
Fall Symposium.
Kushniruk, A.W., et al., 2005. Technology Induced Error
and Usability: The Relationship Between Usability
Problems and Prescription Errors When Using a
Handheld Application. In International Journal of
Medical Informatics, Elsevier.
Kushniruk, A.W., Patel, V. L., 2004. Cognitive and
Usability Engineering Methods for the Evaluation of
Clinical Information Systems. In International Journal
of Medical Informatics, Elsevier.
Linder, J. A., et al., 2006. Decision support for acute
problems: The role of the standardized patient in usability
testing. In Journal of Biomedical Informatics.
Elsevier.
Molich, R., 2000. User-Friendly Web Design (in Danish),
Ingeniøren Books. Copenhagen.
Nielsen, C. M., et al., 2006. It’s Worth the Hassle! The
Added Value of Evaluating the Usability of Mobile
Systems in the Field. In
Proceedings of NordiCHI.
ACM Press.
Nielsen, J., 1993. Usability Engineering. Morgan
Kaufmann. San Diego.
Nielsen, J. and Landauer, TK, 1993. A mathematical
model of the finding of usability problems. In
Proceedings of the SIGCHI conference on Human
factors in computing systems. ACM Press.
Pascual, J., et al., 2008. Intelligent System for Assisting
Elderly People at Home. In Proceedings of the First
International Conference on Health Informatics.
INSTICC press.
Peleg, M., et al., 2009. Using Multi-Perspective
Methodologies to Study Users’ Interactions with the
Prototype Front End of a Guideline-Based Decision
Support System for Diabetic Foot Care. In
International Journal of Medical Informatics,
Elsevier.
Peute, L.W., Jaspers, M.W., 2007. The significance of a
usability evaluation of an emerging laboratory order
entry system. In International Journal of Medical
Informatics, Elsevier.
Rubin, J., 1994. Handbook of Usability Testing, John
Wiley & Sons. New York.
Taleb, T., et al., 2009. ANGELAH: A Framework for
Assisting Elders at Home. In IEEE journal on selected
areas in communications. IEEE.
Sasaki, J., et al., 2009. Experiments of Life Monitoring
Systems for Elderly People Living in Rural Areas. In
Proceedings of the Second International Conference
on Health Informatics. INSTICC Press.
Sashima, A., et al., 2008. Toward Mobile Healthcare
Services by Using Everyday Mobile Phones. In
Proceedings of the First International Conference on
Health Informatics. INSTICC Press.
Souidene W., et al., 2009. Multi-Modal Platform for In-
Home Healthcare Monitoring (EMUTEM). In
Proceedings of the Second International Conference
on Health Informatics. INSTICC Press.
United Nations, 2006. World Population Prospects.
Dept of Economic and Social Affairs. Obtained at:
http://www.un.org/-esa/population/publications/-
wpp2006/-WPP2006_Higlights_rev.pdf (downloaded
august 20, 2009).
USABILITY PROBLEMS IN A HOME TELEMEDICINE SYSTEM
309
